pISSN : 3058-423X eISSN: 3058-4302
Open Access, Peer-reviewed
pISSN : 3058-423X eISSN: 3058-4302
Open Access, Peer-reviewed
Weon Ju Lee,Dong Hyuk Eun,Jun Hong Park,Yong Hyun Jang,Seok-Jong Lee,Do Won Kim,Yong Jun Bang,Jae Bok Jun
http://dx.doi.org/10.17966/KJMM.2017.22.3.141 Epub 2017 September 29
Abstract
Keywords
Chromoblastomycosis Dermatophyte Dermatophytosis Fonsecaea Fonsecaea monophora
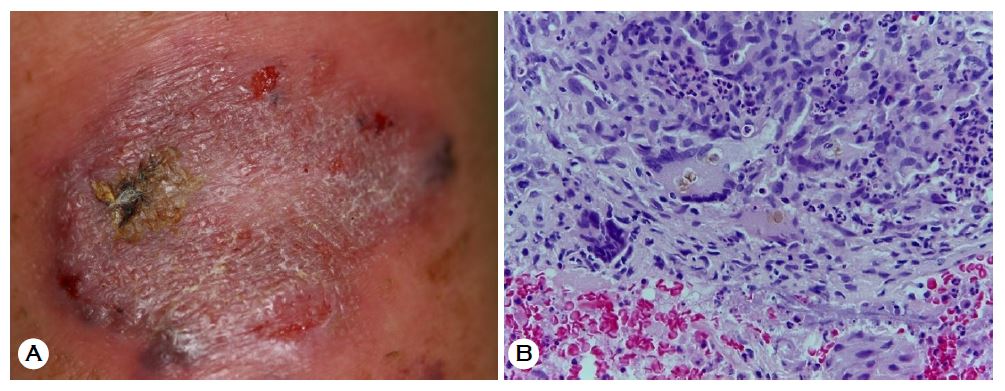
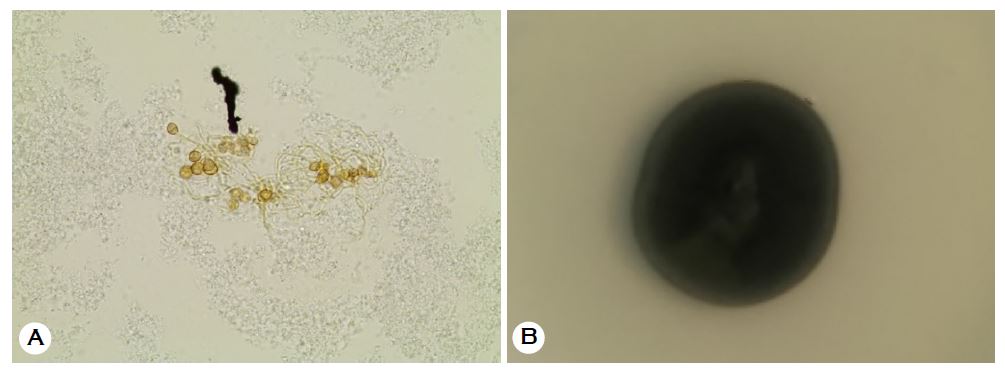
A 65-year-old male patient presented with a walnut-sized, scaly erythematous plaque on the left forearm for 1 year (Fig. 1A). He had been taking antihypertensive agents. He was diagnosed with chromoblastomycosis caused by Fonsecaea monophora by using biopsy, KOH preparation, fungal culture, lactophenol cotton blue staining, and DNA gene sequencing. Histopathology showed brownish sclerotic bodies and a mixed inflammatory and granulomatous infiltrate in the dermis (Fig. 1B). KOH preparation showed brown sclerotic bodies (Fig. 2A). Fungal culture showed dark black, velvety colonies (Fig. 2B). Long, septate hyphae with numerous conidia were observed on lactophenol cotton blue staining. Sequencing analysis of the internal transcribed spacer (ITS) region of ribosomal DNA (rDNA) using Gapped Basic Local Alignment Search Tool (BLAST) and Position-Specific Iterated (PSI)-BLAST in GenBank identified F. monophora. Gene sequencing revealed 100% homology with accession number AB091204. The chromoblastomycosis was controlled by taking oral antifungal medication (itraconazole 100 mg twice a day for 2 months).
Deep mycosis caused by dematiaceous fungi is roughly subdivided into three types: chromoblastomycosis, black-grain mycetoma, and phaeohyphomycosis. F. pedrosoi, which is a major dematiaceous fungus, accounts for 90% of chromoblastomycosis. Fonsecaea has been reclassified using rDNA ITS sequence analysis: F. pedrosoi, F. monophora, and others[1]. Our case had chromomycosis caused by F. monophora that had developed on the left forearm. F. monophora could not be identified through morphological examination, but was confirmed using rDNA ITS sequence analysis. Occasionally, sclerotic cells on KOH preparation and histopathological examination can be helpful in making a diagnosis of chromoblastomycosis caused by F. monophora[2]. Chromoblastomycosis can be successfully treated with physical modalities, chemotherapy, and/or combination therapy[3]. In Korea, 4 cases of F. monophora chromoblastomycosis have been reported. Kim et al.[4] reported a case in 2014, and the others were reclassified phylogenetically as F. monophora by Lim et al.[5] in 2010. Nevertheless, chromoblastomycosis caused by F. monophora is very rare in Korea. We describe a case of F. monophora chromoblastomycosis identified with gene sequencing analysis.
References
1. De Hoog GS, Attili-Angelis D, Vicente VA, Van Den Ende AH, Queiroz-Telles F. Molecular ecology and pathogenic potential of Fonsecaea species. Med Mycol 2004;42:405-416
Google Scholar
2. Queiroz-Telles F, Esterre P, Perez-Blanco M, Vitale RG, Salgado CG, Bonifaz A. Chromoblastomycosis: an overview of clinical manifestations, diagnosis and treatment. Med Mycol 2009;47:3-15
Crossref
Google Scholar
3. Lu S, Lu C, Zhang J, Hu Y, Li X, Xi L. Chromoblasto- mycosis in Mainland China: a systematic review on clinical characteristics. Mycopathologia 2013;175: 489-495
Crossref
Google Scholar
4. Kim BS, Choi JH, Sohng SH, Shin DH, Choi JS, Suh MK. Chromoblastomycosis caused by Fonsecaea monophora. Korean J Med Mycol 2014;19:18-24
Google Scholar
5. Lim SW, Suh MK, Kang GS, Ha GY, Kim H, Choi JS, et al. Molecular phylogenetics of Fonsecaea strains isolated from chromoblastomycosis patients in South Korea. Mycoses 2010;54:415-420
Crossref
Google Scholar
