pISSN : 3058-423X eISSN: 3058-4302
Open Access, Peer-reviewed
pISSN : 3058-423X eISSN: 3058-4302
Open Access, Peer-reviewed

Joon Goon Kim,Hye Ri Kim,Moon Hyung You,Dong Hoon Shin,Jong Soo Choi
10.17966/JMI.2018.23.2.54 Epub 2018 July 01
Abstract
Typically, sporotrichosis follows an environmental transmission route via traumatic inoculation of contaminated plant or soil matter. Although familial occurrences of sporotrichosis are rare, human-to-human transmission is even rarer. Herein, we report two cases, a father and son, with sporotrichosis caused by Sporothrix (S.) globosa. A 33-year-old male who otherwise appeared healthy presented with a tender, erythematous, ulcerative crusted plaque on the left ala nasi and upper lip. A skin biopsy and mycological study revealed fixed cutaneous sporotrichosis. The patient irregularly received oral itraconazole with a relapsing course. Approximately a year later, his 3-year-old son developed a single plaque on the left leg. When the father carried his son on his shoulder, there was direct contact between the two lesions. Fungal culture results from the father and son's lesions confirmed S. globosa with ribosomal DNA ITS sequencing. In both patients, oral terbinafine exhibited better results than oral itraconazole. These cases are an excellent example of human-to-human transmission of sporotrichosis.
Keywords
Human-to-human transmission Sporothrix globosa Sporotrichosis
Sporotrichosis is the leading subcutaneous mycosis caused by the Sporothrix (S.) schenckii complex. With the development of molecular biology methods, Marimon et al.1 reported that the S. schenckii complex comprises six species as follows: S. globosa, S. brasiliensis, S. luriei, S. mexicana, and S. pallida (S. albicans). Of these, S. globosa infection is primarily found in East Asia2. Kim et al.3 reported that S. globosa is the causative organism of fixed sporotrichosis in Korea and proposed that S. globosa might be the only causative agent of sporotrichosis in Korea. Typically, S. globosa propagates through plant-transmitted infection4, and human-to-human transmission is not well reported. Although cases of familial sporotrichosis have been occasionally reported, in most cases, the suspected source of infection was shared, and human-to-human transmission was extremely rare. Here, we report two cases of sporotrichosis due to S. globosa resulting from human-to-human transmission.
1. Case 1
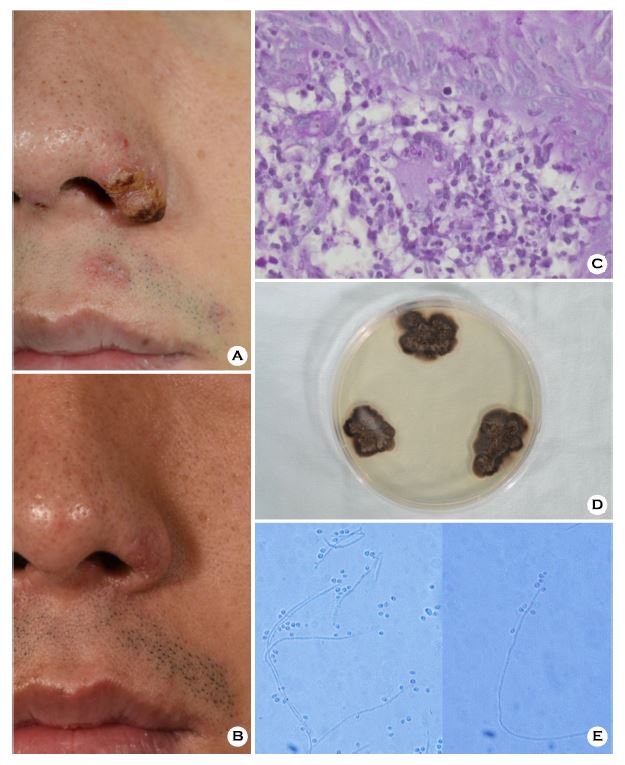
A 33-year-old male presented with a yellow-brown verrucous nodule on the left ala nasi (size, 0.8 × 1 cm; Figure 1A). The lesion developed in the form of a blister on the left side of the nose 3 years ago, which slowly increased in size, and was treated with topical steroids in a clinic; however, it worsened without improvement. The patient was in good health and denied any medications that affected his immune status.
The KOH preparation test performed on the skin lesions was negative. We performed a histological examination and cultured part of the specimen. Histologically, we observed chronic inflammatory granuloma comprising lymphocytes, histiocytes, and giant cells in H&E staining and several spores with periodic acid-Schiff (PAS) staining (Figure 1C). In addition, some parts of the biopsy specimen of the lesion were inoculated on Sabouraud's dextrose agar and cultured at 25℃; in 2 weeks, a grayish, dark-brown colony was observed (Figure 1D). In the slide culture, conidia were developing from con- idiogenous cells in a group or alongside the hyphae alone. Conidia were single-celled, tear-shaped, clavate or oval-shaped, and haline (Figure 1E). Furthermore, BLAST® search revealed 100% similarity between nucleotide sequences of conidia and S. globosa (GenBank® accession number: MH499862). While skin lesions improved with the use of systemic antifungal agents (itraconazole, 100 mg BID; Figure 1B), the symptoms recurred upon discontinuing the medication. Hence, we switched the medication to terbinafine, which was more effective.
2. Case 2
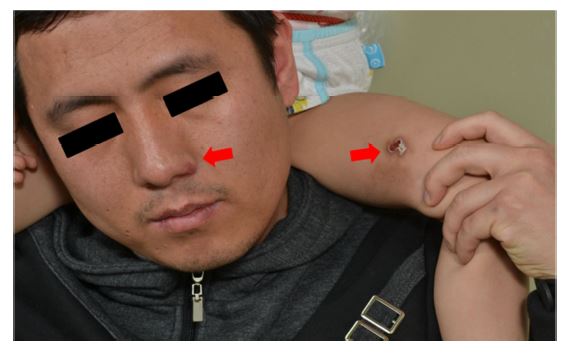
A 3-year-old male presented with a 2- × 2-cm ulcer on the left inner thigh (Figure 2A). Initially, the lesion developed in the form of a blister on the left inner thigh a year ago, but it slowly increased in size; although it was treated in a clinic, it worsened without improvement. Two years ago, the patient's father was diagnosed with sporotrichosis. The family denied having any pets or growing plants. The child's mother, who shared a room with the patient, exhibited no skin symptoms. In the shoulder ride position that the father-son duo often enjoyed, a direct contact occurred between the father and son's lesions (Figure 3). Notably, no fungus was noted in the KOH preparation test. A skin biopsy revealed chronic inflammatory granuloma; we observed multiple spores in the PAS and Gomori methenamine silver staining (Figure 2C). In addition, biopsy specimens were inoculated on Sabouraud's dextrose agar and incubated for 2 weeks at 25℃, displaying a grayish, dark-brown colony of fungi similar to the results of the father's fungal culture. The isolated primary colony was identified as S. globosa by the ribosomal DNA ITS sequencing (GenBank® accession number: MH499863). After sporotrichosis diagnosis, the patient received a systemic antifungal agent (itraconazole, 100 mg QD) for a year. The lesion exhibited gradual improve- ment but worsened upon discontinuing the drug. After switching to oral terbinafine, the patient exhibited better response (Figure 2B).

3. Mycological study
Both strains did not grow at 37℃, and were susceptible to terbinafine (MIC 0.125 μg/ml), and resistant to itraconazole (MIC >16 μg/ml) and voriconazole (MIC >16 μg/ml).
Sporotrichosis, which commonly occurs in mammals, has two major transmission pathways: via animals and plants. Both routes involve impairment of the skin or subcutaneous tissue by trauma and injection of Sporothrix propagules into the skin. Skin lesions occur at the site of inoculation, and localized propagation might occur along the lymphatic path- way during the first 2~3 weeks of infection5. Typically, S. schenckii and S. globosa are spread by infection from contaminated plants; however, S. brasiliensis is mostly transmitted by scratch wounds caused by infected felines4.
In our cases, the family was living in an urban area with no home-grown plants, and the father was not working as a farmer. Thus, in the case of the son, we could exclude trans- mission via plants. In addition, the father and son's lesions did not simultaneously develop. The father intermittently received the medication as he was first diagnosed with sporotrichosis. The father informed that he often carried his son on his shoulders. In the shoulder ride position, we observed a direct contact between the father and son's lesions (Figure 3). Presumably, the son might have had unrecognizable trauma, which induced infection of Sporothrix from the father's lesion. Reportedly, the inoculum load, host immune status, virulence of the inoculated strain, and inoculation depth are involved in the clinical manifestations of sporotrichosis6. The host is resistant to the strain primarily by cell-mediated immunity. When a human is infected by a Sporothrix spp., suppurative granuloma formation with scanty fungal elements is usually observed on H&E staining. Perhaps, this potent immune response could explain the less human-to-human transmission of Sporothrix spp.
Considering the frequency of contact, there is a high possibility of sporadic spread of Sporothrix spp. in sporotrichosis occurring in the family. To date, 22 familial cases of sporotrichosis have been reported worldwide7-11; of these, 17 were not related with animal transmission, which is not the usual transmission pathway of S. globosa. However, only three cases could be suspected because of human-to-human transmission while considering the temporal order, occupation, and frequency of contact among patients12-14. Moreover, none of the three cases presented the exact species because when these were reported, the S. schenckii complex was only classified as S. schenckii in the absence of a molecular technique. Thus, if human-to-human transmission of sporotrichosis is suspected, detecting the correct species by a molecular method will help the epidemiological study of sporotrichosis.
In our cases, several fungal elements were observed in the histological examination, itraconazole was ineffective, and a repetitive contact occurred between the father and the son — all contributing to the human-to-human transmission of S. globosa. In addition, the patients might have a genetic predisposition or susceptibility to Sporothrix. Hence, as S. schenckii is transmitted by felines in Malaysia, the possibility of S. globosa transmission by animals or humans should be carefully observed15.
In relation to this article, I declare that there is no conflict of interest.
References
1. Marimon R, Cano J, Gené J, Sutton DA, Kawasaki M, Guarro J. Sporothrix brasiliensis, S. globosa, and S. mexicana, three new Sporothrix species of clinical interest. J Clin Microbiol 2007;45:3198-3206
Crossref
Google Scholar
2. Chakrabarti A, Bonifaz A, Gutierrez-Galhardo MC, Mochizuki T, Li S. Global epidemiology of sporotrichosis. Med Mycol 2015;53:3-14
Crossref
Google Scholar
PubMed
3. Kim JG, You MH, Kim YW, Kim BS, Shin DH, Choi JS, et al. A case of fixed cutaneous sporotrichosis caused by Sporothrix globosa on the face. Korean J Med Mycol 2016; 21:52-58
Crossref
Google Scholar
4. Gremião ID, Menezes RC, Schubach TM, Figueiredo AB, Cavalcanti MC, Pereira SA. Feline sporotrichosis: epidemio- logical and clinical aspects. Med Mycol 2015;53:15-21
Crossref
PubMed
5. Orofino-Costa R, de Macedo PM, Bernardes-Engemann AR. Hyperendemia of sporotrichosis in the Brazilian Southeast: Learning from clinics and therapeutics. Curr Fungal Infect Rep 2015;9:220-228
Crossref
Google Scholar
6. Barros MB, de Almeida Paes R, Schubach AO. Sporothrix schenckii and sporotrichosis. Clin Microbiol Rev 2011;24: 633-654
Crossref
Google Scholar
PubMed
7. Frumkin A, Tisserand ME. Sporotrichosis in a father and son. J Am Acad Dermatol 1989;20:964-967
Crossref
Google Scholar
PubMed
8. Umemoto N, Demitsu T, Osawa M, Toda S, Kawasaki M, Mochizuki T. Sporotrichosis in a husband and wife. J Dermatol 2005;32:569-573
Crossref
Google Scholar
PubMed
9. Cordeiro FN, Bruno CB, Paula CD, Motta Jde O. Familial occurrence of zoonotic sporotrichosis. An Bras Dermatol 2011;86:S121-S124
Crossref
Google Scholar
PubMed
10. Falqueto A, Bravim Maifrede S, Araujo Ribeiro M. Unusual clinical presentation of sporotrichosis in three members of one family. Int J Dermatol 2012;51:434-438
Crossref
Google Scholar
11. Tsuji G, Takei K, Takahara M, Matsuda T, Nakahara T, Anzawa K, et al. Simultaneous onset of sporotrichosis in mother and daughter. J Dermatol 2017;44:1068-1069
Crossref
Google Scholar
PubMed
12. Smith LM. Sporotrichosis: Report of four clinically atypical cases. South Med J 1945;38:505-515
Crossref
Google Scholar
13. Murakami M, Yamada T, Kariya H. A case of sporotrichosis suspected to be herpes simplex. Hifubyo-Shinryo 1982;4: 319-322. (in Japanese)
Crossref
Google Scholar
14. Jin XZ, Zhang HD, Hiruma M, Yamamoto I. Mother-and¬child cases of sporotrichosis infection. Mycoses 1990;33: 33-36
Crossref
Google Scholar
15. Siew HH. The current status of feline sporotrichosis in Malaysia. Med Mycol J 2017;58:E107-E113
Crossref
Google Scholar
PubMed
Congratulatory MessageClick here!
