pISSN : 3058-423X eISSN: 3058-4302
Open Access, Peer-reviewed
pISSN : 3058-423X eISSN: 3058-4302
Open Access, Peer-reviewed

Sang-Jin Cheon,Ji Hyun Lee,Yang Won Lee,Joonsoo Park, Moo Kyu Suh,Hyojin Kim,Je-Ho Mun,Sung Yul Lee,Jong Soo Choi, Eung Ho Choi,Jee-Bum Lee,Jin Park,Hee Joon Yu, Hyun-Chang Ko
10.17966/JMI.2018.23.2.45 Epub 2018 July 01
Abstract
Background: Superficial dermatomycoses are fungal infections of the skin, hair, or nails and are most commonly caused by dermatophytes. Superficial dermatomycoses are very common diseases in the field of dermatology; however, their prevalence and clinical characteristics vary with geographical areas and populations. Moreover, pathogenic species change constantly over time.
Objective: This multicenter study aimed to investigate the epidemiologic and clinical findings of tinea corporis, tinea faciale, and tinea capitis in Korea during 2016-2017. In addition, we sought to identify the pathogenic organism causing these three different types of fungal infections.
Methods: Total 453 patients from the dermatology clinics of 13 tertiary hospitals in Korea were enrolled in this study. Information regarding demographic characteristics, comorbidities, occupation, family history of superficial dermatomycoses, suspected routes of infection, and treatment was collected. Fungal cultures and molecular analyses were performed for patients with tinea corporis, tinea faciale, and tinea capitis.
Results: Of the 453 patients, 275 were men and 178 were women. With respect to past history, 214 patients (53.4%) had at least one comorbidity. Tinea corporis (27.3%) was the most common form of superficial dermatomycosis, followed by tinea pedis (23.2%) and tinea unguium (16.6%). Overall, the fungal culture positivity was 77.8% (126/162). Trichophyton rubrum was the most common causative organism for tinea corporis (66.7%, 68/80) and tinea faciale (43.8%, 14/23), while Microsporum canis was the most common causative organism for tinea capitis (36.7%, 11/23).
Conclusion: Trichophyton rubrum was consistently the most common causative organism of superficial dermatomycoses, except for tinea capitis in Korea.
Keywords
Microsporum canis Superficial dermatomycoses Tinea capitis Tinea corporis Tinea faciale Trichophyton rubrum
The prevalence of superficial dermatomycoses is increasing, and the global prevalence is expected to reach 20~25%1. Various fungi, such as dermatophytes, yeasts, and nondermatophyte molds, cause superficial dermatomycoses; among these, dermatophytes are the most common cause of superficial dermatomycoses2.
The epidemiology and mycology of superficial dermatomycoses change with time and are influenced by bioclimatic condition, socioeconomic status, life environment, and immune status of individual members of the society. In Korea, the first nationwide epidemiological and mycological study was conducted in 19593. Thereafter, several authors have conducted studies to detect changes in superficial dermatomycoses. It has also been expected that clinical and mycological changes in fungal infections will occur in Korea owing to continuous industrialization and westernization. Investigation of the epidemiologic and mycologic findings of superficial dermatomycoses is essential for infection management and prevention. Therefore, we conducted a multicenter study on the epidemiology of superficial dermatomycoses and identified the organisms associated with superficial dermatomycoses in tertiary hospitals of Korea.
1. Patients
This multicenter study was conducted on patients with superficial dermatomycoses who were examined in the dermatology clinics at 13 tertiary hospitals in South Korea between July 2016 and May 2017. Patients with clinically suspected superficial dermatomycoses were assessed with the potassium hydroxide (KOH; 10%) examination to identify the presence of fungi. Patients with a positive KOH examination result were included in this study. At the initial visit, patients completed a case report form that required them to provide epidemiologic information, and mycologic evaluations were conducted in patients with tinea corporis, tinea faciale, and tinea capitis.
2. Epidemiologic study
The following epidemiologic data were collected using a well-structured case report form: age, sex, past history of comorbidities, family history of dermatomycoses, occupation, suspected route of infection, duration of disease, clinical diagnosis, and antifungal agent used for treating superficial dermatomycoses. Each category was subdivided, as shown in Table 1.
|
Category |
Subdivision |
|
Past history |
Liver disease: hepatitis, liver
cirrhosis, hepatocellular carcinoma, other liver diseases Diabetes mellitus Hypertension Dyslipidemia Tuberculosis Malignancy Immunosuppressive |
|
Family history |
Grandfather/grandmother Father/mother Son/daughter Grandson/granddaughter Brother/sister Husband/wife |
|
Occupation |
Office worker / Student / Fisherman
/ Freight transporter / Scrubber / Salesperson / Athlete / Logger /
Researcher / Pet beautician / Doctor / Educator / Housewife / Laborer / Baker
/ Nurse / Farmer / Beautician / Factory worker / Unemployed |
|
Clinical diagnosis |
Tinea capitis / Tinea corporis /
Tinea faciale Tinea barbae / Tinea manus / Tinea
unguium Tinea cruris / Candidiasis /
Pityriasis versicolor Malassezia folliculitis / Other |
|
Treatment |
Systemic medication -
Terbinafine -
Itraconazole - Fluconazole -
Griseofulvin |
|
Topical medication -
Terbinafine -
Ketoconazole -
Amorolfine -
Clotrimazole -
Isoconazole -
Sertaconazole -
Flutrimazole -
Lanoconazole -
Imidazole |
|
|
Suspected route of infection |
Soil/Cat/Dog/Other animals/Plant/Onychomycosis
(own infected nail) Other member of family/Other route Unknown |
3. Mycologic evaluation
Samples were collected after cleaning the affected skin surface with 70% alcohol. Scales were collected from the erythematous advancing border of the skin lesion with a sterile blunt scalpel, and in cases of tinea capitis, affected hair was removed using sterile surgical forceps. All samples were cultured on two sets of potato dextrose agar corn meal Tween 80 media and quickly transported to the department of dermatology, Yeungnam University Hospital. The cultured media was incubated at room temperature (20~25℃) for at least four weeks before discarding them as negative. Fungal species were identified by examining colony morphology, pigment production, and microscopic tease mount technique evaluations in lactophenol cotton blue. In cases where it was challenging to identify the organism via microscopic and macroscopic examinations, molecular biology methods were used with polymerase chain reaction (PCR) or PCR-Reverse Blot Hybridization Assay.
4. Ethics statement
This study was approved by the institutional review board of each institution (IRB number of the principal investigator's institution: 05-2016-091).
1. Patient demographics
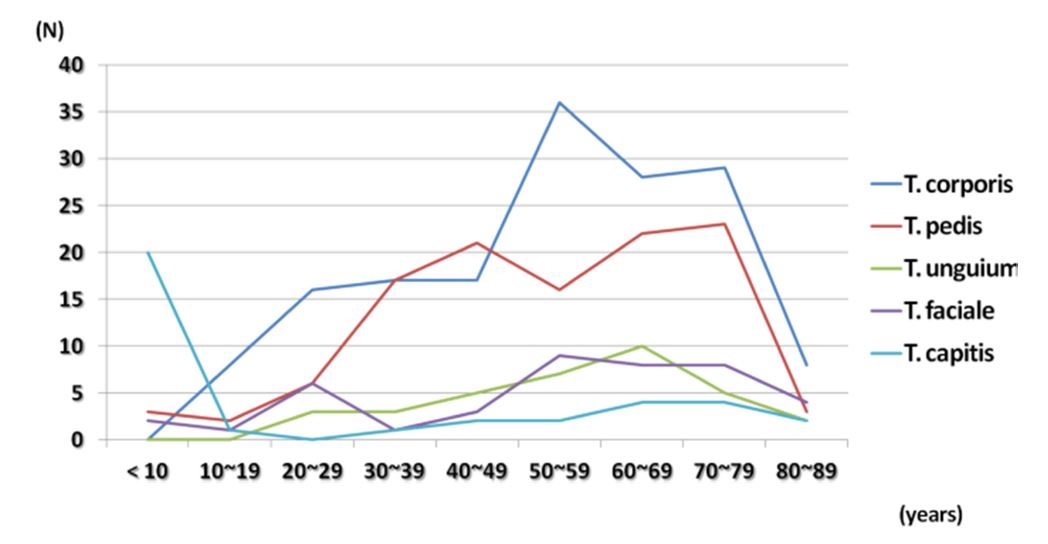
Total 453 patients with confirmed superficial dermatomycoses based on KOH examination were enrolled in this study. Among the 453 patients, majority were men (men: n = 275, 60.7% and women: n = 178, 39.3%), and the mean age of the patients was 51.4 ± 20.9 years (range, 9 months to 92 years). There was no difference in the mean age at visit between the men and women (51.0 vs. 51.9 years). Tinea capitis was the most common infection in children < 10 years of age, while tinea pedis had two peak incidences at 40~49 years and 70~79 years. Tinea corporis and tinea faciale were predominantly present in the 50~59-year age group. Tinea unguium most commonly occurred in the 60~69-year age group (Figure 1).
2. Patients' clinical characteristics
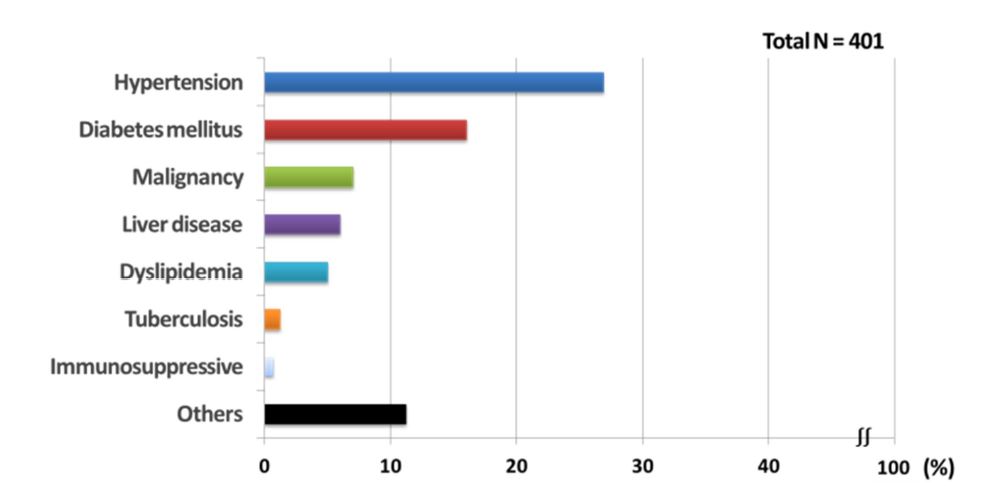
In terms of past history, 53.4% (214/401) of the patients had at least one comorbidity. Hypertension (108/401, 26.9%) was the most common comorbidity, followed by diabetes mellitus (64/401, 16.0%), malignancy (28/401, 7.0%), liver disease (24/401, 6.0%), and dyslipidemia (20/401, 5.0%) (Figure 2). Among patients without previous comorbidities, tinea pedis (77/238, 32.4%) was the most common type of superficial dermatomycoses, while in those with ≥ 1 comorbidity, tinea corporis (97/212, 45.8%) was the most common disease.
Sixty-eight patients (15.0%) had a family history of dermatomycoses. The most commonly infected family member was the father (24/68, 35.3%), followed by the son (14/68, 20.6%), mother (11/68, 16.2%), and husband (9/68, 13.2%). Among patients with a positive family history, infected family members mainly exhibited tinea pedis (41/68, 60.3%), and patients with a family history of superficial dermatomycoses usually experienced infections of tinea corporis (20/68, 29.4%).
Total 177 patients (41.3%) were non-workers, 59 (13.8%) were office workers, 40 (9.3%) were housewives, 27 (6.3%) were students, and 23 (5.3%) were farmers.
Clinically, tinea corporis (161/590, 27.3%) was the most common type of superficial dermatomycoses, followed by tinea pedis (137/590, 23.2%), tinea unguium (toe) (84/590, 14.2%), tinea cruris (78/590, 13.2%), tinea faciale (52/590. 8.8%), tinea capitis (36/590, 5.6%), tinea unguium (finger) (12/590, 2.2%), pityriasis versicolor (8/590, 1.4%), candidiasis (4/590, 0.7%), and tinea barbae (3/590, 0.3%).
Disease duration varied widely, depending on the type of superficial dermatomycoses. The disease duration was long for tinea unguium (toe) (mean, 74.9 months), tinea pedis (mean, 64.9 months), and tinea unguium (finger) (mean, 54.6 months), while that for tinea capitis (mean, 5.4 months), tinea barbae (mean, 6.0 months), and tinea faciale (mean, 9.9 months) was short (Table 2).
|
Clinical
diagnosis |
Patients
(%) |
Average
duration ± SD (Months) |
|
Tinea corporis |
161 (27.3) |
13.5 ± 39.96 (10 days ~ 360 months) |
|
Tinea pedis |
137 (23.2) |
64.9 ± 101.45 (15 days ~ 720 months) |
|
Tinea unguium (Toe) |
84 (14.2) |
74.9 ± 108.80 (1 month ~ 600 months) |
|
Tinea cruris |
78 (13.2) |
30.0 ± 62.85 (1 month ~ 360 months) |
|
Tinea faciale |
52 (8.8) |
9.9 ± 35.97 (7 days ~ 240 months) |
|
Tinea capitis |
36 (6.1) |
5.4 ± 12.41 (7 days ~72 months) |
|
Tinea unguium (Finger) |
14 (2.4) |
54.6 ± 60.26 (2 months ~ 120months) |
|
Tinea manus |
13 (2.2) |
9.3 ± 12.06 (1 month ~ 36 months) |
|
Pityriasis versicolor |
8 (1.4) |
18.7 ± 25.95 (7 days ~ 60
months) |
|
Candidiasis |
4 (0.7) |
9.0 ± 10.23 (1 month ~24 months) |
|
Tinea barbe |
3 (0.5) |
6.0 ± 3.46 (2 months ~8 months) |
|
Malassezia folliculitis |
0 (0) |
0 |
|
Total |
590 |
35.9 ± 75.68 (7 days ~ 720 months) |
Majority of the patients (297/442, 57.4%) were unaware of the infection route; however, 72 patients (16.3%) speculated that their infection was owing to pre-existing onychomycosis, 21 (4.8%) believed that they acquired it from their cat, 21 (4.8%) thought they got it from their dog, 20 (4.5%) believed that another family member was the infection source, and 11 (2.5%) thought they got it from the soil.
3. Treatment of superficial dermatomycoses
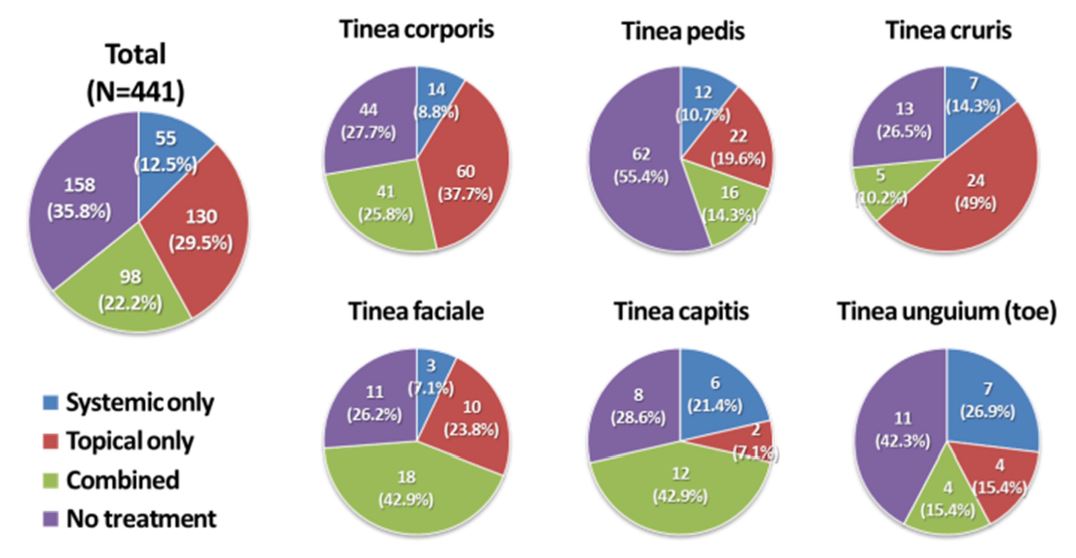
In this study, the dermatologist prescribed topical antifungal medication to 29.5% (130/441), systemic agent to 12.5% (55/441), and a combination of both to 22.2% (98/441) of the patients for the treatment of superficial dermatomycoses. When we classified the patients according to the subtype of superficial dermatomycoses, topical agents alone were predominantly used to treat tinea corporis, tinea pedis, and tinea cruris; systemic agents alone were usually used to treat tinea unguium (toe); a combination of topical and systemic agents was used to treat tinea capitis and tinea faciale (Figure 3).
The most commonly used systemic antifungal agent was terbinafine (117/155, 75.5%). However, itraconazole (13/18, 72.2%) was the most commonly used systemic agent for treating tinea capitis. For topical antifungal medications, various topical agents, such as amorolfine (57/247, 23.1%), terbina- fine (51/247, 20.6%), isoconazole (51/247, 20.6%), sertaconazole (40/247, 16.2%), and flutrimazole (26/247, 10.5%) were prescribed.
4. Mycologic findings
Fungal cultures were obtained from 162 patients (102 cases of isolated tinea corporis, 32 of tinea faciale, and 30 of tinea capitis) to identify the causative fungal strains. The overall positivity by fungal culture was 77.8% (126/162, 78.4% for tinea corporis, 71.9% for tinea faciale, and 76.7% for tinea capitis).
In the 80 isolated cases of tinea corporis, Trichophyton rubrum was present most commonly (68 cases, 66.7%), followed by yeast (5 cases, 4.9%), Microsporum canis (3 cases, 2.9%), Trichophyton mentagrophytes (2, 2.0%), and Trichophyton interdigitale and Cyphellophora europaea in (1 case each, 1.0%). In the 23 isolated incidences of tinea faciale, Trichophyton rubrum was present in 14 cases (43.8%), Microsprum canis in four (12.5%), and Trichophyton mentagrophyte, another Trichophyton species, yeast, Aspergillus jensenii, and Cladosporium halotolerans in one case (3.1%). In the 23 isolated incidences of tinea capitis, Microsporum canis was present in 11 cases (36.7%), Trichophyton rubrum in eight (26.7%), yeast in two (6.7%), and Trichophyton mentagrophytes and Microsporum canis with Trichophyton rubrum in one case (3.3%) (Figure 4).

This study surveyed the epidemiological and mycological characteristics of superficial dermatomycoses in Korea. Dermatomycosis was observed across all ages and in both sexes; however, its prevalence varied. Our study showed a mild male predominance that was consistent with several previous reports from Korea4,5. Tinea capitis was more common in children; however, all other types of superficial dermatomycoses were more common in adults, especially the elderly. It is already known that tinea capitis was common in the prepubertal period. Malassezia is predominantly localized in the adult scalp, while prepubertal children have more diverse fungal communities on their scalp; this may influence the predominance of tinea capitis in children6.
In terms of clinical characteristics, > 50% of the patients showed various comorbidities, including hypertension. Immune disturbances due to underlying comorbidities can lead the skin infections, including superficial dermatomycoses. Moreover, comorbidities lead to polypharmacy that is often associated with significant and clinically relevant drug interactions with antifungal agents, especially azole agents7. Therefore, it is crucial to identify the patient's comorbidities before selecting an antifungal agent. A family history of superficial dermatomycoses was identified in several patients, especially in male family members, such as fathers and sons. Tinea corporis infection can be transmitted from tinea pedis by the sharing of items, such as towels, with an infected person8. The most frequently suspected route of infection was a patient's own onychomycosis. Previously, approximately 42% of patients with onychomycosis had another concomitant dermatomycosis. Onychomycosis may provide a site from which the fungal infections could spread to other areas of the body. Therefore, treatment of pre-existing superficial dermatomycoses, such as onychomycosis, is believed to play a major role in preventing the spread of superficial dermatomycoses. The second most common suspected source of infection is animals (cats and dogs); this is the primary source of dermatomycosis, especially tinea capitis, in children who are in regular and intimate con- tact with cats and dogs. The increase in the number of house pets in Korea has also played an important role in the transmission of superficial mycoses. This infection pathway, in particular, causes alterations in the fungal species that cause superficial mycosis and facilitates the development of zoophilic dermatophytes, including microsporum9.
In cases of tinea pedis and tinea unguium, there is a considerable time delay in the patients' visit to the hospital owing to the lack of subjective symptoms or lesions in the unexposed areas. Tinea barbae and tinea faciale affect exposed areas, such as the face, and patients easily detect the lesions and visit clinics at the early stages of infection. For the treatment of superficial dermatomycoses, terbinafine is the dominant systemic antifungal medication10. Since terbinafine demonstrates high fungicidal activity, it is among the most commonly used systemic antifungal agents in the treatment of various dermatomycosis11. However, for tinea capitis, itraconazole is a widely used systemic antifungal agent in Korea. In North America, Trichophyton tonsurans is the most common causative organism for tinea capitis; however, Microsporum canis is most common in Korea and Europe12. It has been suggested that with Microsporum canis, a longer therapy duration or higher drug dose may be required in cases of terbinafine, while a short treatment period is required with itraconzaole for successful treatment outcomes12,13. Thus, itraconazole is the first choice of treatment for tinea capitis in Korea. Combined treatment with systemic and topical antifungal agents is usually applied for tinea capitis and tinea faciale infections that involve appendageal structures, such as hair.
In our mycological examination, the fungal culture positivity was 77.8%. Previous reports have shown that fungal positivity varies from 24% to 87. To achieve high rates of culture positivity, we used potato dextrose agar corn meal Tween 80 media, a suitable culture medium for Trichophyton rubrum that was developed at the Institute of Microbiology, Catholic Skin Clinic, Daegu, Korea. The potato and corn meal infusion provide the nutrition base required for sporulation, and dextrose serves as the energy source for pigmentation14. This medium intensifies the characteristic reverse wine-red colored pigmentation observed in Trichophyton rubrum and is more useful for the differentiation of Trichophyton rubrum from other fungi15. Trichophyton rubrum is the most common dermatophyte, accounting for approximately 88% of the causative fungal species in Korea16. Potato dextrose agar corn meal Tween 80 media benefits the cultivation of Trichophyton rubrum; this media may have played an important role in the acquisition of high culture positivity in our study. Moreover, fungal cultures were performed in a single institution by highly experienced individuals adept at achieving high fungal culture positivity.
Previous studies, as well as this investigation, have reported that Trichophyton rubrum is the most common causative agent of tinea corporis and faciale, and Microsporum canis is the most common agent of tinea capitis in Korea17-19 (Table 3). However, the ratios of yeast-induced tinea coporis, tinea faciale, and tinea capitis were higher than those in previous studies. This could be due to the increased prevalence of immunocom- promised patients or elderly individuals. Our study revealed this tendency among patients who were referred to the tertiary hospitals with various comorbidities. In addition, we found that the proportion of tinea faciale caused by Microsporum canis was higher than that in previous studies. Microsporum canis is the most common dermatophyte in cats and dogs; therefore, we suspected that an increase in the number of house pets influenced this difference20. In contrast, in tinea capitis, the prevalence of Microsporum canis infections decreased and that of Trichophyton rubrum infections increased. Microsporum canis is a representative zoophilic organism, and Trichophyton rubrum is an anthropophilic species. This increased overall incidence of anthropophilic tinea capitis has also been observed in a European study21-23. Therefore, we need to pay more attention to the inter-human transmission of tinea capitis caused by anthropophilic tinea capitis.
|
|
Tinea corporis |
Tinea faciale |
Tinea capitis |
|||
|
Present study (2016~2017) |
Ahn et al. |
Present study (2016~2017) |
Park et al. |
Present study |
Ahn et al. |
|
|
Trichophyton rubrum |
69.4% |
38.0% |
43.8% |
67.9% |
26.7% |
14.3% |
|
Yeast |
4.9% |
0% |
3.1% |
0% |
6.7% |
0% |
|
Microsporum |
2.9% |
4.8% |
12.5% |
0% |
36.7% |
82.1% |
|
Trichophyton mentagrophytes |
2.0% |
26.7% |
3.1% |
7.2% |
3.3% |
3.6% |
|
Trichophyton interdigitale |
1.0% |
2.9% |
0% |
0% |
0% |
0% |
|
Other |
1.0% |
0% |
9.3% |
10.7% |
3.3% |
0% |
|
Contamination |
2.9% |
6.7% |
6.3% |
3.5% |
6.7% |
0% |
|
No growth |
15.7% |
18.1% |
21.9% |
14.2% |
16.7% |
0% |
In conclusion, in Korean tertiary hospitals, superficial dermatomycoses were more common in male than in female patients, and the mean age of the infected patients was 51.4 ± 20.9 years. More than half of the patients had at least one comorbidity. Trichophyton rubrum was the most common pathogenic organism for tinea corporis and faciale, and Microsporum canis was the most common pathogen for tinea capitis. We believe that this study contributes to the treatment and management of superficial dermatomycoses by identifying the epidemiology and causative organisms of superficial dermatomycoses in Korea.
In relation to this article, I declare that there is no conflict of interest.
References
1. Kim SH, Cho SH, Youn SK, Park JS, Choi JT, Bak YS, et al. Epidemiological characterization of skin fungal infections between the years 2006 and 2010 in Korea. Osong Public Health Res Perspect 2015;6:341-345
Crossref
Google Scholar
2. Agarwal US, Saran J, Agarwal P. Clinico-mycological study of dermatophytes in a tertiary care centre in Northwest India. Indian J Dermatol Venereol Leprol 2014;80:194.
Crossref
Google Scholar
3. Suh SB. Dermatophytosis in Korea. Kyungpook Univ Med J 1959;59:1-33
Crossref
4. Kim JS, Young HW, Chun IK, Kim YP. Clinical and mycological studies on dermatomycosis. Korean J Dermatol 1992;30:68-75
Crossref
Google Scholar
5. Moon HJ, Lee JB, Kim SJ, Lee SC, Won YH. Clinical and mycological studies on dermatomycosis (1991-2000). Korean J Med Mycol 2002;7:78-85
Crossref
Google Scholar
6. Jo JH, Deming C, Kennedy EA, Conlan S, Polley EC, Ng WI. Diverse human skin fungal communities in children converge in adulthood. J Invest Dermatol 2016;136:2356 -2363
Crossref
Google Scholar
PubMed
7. Shivanna R, Rajesh. Management of dermatophytosis in elderly and with systemic comorbidities. Clin Dermatol 2017;1:S38-41
Crossref
Google Scholar
8. Jain A, Jain S, Rawat S. Emerging fungal infections among children: a review on its clinical manifestations, diagnosis, and prevention. J Pharm Bioallied Sci 2010;2:314-320
Crossref
Google Scholar
9. Nenoff P, Krüger C, Ginter-Hanselmayer G, Tietz HJ. Mycology - an update. Part 1: Dermatomycoses: causative agents, epidemiology and pathogenesis. J Dtsch Dermatol Ges 2014;12:188-209
Crossref
10. Millikan LE. Current concepts in systemic and topical therapy for superficial mycoses. Clin Dermatol 2010;28: 212-216
Crossref
Google Scholar
PubMed
11. Newland JG, Abdel-Rahman SM. Update on terbinafine with a focus on dermatophytoses. Clin Cosmet Investig Dermatol 2009;2:49-63
Crossref
Google Scholar
PubMed
12. Gupta AK, Ginter G. Itraconazole is effective in the treatment of tinea capitis caused by Microsporum canis. Pediatr Dermatol 2001;18:519-522
Crossref
Google Scholar
PubMed
13. Dragos V, Lunder M. Lack of efficacy of 6-week treatment with oral terbinafine for tinea capitis due to Microsporum canis in children. Pediatr Dermatol 1997;14:46-48
Crossref
Google Scholar
PubMed
14. Mahajan S, Tilak R, Kaushal SK, Mishra RN, Pandey SS. Clinico-mycological study of dermatophytic infections and their sensitivity to antifungal drugs in a tertiary care center. Indian J Dermatol Venereol Leprol 2017;83:436-440
Crossref
Google Scholar
15. Snyder JW, Atlas RM, LaROcco MT. Manual of clinical microbiology. 10th ed. Washington DC: ASM Press 2011: 1767-1775
Crossref
16. Kim HR, Kwon OS, Bang YJ, Park JS. Growth features of Trichophyton rubrum on potato dextrose agar-corn meal¬Tween 80 plate. Korean J Med Mycol 2016;21:103-104
Crossref
Google Scholar
17. Lee WJ, Kim SL, Jang YH, Lee SJ, Kim DW, Bang YJ, et al. Increasing prevalence of Trichophyton rubrum identified through an analysis of 115,846 cases over the last 37 years. J Korean Med Sci 2015;30:639-643
Crossref
Google Scholar
18. Jang SJ, Choe YB, Ahn KJ. A clinical and mycological study of tinea corporis. Korean J Dermatol 2004;42:166-172
Crossref
Google Scholar
19. Kim IY, Bang YJ, Jun JB, Park KD, Chung H, Park JS. The clinical and mycological study of tinea faciei in Daegu. Korean J Med Mycol 2015;20:63-69
Crossref
Google Scholar
20. Kim SM, Lee YW, Ahn KJ. A clinical and mycological study of tinea capitis. Korean J Med Mycol 2006;11:184-190
Crossref
21. Atzori L, Aste N, Aste N, Pau M. Tinea faciei due to Microsporum canis in children: a survey of 46 cases in the District of Cagliari (Italy). Pediatr Dermatol 2012;29:409- 413
Crossref
Google Scholar
22. Hay RJ, Robles W, Midgley G, Moore MK. Tinea capitis in Europe: new perspective on an old problem. J Eur Acad Dermatol Venereol 2001;15:229-233
Crossref
Google Scholar
PubMed
23. Ginter-Hanselmayer G, Weger W, Ilkit M, Smolle J. Epidemiology of tinea capitis in Europe: current state and changing patterns. Mycoses 2007;50:6-13
Crossref
Google Scholar
Congratulatory MessageClick here!
