pISSN : 3058-423X eISSN: 3058-4302
Open Access, Peer-reviewed
pISSN : 3058-423X eISSN: 3058-4302
Open Access, Peer-reviewed

Dong Heon Lee,Dong Hyek Jang,Mi Youn Park,Jiyoung Ahn,Hye Jung Jung
10.17966/JMI.2021.26.1.17 Epub 2021 March 29
Abstract
Serratia marcescens is an uncommon gram-negative bacterium strain that does not cause skin infections in healthy individuals. However, it is rarely reported as the causative agent of infection in immunosuppressed patients or in nosocomial infections. A 51-year-old man was admitted to a hospital presenting with pus and pain that had developed a month ago on a hypertrophic scar area of the back. Although he was on medication for diabetes mellitus, his blood sugar level was poorly controlled. In addition, two months earlier, he received an intralesional injection of 40 mg/mL triamcinolone twice for the hypertrophic scar of the back. S. marcescens was identified in the wound culture. His condition improved after ceftriaxone administration, debridement, and split-thickness skin grafts. Although S. marcescens is an infrequent cause of skin infections, it is important to remember that it may cause infection in some patients and that the course of the disease may be worse than that in a typical skin infection with poor prognosis.
Keywords
Cutaneous infection Serratia marcescens
Serratia marcescens is a gram-negative bacterium that belongs to the Enterobacteriaceae family. It can usually be found in water, soil, plants, and insects, and it is not a strain that is known to be a causative agent of skin infections in healthy subjects. Indeed, it rarely causes infection even in immunosuppressed patients. In addition, it can stick to the surface of medical instruments used for invasive procedures, such as catheters or intravenous tubing. In some cases, it is resistant to disinfection or sterilization, thereby causing nosocomial infections.
To date, there have been reports on lung and genitourinary infection, septicemia, meningitis, wound infection, and keratitis caused by S. marcescens. Skin infections caused by S. marcescens can be divided into two types: acute type with cellulitis or intradermal abscess, and chronic type with persistent nodules or repeat cycles of improvement and deterioration.
A 51-year-old man presented to the hospital with a hard plaque on the back. The lesion occurred after coronary angiography (CAG) that had been performed one year prior to admission. The plaque became harder over time and was associated with itching and slight tenderness. The patient was diagnosed with hypertension and diabetes mellitus in 2003 and was on medication for both conditions.
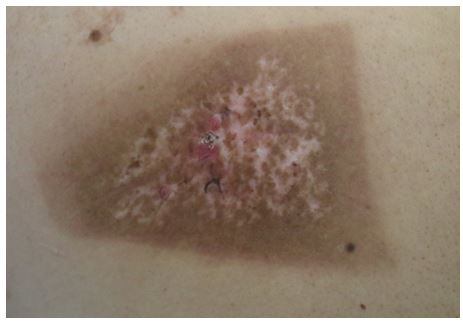
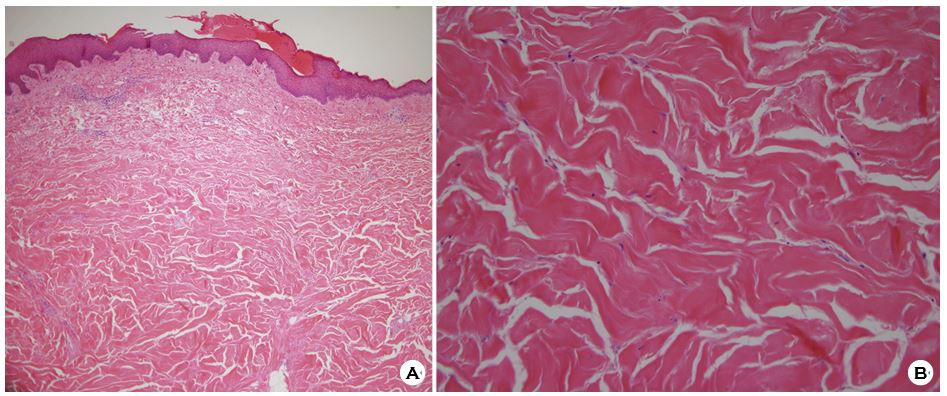
The lesion had a patch of hyperpigmentation and hypo- pigmentation, which were presumed to be adverse effects of the previous CAG, and a coarse crust was found in the center (Fig. 1). The lesion was sharply demarcated, hard on palpation, and showed no signs of infection, such as erythema, edema, or pus, other than slight tenderness. Biopsy performed (Fig. 2) revealed a hypertrophic scar, and intralesional injection (ILI) of 40 mg/mL triamcinolone was administered every other week to improve symptoms.
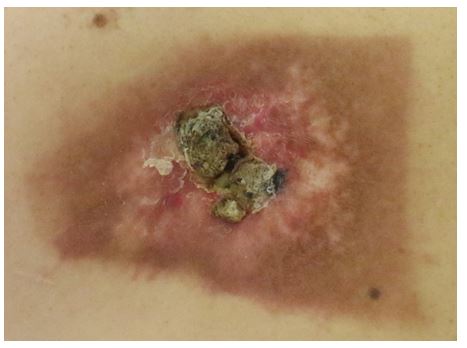
On a follow-up visit two months after the last ILI, pus was found in the crust in the middle of the lesion (Fig. 3). The patient stated that pus and pain had occurred one month prior and that the symptoms worsened despite treatment at another hospital. Laboratory tests revealed an elevated level HbA1c level at 12.6%, indicating that diabetes was not con- trolled. S. marcescens was positive in the wound culture, and the results of antibiotic susceptibility tests showed resistance to amoxicillin/clavulanic acid, cefazolin, and cefoxitin, and sensitivity to cefotaxime, ceftazidime, cefepime, and ciprofloxacin. The patient was referred to a plastic surgeon for surgery, and his condition improved after ceftriaxone administration, debridement, and split-thickness skin grafts.
Skin infection caused by S. marcescens is uncommon. However, it can be divided into two types: acute and severe type and chronic type. The acute and severe type is seen in patients with underlying diseases, such as diabetes mellitus or liver cirrhosis, as in the present case, while the chronic type is seen in healthy individuals. Acute and severe cases can present severe ulcers, necrotizing fasciitis, and multiple intra-ermal abscesses. These do not respond well to treatment with antibiotics alone, therefore surgical treatment is often required. This type of infection is often reported in diabetic patients, since diabetes weakens the immune system. More specifically, in diabetic patients, leukocyte chemotaxis and phagocytosis are reduced; moreover, vascular reaction is also reduced, leading to frequent infection and delayed recovery. The patient in this case also did not respond to antibiotic treatment before visiting a hospital, and the skin defect was already severe at the time of admission. Therefore, surgical treatment was required along with antibiotic treatment.
Among the organisms in the Serratia genus, S. marcescens is the main pathogen, and, rarely, S. liquefaciens, S. plymuthica, S. rubidaea, S. odorifera, and S. fonticola can also cause diseases. Given that S. marcescens may be resistant to many drugs, antibiotic susceptibility testing must be performed. In general, antibiotics, such as third-generation cephalosporins, aminoglycosides, carbapenems, fluoroquinolones, and trimethoprim-sulfamethoxazole, are known to be effective. The present case was resistant to amoxicillin/clavulanic acid and first- and second-generation cephalosporins, such as cefazolin and cefoxitin. However, third- and fourth-generation cephalosporins, such as cefotaxime, ceftazidime, cefepime, and ciprofloxacin, showed sensitivity. Therefore, the patient was placed on ceftriaxone.
Although the patient had an injection of triamcinolone, we presume that the triamcinolone injection did not have a direct effect on the infection, since symptoms occurred a month after the injection. However, it is worth noting that the use of steroid may adversely affect the control of diabetes in some patients and that infections which occur after ILI are relatively more prone to keloid formation than other lesions.
This report describes a case of S. marcescens skin infection in a patient with uncontrolled diabetes. Although it accounts for a relatively low percentage of cutaneous infections, it has constantly been reported. Therefore, it is important to note that it may be the cause of infection in certain patients and that the course may be worse than that of normal skin infections with poor prognoses.
References
1. Rodrigues AP, Holanda AR, Lustosa GP, Nóbrega SMB, Santana WJ, Souza LB, et al. Virulence factors and re- sistance mechanisms of Serratia marcescens: A short review. Acta Microbiol Immunol Hung 2006;53:89-93
Google Scholar
2. Cristina ML, Sartini M, Spagnolo AM. Serratia marcescens infections in neonatal intensive care units (NICUs). Int J Environ Res Public Health 2019;16:610
Google Scholar
3. Veraldi S, Nazzaro G, Skin ulcers caused by Serratia marcescens: three cases and a review of the literature. Eur J Dermatol 2016;26:373-376
Google Scholar
4. Soria X, Bielsa I, Ribera M, Herrero MJ, Domingo H, Carrascosa JM, et al. Acute dermal abscesses caused by Serratia marcescens. J Am Acad Dermatol 2008;58:891-893
Google Scholar
5. Farajollahi A, Rahimi A, Shal EK, Ghaffari S, Ghojazadeh M, Tajlil A, et al. Patient's radiation exposure in coronary angiography and angioplasty: The impact of different projections. J Cardiovasc Thorac Res 2014;6:247-252
Google Scholar
6. Combemale P, Faisant M, Azoulay-Petit C, Dupin M, Kanitakis J. Neutrophilic eccrine hidradenitis secondary to infection with Serratia marcescens. Br J Dermatol 2000; 142:784-788
Google Scholar
7. João AM, Serrano PN, Cachão MP, Bártolo EA, Brandão FM. Recurrent Serratia marcescens cutaneous infection manifesting as painful nodules and ulcers. J Am Acad Dermatol 2008;58:S55-S57
Google Scholar
8. Lima AL, Illing T, Schliemann S, Elsner P. Cutaneous mani- festations of diabetes mellitus: a review. Am J Clin Dermatol 2017;18:541-553
Google Scholar
9. Mendes AL, Miot HA, Junior VH. Diabetes mellitus and the skin. An Bras Dermatol 2017;92:8-20
10. Park KY, Seo SJ. Cutaneous Serratia marcescens infection in an immunocompetent patient after filler injection. Acta Derm Venerol 2013;93:191-192
Google Scholar
11. Cooper CL, Wiseman M, Brunham R. Bullous cellulitis caused by Serratia marcescens. Int J Infect Dis 1998;3: 36-38
Google Scholar
12. Yoshida R, Takae Y, Fujio Y, Tanaka M, Ohyama M. Cutaneous Serratia marcescens infection on the face of a healthy female. J Eur Acad Dermatol Venereol 2009; 23:1213-1215
Google Scholar
13. Grim KD, Doherty C, Rosen T. Serratia marcescens bullous cellulitis after iguana bites. J AM Acad Dermatol 2010; 62:1075-1076
Google Scholar
14. Luther CA, Griffith JL, Kurland E, Shabeeb RA, Eleryan M, Redbord K, et al. The infection rate of intralesional triamcinolone and the safety of compounding in der- matology for intradermal and subcutaneous injection: A retrospective medical record review. J Am Acad Dermatol 2020;83:1044-1048
Google Scholar
15. Seo J, Shin D, Oh SH, Lee JH, Chung KY, Lee M, et al. Cutaneous Serratia marcescens infections in Korea: A retrospective analysis of 13 patients. J Dermatol 2016;43: 149-155
Google Scholar
Congratulatory MessageClick here!
