pISSN : 3058-423X eISSN: 3058-4302
Open Access, Peer-reviewed
pISSN : 3058-423X eISSN: 3058-4302
Open Access, Peer-reviewed

Jeongsoo Lee,Yongwoo Choi,Joonsoo Park
10.17966/JMI.2021.26.1.13 Epub 2021 March 29
Abstract
Keywords
Tinea pseudoimbricata Trichophyton tonsurans
Tinea imbricata is a unique dermatophytosis caused by Trichophyton(T) concentricum. It is observed endemically in subtropical to torrid zones and characterized by concentric scaly rings on the trunk or limbs. The term tinea imbricata is restricted to T. concentricum infection, but other dermatophytosis may mimic this disease as "tinea pseudoimbricata". It can be caused by T. mentagrophytes and T. rubrum infection in regions other than tropical countries.
T. tonsurans is an anthropophilic dermatophyte transmitted through human contact. It is globally distributed and is most prevalent in the United States, Canada, Mexico, and some European countries. The common clinical manifestations of T. tonsurans infection are tinea capitis and tinea corporis. However, few cases of patients with compromised immunity showed development of concentric annular erythemas.
This study reported a case of tinea pseudoimbricata caused by T. tonsurans in South Korea.
A 60-year-old man presented with multiple scaly erythematous to purpuric concentric patches on both the lower extremities (Figs. 1A, 1B, 1C) visited our clinic 1 month ago. Nails and scalp were observed to be unaffected. He was administered oral antihistamines and applied a topical agent mixed with diflucortolone valerate and isoconazole nitrate at a local medical center, but the lesions gradually enlarged. He was then transferred from the local medical center to rule out erythema gyratum repens. Although he was on medication for hypertension, there were no recent medication changes. He had no abroad travel history. No other internal disease or abnormal results were observed during medical examination.
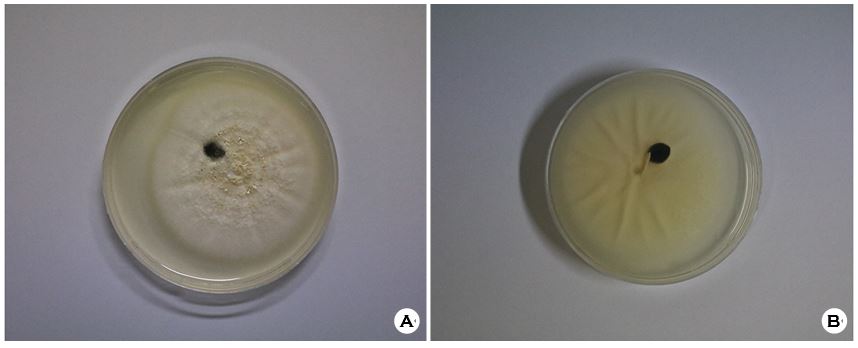
KOH mount of scale and fungal culture were performed at the right calf. KOH mount revealed multiple hyphae on specimen. White velvety colonies with fine granules and concentric furrows were observed after incubation at 25℃ for 2 weeks on Sabouraud's dextrose agar. The colonies appeared yellowish white on the reverse side (Figs. 2A, 2B). Microscopic examination of the culture revealed pear-shaped microconidia and roller-shaped macroconidia. These findings confirmed a T. tonsurans infection. The patient was finally diagnosed with tinea pseudoimbricata caused by T. tonsurans and started treatment with topical antifungal agent in addition to oral administration of terbinafine. He visited our clinic again after 2 weeks with improved skin lesions and post-inflammatory hyperpigmentation (Figs. 3A, 3B).

The term "imbricata" is derived from the Latin word imbrex and refers to overlapping roof tiles. Tinea imbricata is a distinct superficial mycosis caused by T. concentricum with a characteristic pattern of concentric annular plaques of erythema and scales. The disease has a restricted geographical distribution in South-East Asia, South Pacific, Central, and South America. Cases clinically resembling tinea imbricata but caused by species other than T. concentricum are reported as "tinea pseudoimbricata" or "tinea indecisiva". Tinea pseudoimbricata has been reported to be caused by T. tonsurans, T. rubrum, T. mentagrophytes, Microsporum audouinii, and Microsporum gypseum.
It has been stated in the literature that the development of concentric rings is due to a negative, delayed-type hyper- sensitivity to the T. concentricum cytoplasmic antigen and T-lymphocyte hyporeactivity. Immunosuppression plays a central role in the development of both tinea pseudoimbricata and tinea imbricata. Secondary to topical corticosteroid misuse, or some form of underlying immunosuppression such as protein-energy malnutrition, HIV infection, or immunosup- pressive therapy following transplantation can be a cause of immunosuppression. A previous study conducted in Papua New Guinea reported that 52% of individuals with tinea imbricata (35/68) failed to develop a delayed-type hyper- sensitivity reaction despite demonstrating normal immediate-type hypersensitivity responses. This implies that individuals with tinea imbricata have deficient cellular immunity.
The process of characteristic lesions is estimated as follows in the immunosuppressed host. From the primary fungal infection site, digestion of keratin by multiple fungal proteases and inflammatory reactions occurs in the host's skin. The hair follicles present in the lesions act as a central storage for fungus in the entire process. When the host's systemic or local immunity decreases, secondary and tertiary circular patches progress and make characteristic lesions from each storage, resulting in a ring within a ring formation.
There have been no reports of tinea imbricata, whereas six cases of tinea pseudoimbricata are found in South Korea, including this one (Table 1). There are two cases of T. verrucosum, two cases of T. rubrum, and one case of Microsporum ferrugineum. All cases were treated with systemic antifungal agents like oral terbinafine with or without topical antifungal agents regardless of species of fungus. There was no case reporting "successful treatment with only topical antifungal agent".
In this case there was no improvement even after applying a mixture of diflucortolone valerate and isoconazole nitrate. The patient showed improvement with additional oral terbinafine.
It is recommended to perform an immediate KOH mount of scale and fungal culture in patients with a ring within a ring formation of skin lesions for fungal infection. Laboratory tests and medical examinations should be followed to check the immune status of the patient. For patients with these lesions, it is likely to be accompanied by a local or systemic immunosuppression. Therefore, it would be helpful to use systemic antifungal agents in combination with topical agents.
|
Author |
Age/Sex |
Infection
site |
Treatment |
Fungus |
|
Lee
et al. (1987)4 |
9/Male |
Right forearm |
Topical bifonazole and ciclopirox, |
Microsporum
ferrugineum |
|
Roh
et al. (2000)5 |
19/Male |
Right forearm |
Oral itraconazole |
Trichophyton
rubrum |
|
Lim
et al. (2006)6 |
7/Male |
Left thigh |
Oral terbinafine, Topical lanoconazole |
Trichophyton
verrucosum |
|
Kang
et al. (2008)7 |
69/Female |
Right forearm |
Oral terbinafine, Topical lanoconazole |
Trichophyton
verrucosum |
|
Kwon
et al. (2020)8 |
80/Female |
Left abdomen |
Oral terbinafine, Topical terbinafine |
Trichophyton
rubrum |
|
Present case |
60/Male |
Both legs |
Oral terbinafine, Topical
isoconazole |
Trichophyton tonsurans |
References
1. Ouchi T, Nagao K, Hata Y, Otuka T, Inazumi T. Tricho- phyton tonsurans infection manifesting as multiple concentric annular erythemas. J Dermatol 2005;32:565-568
Google Scholar
2. Singal A, Jakhar D, Kaur I, Pandhi D, Das S. Tinea pseudo- imbricata as a unique manifestation of steroid abuse: a clinico-mycological and dermoscopic study from a tertiary care hospital. Indian Dermatol Online J 2019;10:422-425
Google Scholar
3. Lim SP, Smith AG.
Google Scholar
4. Lee H, Lee ES, Kang WH, Lee SN. An unusual clinical manifestation of tinea corporis caused by Microsporum ferrugineum. Korean J Dermatol 1987;25:383-388
Google Scholar
5. Roh DK, Park CJ, Yi JY, Lee HK. A case of tinea corporis showing tinea imbricata-like clinical appearance. Korean J Med Mycol 2000;5:20-
Google Scholar
6. Lim JW, Lee YH, Suh MK, Ha GY, Kim JR. A case of tinea corporis caused by Trichophyton verrucosum showing tinea imbricata-like clinical appearance. Korean J Dermatol 2006;44:318-321
Google Scholar
7. Kang GS, Go WT, Suh MK, Ha GY, Lee JI. A case of tinea corporis caused by Trichophyton verrucosum showing tinea imbricata-like clinical appearance. Korean J Med Mycol 2008;13:181-186
Google Scholar
8. Kwon HM, Kim HR, Shin DH, Choi JS. Tinea pseudo- imbricata caused by Trichophyton rubrum. J Mycol Infect 2020;25:22-25
Google Scholar
9. Narang K, Pahwa M, Ramesh V. Tinea capitis in the form of concentric rings in an HIV positive adult on antiretroviral treatment. Indian J Dermatol 2012;57:288-290
Google Scholar
10. Satter EK. Tinea Imbricata. Cutis 2009;83:188-191
Google Scholar
Congratulatory MessageClick here!
