pISSN : 3058-423X eISSN: 3058-4302
Open Access, Peer-reviewed
pISSN : 3058-423X eISSN: 3058-4302
Open Access, Peer-reviewed

Eui-Sung Jung,Sang-Kyung Lee,Il-Jae Lee,Jin Park,Seok-Kweon Yun,Han-Uk Kim
10.17966/JMI.2021.26.1.8 Epub 2021 March 29
Abstract
Purpureocillium lilacinum (formerly Paecilomyces lilacinus) is a saprophytic fungus found in the soil and decaying vegetation and is rarely pathogenic to humans. To our knowledge, only six cases of cutaneous infection caused by P. lilacinum have been reported in journals published by the Korean Dermatological Association and the Korean Society for Medical Mycology. Here, we report the case of a patient with localized cutaneous infection caused by P. lilacinum. An 84-year-old woman presented with a 2-month history of multiple plaques with surrounding erythematous patches on her left forearm and dorsum of the hand. Histopathological examination showed suppurative inflammation accompanied by fungal elements in the dermis. Furthermore, periodic acid-Schiff and methenamine silver staining showed revealed fungal elements. The sub-cultured fungus of the isolate revealed velvety pink colonies that were yellowish-tan on the reverse side, and lactophenol cotton blue staining showed flask-shaped phialides. The DNA sequence from the colony was identical to that of P. lilacinum. The patient was treated with oral itraconazole (200 mg/d) for 6 weeks that achieved significant improvement in the patient's condition.
Keywords
Cutaneous infection Purpureocillium lilacinum
Purpureocillium lilacinum, a saprophytic filamentous fungus commonly found in soil, is rarely pathogenic to humans. However, infective endocarditis, pulmonary infections, and localized skin infections caused by P. lilacinum have been reported in immunocompromised patients who have under- gone kidney transplantation or bone marrow transplantation or have malignant tumors; these disorders may also have idiopathic origin. Only six cases of cutaneous infection due to P. lilacinum have been reported in journals published by the Korean Dermatological Association (KDA) and the Korean Society for Medical Mycology (KSMM). Here, we report the case of a patient with cutaneous infection caused by P. lilacinum that was believed to be associated with repeated physical trauma in a healthy patient.
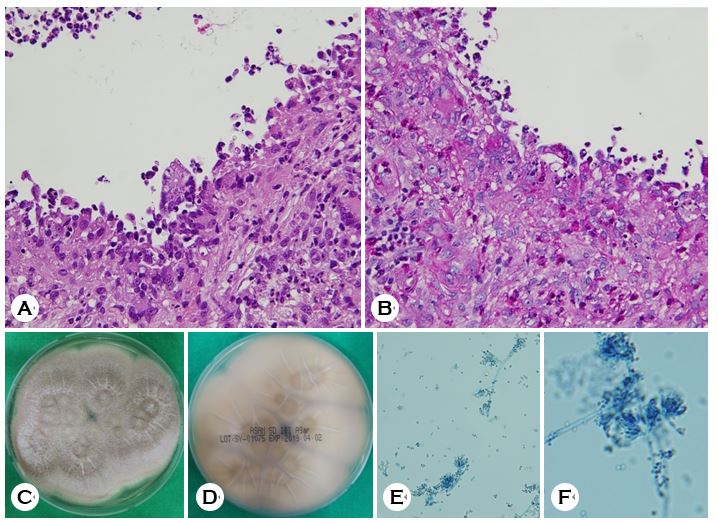
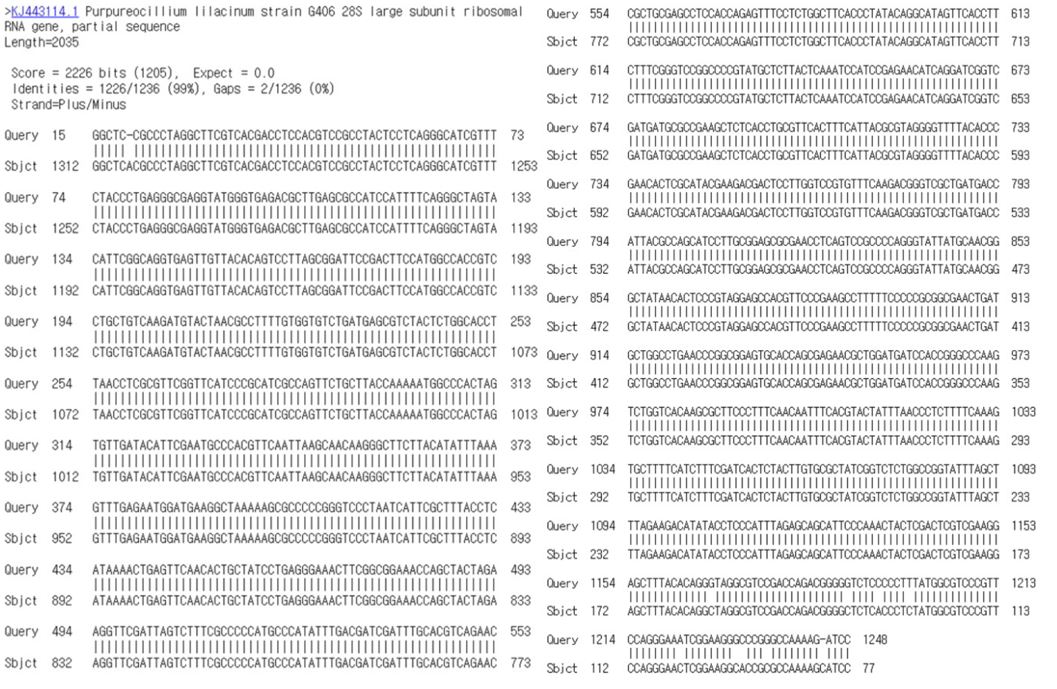
An 84-year-old female patient presented with a 2-month history of pruritic localized cutaneous lesions on her left forearm and the dorsum of the hand (Fig. 1A). There was no pain, direct tenderness, heating sensation, or fever. She was a farmer who used a hand hoe on a daily basis for performing her farm work, and she had a history of repeated trauma on the affected site, caused by the frequent use of farming tools. There was no underlying immunocompromising disease or relevant family medical history. Physical examination revealed multiple plaques with surrounding erythematous patches. Laboratory findings, including complete blood count, blood chemistry, and urinalysis, were within the normal ranges. A skin biopsy of the left forearm and a fungal culture of the biopsied specimen were performed. Hematoxylin and eosin (H&E) staining revealed suppurative inflammation with fungal elements in the dermis (Fig. 2A). Periodic acid-Schiff (PAS) staining was positive for fungal elements (Fig. 2B). The biopsied specimen was cultured on Sabouraud dextrose agar (SD AgarTM, Asan Pharm, Hwaseong-si, Korea) and was kept in an incubator at 28℃. Velvety white and light brown colonies, observed from the original colony, were sub-cultured at room temperature (25℃) for 14 d, resulting in velvety pink colonies. A yellowish-tan color was observed on the reverse side of the sub-cultured fungus (Fig. 2C, 2D). Flask-shaped phialides were observed after staining the colony with lactophenol cotton blue (Fig. 2E, 2F). Subsequently, DNA sequence analysis of the internal transcribed spacer rRNA gene and assessment using the basic local alignment search tool program revealed 99% sequence similarity; thus, the colony was conclusively identified as P. lilacinum (Fig. 3). The patient was treated with oral itraconazole (200 mg/day) for a period of 6 weeks. Improvement in the cutaneous lesions with mild post-inflammatory hyper-pigmentation was observed at the end of 6 weeks of treatment (Fig. 1B). A follow-up biopsy culture was not performed because the patient did not visit us for the follow-up appointment.

P. lilacinum, formerly called Paecilomyces lilacinus, is a fungal pathogen that is commonly found in soil and decaying vegetation. Skin and soft tissue infections caused by P. lilacinum are very rare. The first reported case of localized cutaneous infection by P. lilacinum that manifested as uni- lateral cellulitis was reported in 1977. Thereafter, only six case reports of cutaneous infection caused by P. lilacinum have been published by the KDA and the KSMM (Table 1). Our report describes the case of a patient with cutaneous infection caused by P. lilacinum that was believed to be associated with repeated physical contact with farming tools.
P. lilacinum infections predominantly occur in immunocompromised patients, such as those with a history of organ transplantations, diabetes mellitus, malignant tumors, and prolonged use of immunosuppressants or steroids. How- ever, P. lilacinum infections in immunocompetent patients have been reported to occur following ophthalmic surgery or non-surgical trauma. As per Pastor et al., 18.6% of cutaneous P. lilacinum infections occurred in patients who had no predisposing factors. Five out of the 6 (83.3%) patients reported by the KDA and the KSMM did not have any immunocompromising illness. In our case, the patient had no immunocompromising disease; however, he had a history of repeated trauma owing to the use of farming tools. Kwak et al. suggested that frequent exposure to soil and unnoticed injuries that are commonly found in farmers are risk factors for cutaneous P. lilacinum infections. Our patient was a farmer; two out of six (33.3%) previously reported cases also had agriculture-related occupations. The unnoticed wound site in our patient was considered to be the entry point for the opportunistic infection. Therefore, we suggest careful physical examination and clinical history-taking for the identification of signs of trauma that may be inconspicuous or may have been unnoticed by the patients themselves.
Clinical manifestations of cutaneous P. lilacinum infections show considerable variation. Erythematous macules, patches, plaques, nodules, pustules, vesicles, and necrotic crusts have been described in previous trials. Fungal cultures and histologic studies are essential for confirming the diagnosis. Colonies of P. lilacinum rapidly grow on SD agar at room temperature with a velvety, whitish light-pink and lilac color, and a dome-shaped appearance. Lactophenol cotton blue staining show that the conidiophores have delicate phialides with long tapering necks arranged like paintbrushes and elliptical conidia attached to chains at the ends. Histopathological examination of the skin reveals spores and chronic granulomatous inflammation with lymphocytes, histiocytes, and giant cells in the dermis on H&E stains. Molecular techniques, including real-time polymerase chain reaction (PCR) and species-specific primers, are also highly effective as diagnostic tools. In our study, we identified P. lilacinum with the fungus isolate observed from the fungal culture of the biopsied specimen and the DNA sequencing of ITS rRNA gene.
Treatments for P. lilacinum include surgical debridement, systemic antifungal therapy, or a combination of these two methods. High resistance to conventional antifungal drugs has been reported in various studies. Furthermore, the selection of antifungal drugs based on previous case reports is essential because there are no established guidelines for the treatment of P. lilacinum. Unfavorable outcomes have been observed with amphotericin B, flucytosine, fluconazole, miconazole, terbinafine, and itraconazole. A review of 20 cases of cutaneous infection by P. lilacinum showed that only 4 of the 20 patients responded to itraconazole. In cases reported by KDA and KSMM, including our case, four patients showed clinical improvement with itraconazole administration, and one patient, who did not respond to this treatment, showed improvement after voriconazole administration. In our case, the cutaneous lesions had almost resolved by the end of 6 weeks of itraconazole treatment. However, no improvement was observed even after itraconazole was administered for 14 weeks in the cases reported by Jung et al. and Pastor et al.. This suggests that the use of voriconazole in combination with surgery is the most effective treatment. Owing to the variable susceptibility of P. lilacinum to antifungal drugs and the absence of unanimous treatment guidelines, the measurement of the minimal inhibitory concentration to determine resistance to antifungal agents before treatment may help in selecting the most appropriate agent.
In sum, we report a case of cutaneous P. lilacinum infection in a healthy patient who was exposed to repeated physical trauma, wherein the patient responded favorably to itraconazole treatment. Thus, we concluded that careful and meticulous physical examination and history-taking may provide important clues for opportunistic infections. We also expect this report to contribute toward a deeper under- standing of cutaneous P. lilacinum infection.
|
Author |
Age/ |
Cutaneous presentation |
Location |
Predisposing |
Treatment |
|
Cho et al.5 |
19/M |
Erythematous patch |
Cheek |
None |
Griseofulvin, |
|
Shin et al.6 |
46/M |
Erythematous nodules |
Forearm |
Renal transplantation |
Excision |
|
Ko et al.7 |
83/M |
Erythematous plaque |
Wrist |
None |
Itraconazole |
|
Hwang et al.8 |
81/M |
Erythematous plaque and |
Hand |
None |
Itraconazole |
|
Jung et al.9 |
72/M |
Erythematous plaque |
Shoulder |
None |
Itraconazole, |
|
Kwak et al.10 |
81/M |
Erythematous pustular plaque |
Dorsal hand |
None |
Itraconazole |
|
Present case |
84/F |
Erythematous papules & patch |
Forearm |
Injury from hoe |
Itraconazole |
References
1. Kwon-Chung KJ, Bennett JE. Medical mycology. Philadelphia: Lea & Febiger, 1992:747-750
2. Castro LG, Salebian A, Sotto MN. Hyalohyphomycosis by Paecilomyces lilacinus in a renal transplant patient and a review of human Paecilomyces species infections. J Med Vet Mycol 1990;28:15-26
3. Gutiérrez-Rodero F, Moragón M, Ortiz de la Tabla V, Mayol MJ, Martín C. Cutaneous hyalohyphomycosis caused by Paecilomyces lilacinus in an immunocompetent host successfully treated with itraconazole: case report and revew. Eur J Clin Microbiol Infect Dis 1999;18:814-818
Google Scholar
4. Takayasu S, Akagi M, Shimizu Y. Cutaneous mycosis caused by Paecilomyces lilacinus. Arch Dermatol 1977; 113:1687-1690
Google Scholar
5. Cho GY, Choo EH, Choi GJ, Hong NS, Houh W. Facial cutaneous mycosis by Paecilomyces lilacinus. Korean J Dermatol 1984;22:89-93
Google Scholar
6. Shin SB, Lee HN, Kim SW, Park GS, Cho BK, Kim HJ. Cutaneous abscess caused by Paecilomyces lilacinus in a renal transplant patient. Korean J Med Mycol 1998;3: 185-189
Google Scholar
7. Ko WT, Kim SH, Suh MK, Ha GY, Kim JR. A case of localized skin infection due to Paecilomyces lilacinus. Korean J Dermatol 2007;45:930-933
Google Scholar
8. Hwang SL, Kim JI, Song KH, Cho YS, Nam GH, Park J, et al. A localized skin infection due to Paecilomyces lilacinus. Korean J Dermatol 2011;64(Suppl. 1):255
Google Scholar
9. Jung MY, Park JH, Lee JH, Lee JH, Yang JM, Lee DY. A localized cutaneous Paecilomyces lilacinus infection treated with voriconazole. Korean J Dermatol 2013;51: 833-836
Google Scholar
10. Kwak HB, Park SK, Yun SK, Kim HU, Park J. A case of localized skin infection due to Paecilomyces lilacinum. Korean J Med Mycol 2017;22:42-49
Google Scholar
11. Van Schooneveld T, Freifeld A, Lesiak B, Kalil A, Sutton DA, Iwen PC. Paecilomyces lilacinus infection in a liver transplant patient: case report and review of the literature. Transpl Infect Dis 2008;10:117-122
Google Scholar
12. Antas PR, Brito MM, Peixoto E, Ponte CG, Borba CM. Neglected and emerging fungal infections: review of hyalohyphomycosis by Paecilomyces lilacinus focusing in disease burden, in vitro antifungal susceptibility and management. Microbes Infect 2012;14:1-8
Google Scholar
13. Pastor FJ, Guarro J. Clinical manifestations, treatment and outcome of Paecilomycese lilacinus infections. Clin Microbiol Infect 2006;12:948-960
Google Scholar
14. Itin PH, Frei R, Lautenschlager S, Buechner SA, Surber C, Gratwohl A, et al. Cutaneous manifestations of Paecilo- myces lilacinus infection induced by a contaminated skin lotion in patients who are severely immunosup- pressed. J Am Acad Dermatol 1998;39:401-409
15. Kim JR, Kim DH, Jang JH, Sung HS, Kim MN. A case of fungal keratitis caused by Purpureocillium lilacinum: a microbiological review of Korean cases. Korean J Med Mycol 2016;21:84-91
Google Scholar
Congratulatory MessageClick here!
