pISSN : 3058-423X eISSN: 3058-4302
Open Access, Peer-reviewed
pISSN : 3058-423X eISSN: 3058-4302
Open Access, Peer-reviewed

Dong Won Lee,Sangbin Jeong,Moo Kyu Suh,Gyoung Yim Ha,Jong Im Lee,Jong Soo Choi
10.17966/JMI.2020.25.4.76 Epub 2021 January 06
Abstract
The patient provided written informed consent for the publication and the use of his images.
Keywords
Contact dermatitis Tinea faciei Trichophyton verrucosum
Tinea faciei is a dermatophyte infection that occurs on the nonbearded regions of the face. It is often confused with other dermatoses because fungal infections occur more frequently in other parts of the body. Tinea faciei has been known to mimic other disorders (e.g., cutaneous lupus erythematosus, cellulitis, granuloma annulare, contact dermatitis, seborrheic dermatitis, and impetigo contagiosum). However, tinea faciei can be misdiagnosed as contact dermatitis if it occurs in the periocular area after ophthalmic treatment. Any substances including environmental and therapeutic contact allergens may produce contact dermatitis because the periocular region is one of the most sensitive areas of the face.
Cutaneous lesions caused by Trichophyton verrucosum are known to be the most common causative dermatophytosis pathogen caused by cattle and are usually clinically characterized by intense inflammation. Thus, they are often misdiagnosed as eczema. Besides, the diagnosis can be even missed by false-negative results from potassium hydroxide (KOH) preparation in atypical cases of tinea faciei. In such cases, a definitive diagnosis can easily be histologically con- firmed by the presence of periodic acid Schiff-positive fungi in stratum corneum.
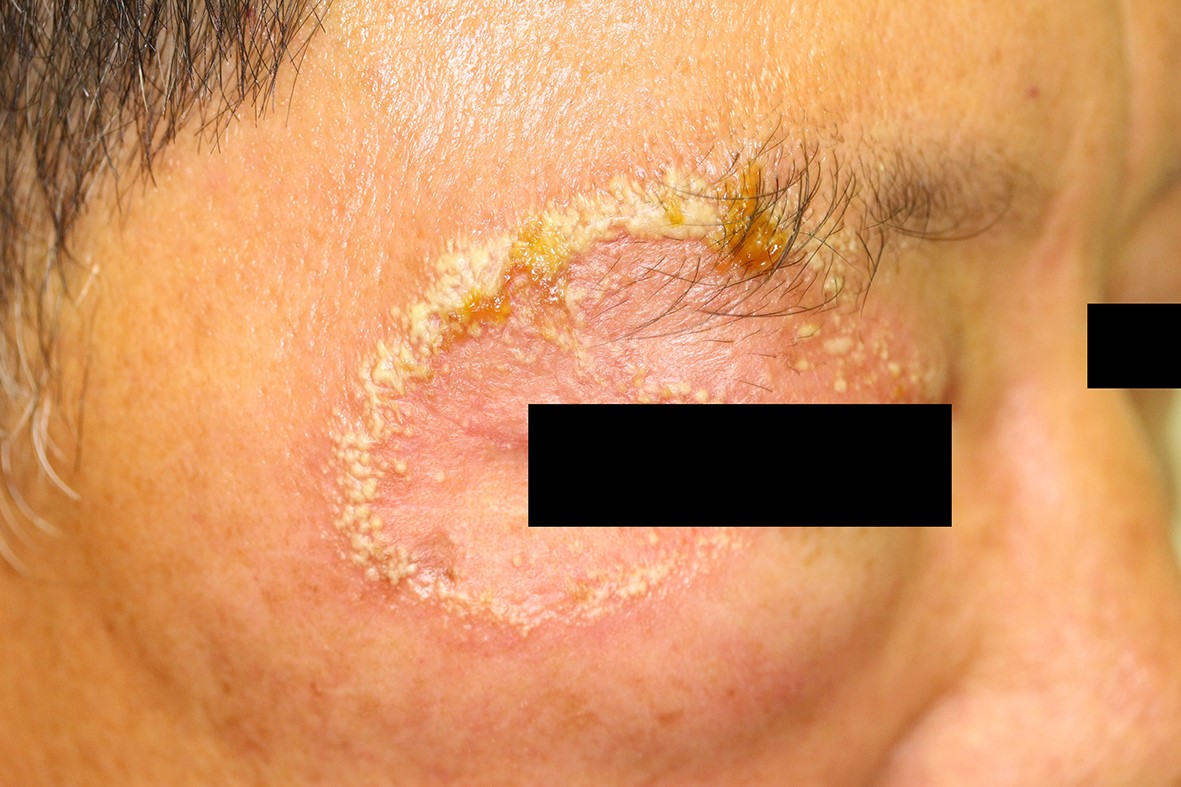
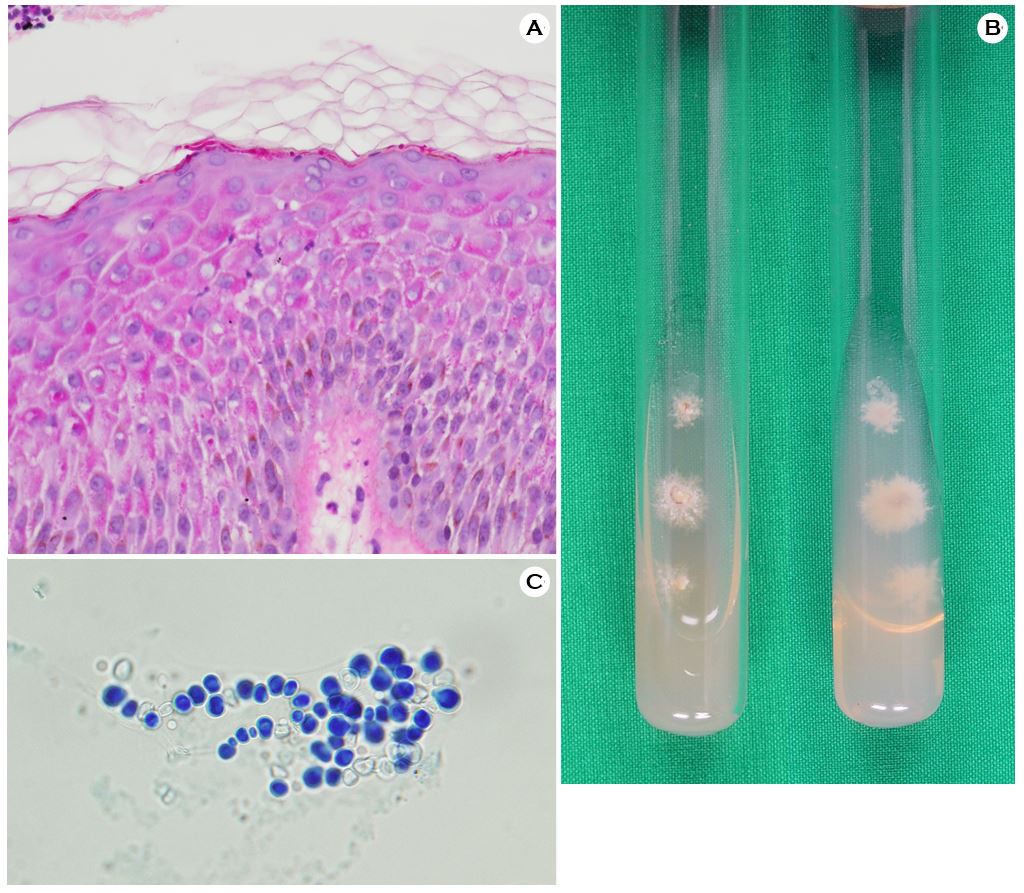
A 56-year-old male patient who is a cattle keeper presented with localized, pruritic, and 5.0×4.0-cm-sized erythematous annular plaque with central clearing and vesicular border on the right periocular area for 3 days (Fig. 1). Surgery on the right pterygium was then performed on the patient 4 days after hospital presentation. Consequently, the patient wore an eye patch for 1 day. Moreover, the patient was diagnosed and treated for contact dermatitis at a local clinic but the lesion did not improve. The result of the KOH examination on the right periocular lesion was negative. Thus, a biopsy was done for the definitive diagnosis. Histopathology showed septated hyphae in the stratum corneum (Fig. 2A). Culture from the skin biopsy specimens on Sabouraud's dextrose agar yielded slow-growing, folded, heaped, glabrous, white colonies, and lack of pigment on the reverse side after 15 days (Fig. 2B). Microscopically, the chlamydoconidia chains were observed in the slide culture (Fig. 2C). The nucleotide sequence of the internal transcribed spacer for the clinical isolate was iden- tical to that of T. verrucosum strain CBS 562.50 (GenBank accession number MH856755). The patient was treated with 100 mg of oral itraconazole daily and topical sertaconazole for 1 month. The skin lesion eventually improved completely.
Tinea faciei occurred at the periocular area and masquerade as other dermatoses. Thus, diagnosis requires a high degree of clinical suspicion. Greater awareness of this diagnosis can result in faster resolution and decreased patient exposure to unnecessary systemic and topical medications. Physicians should consider tinea faciei occurring at the periocular area in their differential diagnosis for periorbital eruptions, particularly those resistant to therapy for more prevalent conditions.
Therefore, this case is reported to emphasize the importance of fungal culture and histological examination for correct diagnosis in atypical and difficult cases.
References
1. Lin RL, Szepietowski JC, Schwartz RA. Tinea faciei, an often deceptive facial eruption. Int J Dermatol 2004;43: 437-440
Google Scholar
2. Lee MW, Yoo JY, Song YB, Suh MK, Ha GY, Kim JR, et al. Periocular tinea caused by Trichophyton rubrum. Korean J Dermatol 2013;51:997-998
Google Scholar
3. Jo JW, Jeong HB, Shin YB, Kang KR, Kim CY. Periocular allergic contact dermatitis associated with the use of ofloxacin ophthalmic ointment: a case report. Korean J Dermatol 2018;56:624-627
Google Scholar
4. Roman C, Massai L, Gianni C, Crosti C. Case reports. Six cases of infection due to Trichophyton verrucosum. Mycoses 2001;44:334-337
5. Hong JS, Lee DW, Suh MK, Ha GY, Jang TJ, Choi JS. Tinea corporis caused by Trichophyton verrucosum mimicking nummular dermatitis. J Mycol Infect 2019;24:32-34
Google Scholar
Congratulatory MessageClick here!
