pISSN : 3058-423X eISSN: 3058-4302
Open Access, Peer-reviewed
pISSN : 3058-423X eISSN: 3058-4302
Open Access, Peer-reviewed

Bom Yee Chung,Ji Min Seo,Min Ji Kang,Minho Lee,Juyoun Shin,Yeun-Jun Chung,Dong Soo Yu,Young Bok Lee
10.17966/JMI.2020.25.2.29 Epub 2020 July 03
Abstract
Background: Dermatophytes are the most common cause of fungal infections worldwide, having an estimated prevalence of 20% by the World Health Organization. Recent advances of sequencing and annotation of fungi explain the biodiversity evaluation and genomic identification of dermatophytes.
Objective: This study's objective is to assess the mycobiome and microbiome in different dermatomycoses and identify their pathogenic organisms using fungal genomic analyses. Besides, we wanted to see the topographical biodiversity in dermatomycoses.
Methods: Patients with dermatophyte infections confirmed by positive potassium peroxide examination were enrolled. Bacterial and fungal DNA were extracted from the skin sample. The internal transcribed spacer regions of rRNA gene and multiple variable regions in 16S rRNA gene were assessed to determine the fungal and bacterial community compositions.
Results: We profiled both bacterial and fungal communities in the fungal-infected skin. Dermatophyte infection resulted in modified bacterial microbiome. The alpha diversity showed that the bacterial diversity was relatively low in tinea cruris patients compared to other dermatomycoses patients. Nonetheless, fungal diversity was not impacted by the body site but by the causative fungal organisms. Tinea pedis, tinea corporis, and tinea cruris due to Trichophyton species were similar as seen in principle component analysis. Alpha diversity demonstrates the tinea corporis on the leg had the most diverse fungal mycobiome and the scalp is the least diverse area.
Conclusion: Sequencing and annotation of dermatophyte genomes of superficial skin infections will give sources that will help explain the virulence mechanisms of the dermatophyte. Understanding the pathogenesis of dermatophyte infections can help in generating effective therapeutics in the future.
Keywords
Dermatology Fungal genomics Microbiome Mycobiome Next-generation sequencing
The majority of skin microbiome studies have taken in a bacteriocentric view. Its only focus is on the diversity of bacterial species. However, fungi and viruses and also mites contribute to the human skin microbiome. Cutaneous fungal infections are mainly associated with two groups of fungi: one is the dermatophytes in the Ascomycete phylum such as the genera Trichophyton, Microsporum, and Epidermophyton, and another is Malassezia in the Blasidiomycete phylum1.
Dermatophytes are the most common cause of fungal infections in the world, resulting in treatment costs of close to half a billion dollars yearly in the USA alone. The World Health Organization estimates the global prevalence of dermatomycoses to be approaching 20%2. Nevertheless, dermatomycoses are considered a minor disease with only superficial infections. It has been lagged behind research on fungi associated with human mortality. And the pathogenesis of dermatophyte infections is not totally explored. So, we have no sophisticated understanding of skin fungal infection.
The diseases due to dermatophytes are generally named after the part of the infected body site rather than the causative organism. Tinea is a fungal infection of the skin, hair, or nails. The phrase is made by adding another term referring to a specific body location. Therefore, the term "tinea pedis" refers to a fungal infection of the feet. Other tinea infections include tinea capitis of the scalp or head, tinea corporis of the body or trunk, tinea cruris of the inguinal area, and tinea unguium of the nails. The terminology specifies that the focus is still not on the causative organism of dermatomycoses3.
Recent developments of next-generation sequencing technologies and the microbiome of several body sites, such as the skin, have been characterized and have explained the mechanisms of the virulence factor, biodiversity assessment, and genomic identification of the dermatophyte. Molecular markers for fungi, such as the rRNA gene, including 18S, 28S, internal transcribed spacer 1 (ITS1) and internal transcribed spacer 2 (ITS2) regions, and the 16S rRNA gene for bacteria, are in sequence and classify these communities.
In this manuscript, we assess the mycobiome and microbiome at the same time in different dermatomycoses and determine the pathogenic organisms with the use of fungal genomic analyses. Ultimately, we wanted to know the topographical biodiversity in dermatomycoses.
1. Subjects
Dermatophyte-associated dermatologic diseases, including tinea capitis, tinea cruris, tinea corporis, and tinea pedis, were assessed using genomic sequencing methods. Ten patients with dermatophyte infections confirmed by positive potassium peroxide (KOH) examination were enrolled in this study. The microbiome and mycobiome of the dermatophyte-infected skin were assessed. The samples were placed into a lysis buffer using a sterile cotton swab and a sterile disposable surgical blade. Bacterial and fungal DNA were extracted from the skin sample using a QIAamp DNA mini kit (Qiagen, Hilden, Germany) and MasterPure Yeast DNA purification kit (Epicentre), respectively.
2. Primers
To identify the fungal and bacterial community compositions, the internal transcribed spacer (ITS) 2 regions were amplified from purified genomic fungal DNA with the use of primers 5.8S-F (5'-GATGAAGAACGYAGYRAA-3') and 28S-R (5'-TCCTCCGCTTATTGATATGC-3'). And multiple variable regions in 16S rRNA gene from purified genomic bacterial DNA were assessed with the use of an ion torrent sequencing (Thermo Fisher Scientific).
1. Demographics of patients
Patients who came to Uijeongbu St. Mary's Hospital Dermatology Clinic due to dermatomycoses from last August to September 2019 were enrolled in this study. They were diagnosed with tinea corporis, tinea capitis, tinea pedis, and tinea cruris, confirmed with potassium hydroxide tests.
Among the 10 patients with dermatomycoses, 9 were males and 1 patient female. The mean age of the patients was 49.8 ± 22.3, including one child with tinea capitis and one adolescent with tinea cruris. The 16-year-old boy had atopic dermatitis, and one 45-year-old patient had psoriasis (Table 1).
|
Patient |
Gender |
Age |
Lesion
of |
KOH |
Fungus
culture |
Diagnosis |
Comorbid |
|
Foot
1 |
M |
45 |
Foot |
+ |
Growth
of mold |
Tinea
pedis Onychomycosis |
Psoriasis |
|
Foot
2 |
F |
66 |
Foot |
+ |
Growth
of mold |
Tinea
pedis |
None |
|
Foot
3 |
M |
48 |
Foot |
+ |
No
growth in 4 weeks culture |
Tinea
pedis Onychomycosis |
None |
|
Leg |
M |
79 |
Lower
leg |
+ |
Growth of Keissleriella sp., possibly contaminations |
Tinea
corporis Onychomycosis |
None |
|
Groin 1 (atopic der) |
M |
16 |
Groin |
+ |
Growth of mold |
Tinea cruris |
Atopic dermatitis |
|
Groin 2 |
M |
69 |
Groin |
+ |
No growth in 4 weeks culture |
Tinea pedis, Tinea cruris Onychomycosis |
None |
|
Groin 3 |
M |
42 |
Groin |
+ |
Growth of mold |
Tinea cruris, Onychomycosis |
None |
|
Buttock
1 |
M |
69 |
Buttock |
+ |
Growth
of mold |
Tinea
corporis |
None |
|
Buttock
2 |
M |
57 |
Buttock |
+ |
Growth
of mold |
Tinea
corporis |
None |
|
Scalp |
M |
7 |
Scalp |
+ |
Growth
of mold |
Tinea
capitis |
None |
2. Bacterial taxonomical analyses
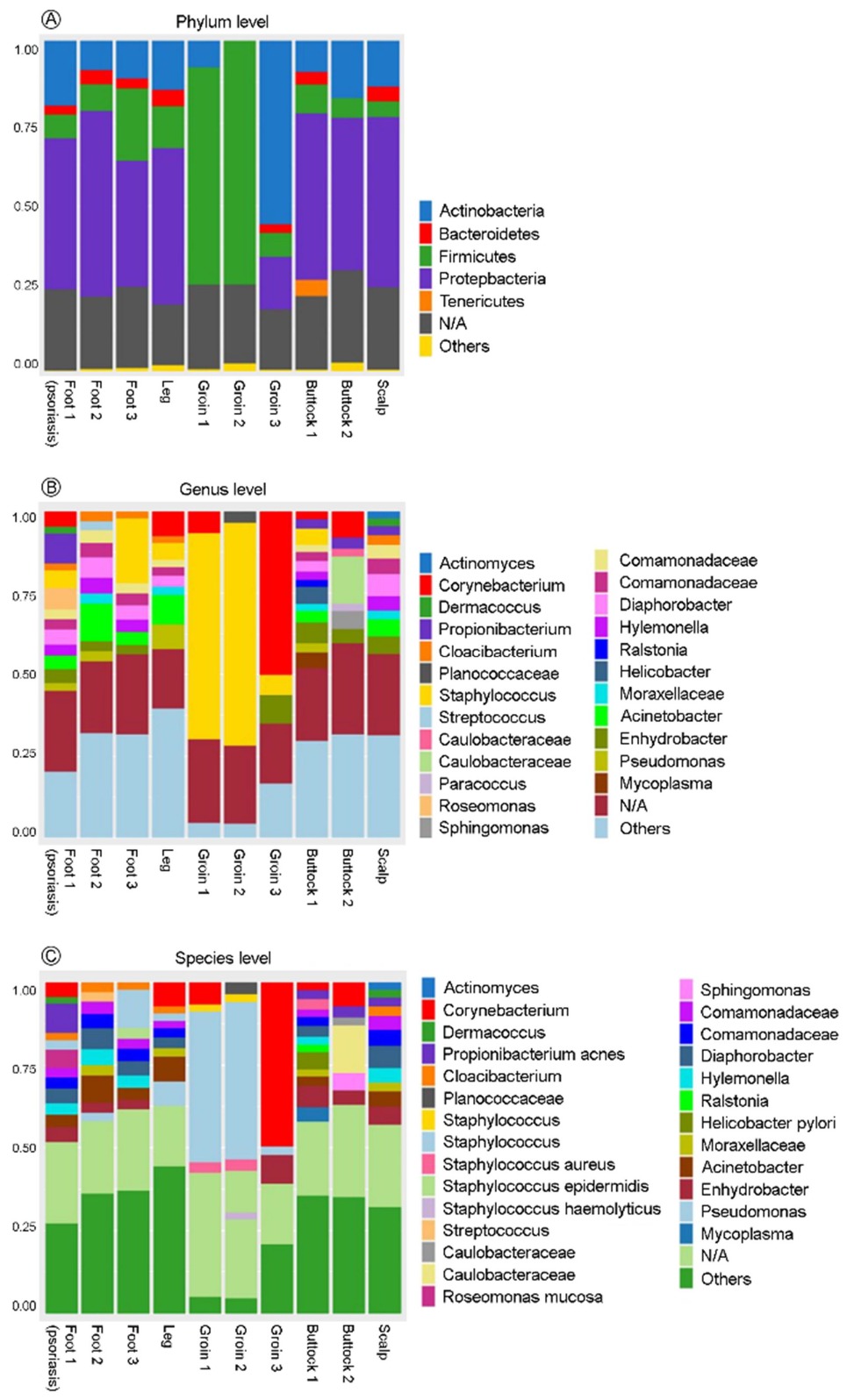
At the phylum level, Proteobacteria had the largest proportion of microbiome in tinea pedis, tinea corporis, and tinea capitis patients. However, in tinea cruris patients, Firmicutes and Actinobacteria are predominant in the groin area (Figure 1A). At the genus level, Staphylococcus and Corynebacterium are relatively predominant in tinea cruris patients. Other body sites seem to have bacterial diversity (Figure 1B). At the species level, Staphylococcus increased in tinea cruris patients. Propionibacterium acne is indicated in tinea pedis patients with psoriasis, while it is not shown in other tinea pedis patients or tinea corporis in the lower legs (Figure 1C).
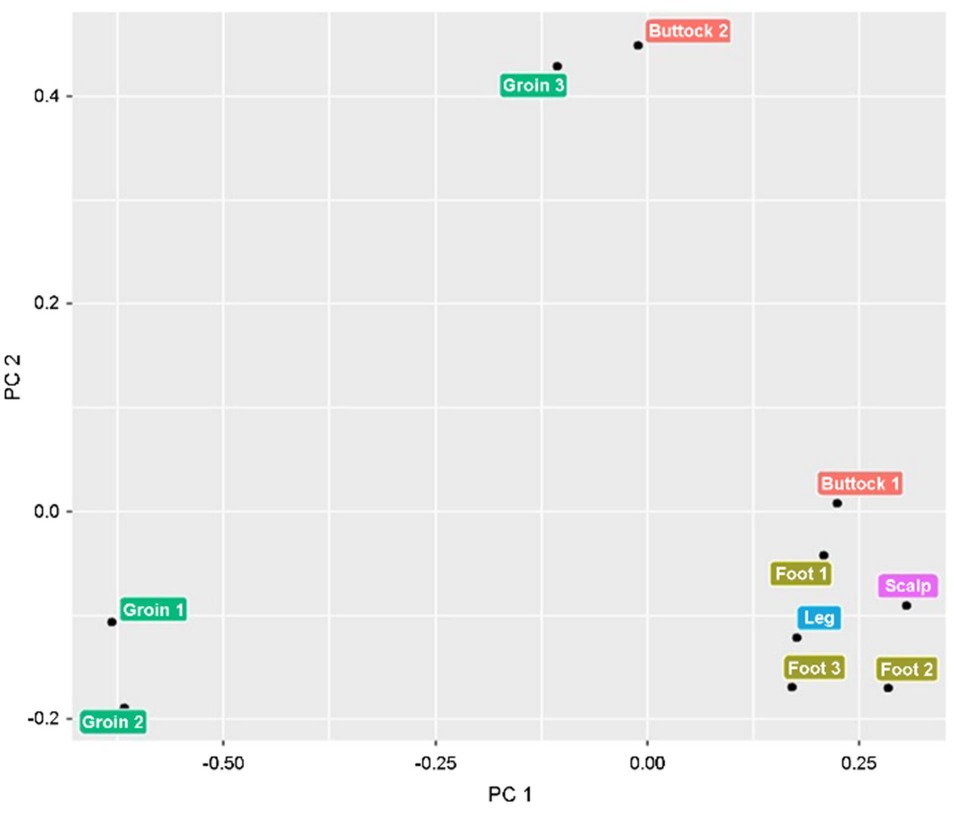
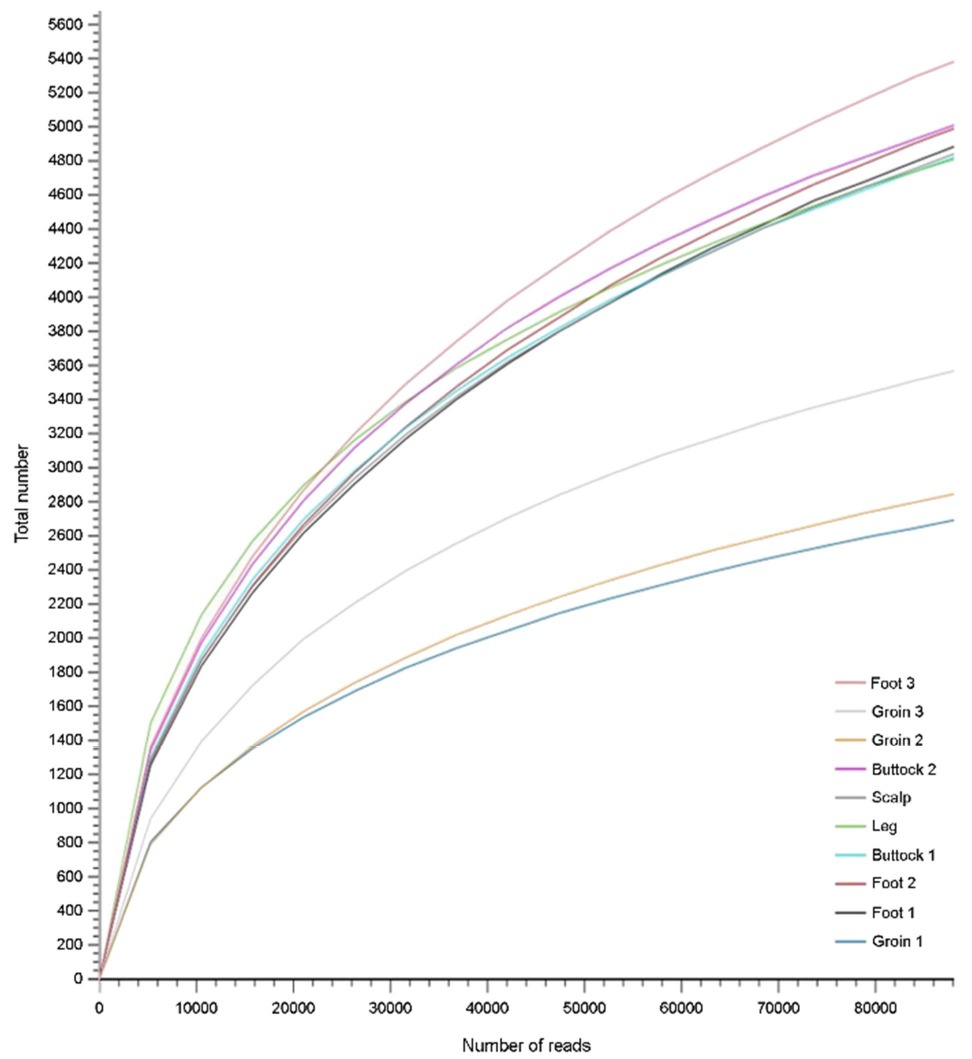
3. Principle component analysis and alpha diversity of bacterial microbiome
The principle component analysis exhibited that the bacterial microbiome of tinea cruris is varied from those of other dermatomycoses (Figure 2). Alpha diversity also showed that the bacterial diversity was relatively low in tinea cruris patients in comparison with other site dermatomycoses (Figure 3).
4. Taxonomical analyses
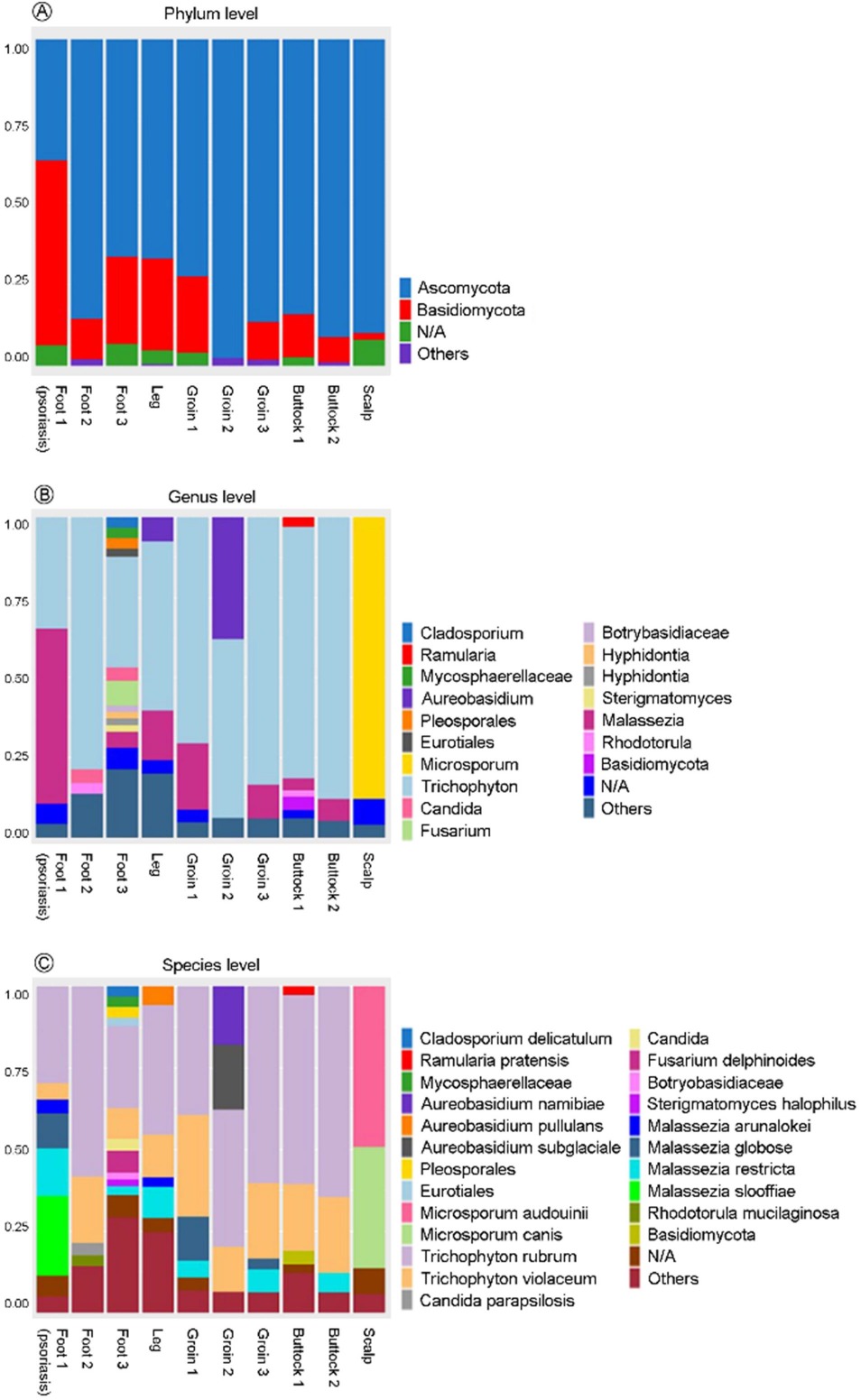
The fungal diversity of dermatomycoses patients was taxonomically classified at the phylum level. Ascomycota predominated in nine patients, and Basidiomycota is chiefly presented in one patient who had been diagnosed with tinea pedis on the foot and had comorbid psoriasis lesions on the leg (Figure 4A). At the genus level, Microsporum prevailed in a tinea capitis patient, and Trichophyton was the most predominant genus in other tinea cruris, tinea pedis, and tinea corporis patients excluding one who had been diagnosed with psoriasis and tinea pedis on the foot, which showed Malassezia to be predominant (Figure 4B). At the species level, the fungal composition of the tinea pedis patient with comorbid psoriasis exhibited that the most prevalent and pathogenic fungal organism was Trichophyton rubrum (more than 25%); however, Malassezia arunalokei, Malassezia globosa, Malassezia restricta, and Malassezia slooffiae had large proportions in the previously mentioned patient in comparison with other patients. The pathogenic organisms in a 7-year-old tinea capitis patient were Microsporum audouinii and Microsporum canis. Other dermatomycoses patients exhibited a large proportion of Trichophyton rubrum (Figure 4C).
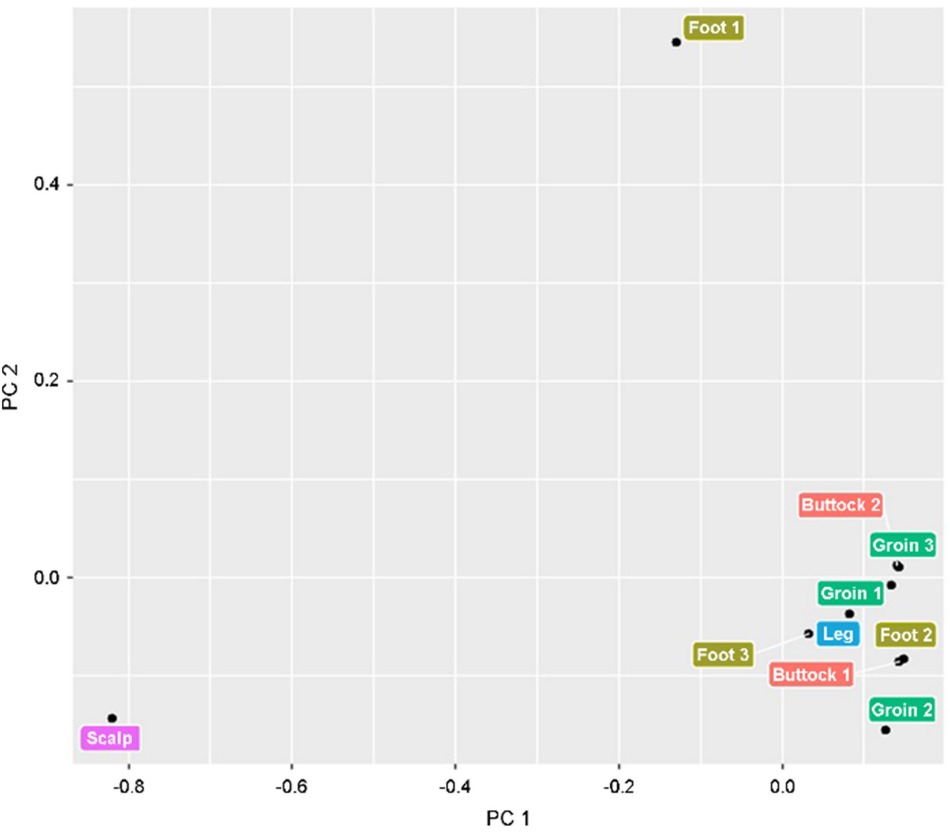
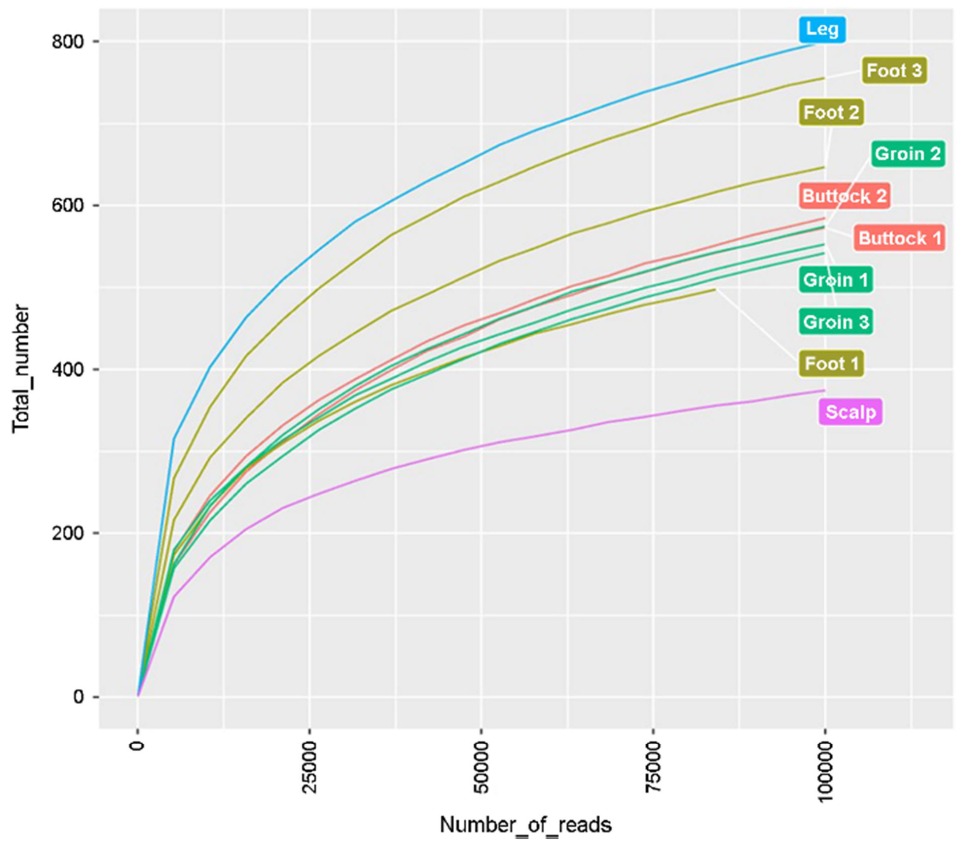
5. Principle component analysis and alpha diversity of fungal mycobiome
The principle component analysis indicated that Trichophyton rubrum-infected dermatomycoses differed from the Microsporum-infected tinea capitis patient (Figure 5). Alpha diversity shows that the tinea corporis on the leg had the most diverse fungal mycobiome and the scalp is the least diverse area (Figure 6).
This study described that the fungal diversity was similar in Trichophyton rubrum-infected dermatomycoses regardless of body sites. The modified biodiversity of bacterial microbiome might be explained by the damaged epidermal barrier due to dermatophyte infection. The condition of patients' skin and comorbid cutaneous diseases can impact the microbiome and mycobiome of the skin.
According to previously reported microbiome of the healthy skin, most skin bacteria comprise four phyla: Actinobacteria (52%), Firmicutes (24%), Proteobacteria (17%), and Bacteroidetes (7%). At the genus level, Corynebacterium in phylum Actinobacteria, Propionibacterium in phylum Actinobacteria, and Staphylococcus in phylum Firmicutes are found on the healthy skin4. When the body skin sites are split into three categories, sebaceous site, moist site, and dry site, the topographical diversity of microbiome was observed. Sebaceous sites including the scalp show the lowest bacterial diversity and isolate mainly Propionibacterium species and Staphylococcus species. And moist areas including the groin and foot preferentially have Corynebacterium species. Dry areas such as the buttock and leg have the most diverse microbial community with a greater prevalence of β-Proteobacteria and Flavobacteriales species4,5.
However, in this study, the modified microbiome was observed in dermatomycoses patients. The proportion of Staphylococcus species in microbiome increased on the inguinal area of tinea cruris patients. In normal healthy skin, the groin area is considered to have a moist condition, and Corynebacterium species are predominant in this site. That discrepancy might be influenced by the impaired epidermal barrier function of tinea cruris infection. Propionibacterium acne is predominant in greasy areas, for instance, the scalp, while the proportion of Propionibacterium acne was relatively low on the scalp of tinea capitis patients. Unexpectedly, Propionibacterium acne was seen in tinea pedis patients with psoriasis, whereas it was not shown in other tinea pedis patients. That might be explained by the topical ointment use in psoriasis patients.
In comparison to previously reported microbiome of the healthy skin, the microbiome of the dermatomycoses is more diverse and different than of the healthy skin. That might be the pathogenic role of fungal infection that damages the skin barrier function. Dermatophyte infection resulted in modified bacterial microbiome. The alpha diversity showed that the bacterial diversity was relatively low in tinea cruris patients in comparison with other site dermatomycoses.
Meanwhile, both ascomycetous and basidiomycetous fungi were determined in normal healthy skin. The genus Malassezia is predominant in all core body and arm sites6. However, in this study, Malassezia only predominated at the foot of the tinea pedis patient who had been treated with comorbid psoriasis. The tinea capitis patient principally exhibited colonization of Microsporum spp. Other dermatomycoses patients exhibited predominant colonization of Trichophyton rubrum.
In this study, fungal diversity was impacted not by body sites but by the causative fungal organisms. Tinea pedis, tinea corporis, and tinea cruris due to Trichophyton species exhibited a similarity, using the principle component analysis. Alpha diversity shows that the tinea corporis on the leg had the most diverse fungal mycobiome and the scalp is the least diverse area.
This study has various limitations as follows: The analysis was only of patients, with no healthy control comparison. We also did not compare the microbiomes before and after antifungal treatment. The number of patients was too small to find significant conclusions.
On the basis of these results, we propose that the causative organisms of dermatomycoses are more important than the infected body sites. There are still several things to be analyzed for cutaneous fungal diseases using genomic studies. Sequencing and annotation of dermatophyte genomes of superficial skin infections will give sources that will help in explaining the mechanisms of virulence of the dermatophyte. The understanding of pathogenesis of dermatophyte infections can design the effective therapeutics in the future.
References
1. White TC, Findley K, Dawson TL, Jr., Scheynius A, Boekhout T, Cuomo CA, et al. Fungi on the skin: dermatophytes and Malassezia. Cold Spring Harb Perspect Med 2014;4
Google Scholar
2. Achterman RR, White TC. Dermatophyte virulence factors: identifying and analyzing genes that may contribute to chronic or acute skin infections. Int J Microbiol 2012;2012: 358305
Google Scholar
3. White TC, Oliver BG, Gräser Y, Henn MR. Generating and testing molecular hypotheses in the dermatophytes. Eukaryot Cell 2008;7:1238-1245
Google Scholar
4. Grice EA, Kong HH, Conlan S, Deming CB, Davis J, Young AC, et al. Topographical and temporal diversity of the human skin microbiome. Science 2009;324:1190-1192
Google Scholar
5. Lee YB, Byun EJ, Kim HS. Potential role of the microbiome in acne: A comprehensive review. J Clin Med 2019;8:987
Google Scholar
6. Findley K, Oh J, Yang J, Conlan S, Deming C, Meyer JA, et al. Topographic diversity of fungal and bacterial communities in human skin. Nature 2013;498:367-370
Google Scholar
Congratulatory MessageClick here!
