pISSN : 3058-423X eISSN: 3058-4302
Open Access, Peer-reviewed
pISSN : 3058-423X eISSN: 3058-4302
Open Access, Peer-reviewed

Sae Rom Chung,Hye Soo Lee,In Cheon You
10.17966/JMI.2018.23.1.24 Epub 2018 April 01
Abstract
A 74-year-old man presented with pain and progressively worsening vision from 20 days ago in the left eye. His ophthalmological history was significant for cataract extraction, scleromalacia, and three surgeries for pterygium removal in the left eye. Slit-lamp examination was remarkable for a 4.5×4.0 mm sized epithelial defect, with corneal stromal infiltration and melting and a surrounding feathery margin. Corneal scraping was performed, and culture of specimen demonstrated mold that grew on Sabouraud dextrose agar. The isolate was finally identified as Corynespora cassiicola based on DNA sequencing analysis of internal transcribed spacer (ITS) with maximum identity of 100%. The patient was treated successfully with intracameral amphotericin B injection and topical voriconazole and amphotericin B. To the best of our knowledge, this is the first reported case of mycotic keratitis caused by a plant pathogen, Corynespora cassiicola, in Korea.
Keywords
Corynespora cassiicola Fungus Keratitis Plant pathogen
Corynespora cassiicola is a major plant pathogen that is associated with target spot disease on stems, fruits, and flowers of multiple host plants[1],[2]. In 1969, this organism was first reported to cause maduromycetoma of the foot in Sudan[3]. Two recent reported cases of subcutaneous infection caused by Corynespora cassiicola have been documented and one corneal infection by this organism was reported in Japan[4]. This is the first case of corneal infection caused by Corynespora cassiicola in Korea. We describe a case of corneal ulceration due to Corynespora cassiicola.
A 74-year-old man was admitted complaining of pain and progressively decreased visual acuity from 20 days ago in the left eye. He had hypertension and had received oral antihypertensive treatment for 8 years. He had undergone three surgeries for pterygium removal in his left eye. He also underwent cataract extraction and intraocular lens implantation in the left eye. He had relatively poor vision in his left eye due to focal scleromalacia, corneal thinning, and opacity.
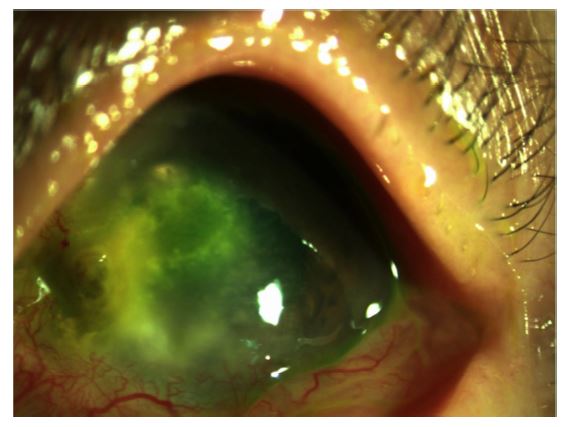
He was a farmer. He had not noticed any obvious injury or foreign body impaction. He did, however, wipe the sweat off his brow with the back of his dirty hand at work. On initial examination, visual acuity was 20/25 (0.8) in the right eye and 20/250 (0.08) in the left eye. The left eye had a 4.5×4.0 mm sized epithelial defect and underlying stromal infiltration with surrounding feathery margin (Figure 1). There was an associated endothelial plaque along the lower ulcerative margin. The right eye was normal.
Corneal scraping for smears and cultures was performed. A corneal scraping revealed hyphae on 10% potassium hydroxide (KOH) smear. He was started on topical fluconazole every hour, moxifloxacin every 2 hours, and homatropine three times daily. Two days later, topical amphotericin B and 100 mg of systemic fluconazole twice daily were added. One week of this therapy resulted in no appreciable response. The stromal infiltration and endothelial plaque remained as previously described, and cyclitic membrane in the anterior chamber was newly appeared.
Culture of the corneal scraping revealed mold that grew well on Sabouraud dextrose agar and formed velvety and olive colonies after seven days of incubation at 28℃ (Figure 2). Microscopically, the organism exhibited long, straight, and separate conidiophores and catenate conidia on lactophenol cotton blue stain (Figure 3). The isolate was further identified to the species level by DNA sequencing analysis of internal transcribed spacer (ITS) regions. The isolate was finally identified as Corynespora cassiicola based on sequencing analysis with maximum identity of 100% (535/535).


Topical fluconazole was changed to topical voriconazole, and 5 μg of amphotericin B in 0.1 mL was injected into the anterior chamber. The patient responded well, and the cyclitic membrane and the endothelial plaque started to decrease. The anterior chamber reaction and stromal edema resolved gradually. All medications were progressively reduced and discontinued after 3 months of treatment. Six months later, focal corneal thinning and a mild central corneal scar were visible, and visual acuity was 20/100 (0.2) in the left eye.
Corynespora cassiicola is a common causative agent of target leaf spot disease of grasses and other herbaceous plants in tropical and subtropical climate zones, including China[5],[6]. Crops, such as cucumber, papaya, perilla, rubber, soybean, and tomato, suffer the greatest yield loss due to this fungus[1],[5],[7]. Cassiicolin, a 27-residue O-glycosylated phytoxin produced by C. cassiicola, is responsible for leaf fall disease and induces cellular damage identical to that caused by fungus on rubber tree leaves[7]. As a pathogen, C. cassiicola infects plant leaves, stem, and roots; and has been isolated from nematodes. Pathogenicity varies depending on the host and some isolates can infect multiple hosts while others appear to be host specific[8]. Human infections are extremely rare, less than 10 cases of human infections have been reported including three cases of subcutaneous infections and one corneal infection[1]-[3]. Huang et al.[1] and Lv et al.[2] reported successful treatment of subcutaneous infection of C. cassiicola with systemic amphotericin B and oral terbinafine with topical povidone iodine.
C. cassiicola is a member of Pleosporales and, as with many species of this order, is a major plant pathogen[2]. Only very few plant pathogens have thus far been found to be involved in human infection, and C. cassiicola appears to be one of them. Most species of Bipolaris, Curvularia, Exserohilum, and Alternaria that are causative agents of human infection are related to saprobic members of this genera[9]. With the increasing use of molecular methods in clinical laboratories, especially DNA sequencing analysis, identification of rare melanized fungi are greatly facilitated. Identification of C. cassiicola was made based on its microscopic features in culture, and was then confirmed by molecular analysis. Major diagnostic characteristics of C. cassiicola were the long pseudoseptate conidia, very wide, flat basal scars, and slow maturation in the apical region[10].
In our case, the mold was identified as C. cassiicola according to the characteristic phenotypes and relevant molecular methods (DNA sequencing analysis of the ITS regions). The appropriate treatment of these infections is not well established. In our case, the patient was treated successfully with topical voriconazole and amphotericin B, the addition of intracameral injection of amphotericin B was especially effective. The patient had obvious contact with plants. It is postulated that the patient had acquired the infection through the hands by handling the plants probably soybean or cucumber. Old age, ocular surface irregularity due to prior pterygium surgery, and agricultural activity partially predisposed the patient to developing this opportunistic fungal keratitis.
In relation to this article, I declare that there is no conflict of interest.
References
1. Huang HK, Liu CE, Liou JH, Hsiue HC, Hsiao CH, Hsueh PR. Subcutaneous infection caused by Corynespora cassiicola, a plant pathogen. J Infect 2010;60:188-190
Crossref
Google Scholar
2. Lv GX, Ge YP, Shen YN, Li M, Zhang X, Chen H, et al. Phaeohyphomycosis caused by a plant pathogen, Coryne- spora cassiicola. Med Mycol 2011;49:657-661
Crossref
Google Scholar
3. Mahgoub E. Corynespora cassiicola, a new agent of mad- uromycetoma. J Trop Med Hyg 1969;72:218-221
Crossref
Google Scholar
PubMed
4. Yamada H, Takahashi N, Hori N, Asano Y, Mochizuki K, Ohkusu K, et al. Rare case of fungal keratitis caused by Corynespora cassiicola. J Infect Chemother 2013;19:1167 -1169
Crossref
Google Scholar
5. Lee HB, Kim CJ, Mun HY. First report of stem blight on perilla (Perilla frutescens) caused by Corynespora cassiicola in Korea. Plant Dis 2009;93:550
Crossref
Google Scholar
6. Qi YX, Xie Y, Zhang X, Pu J, Zhang H, Huang S, et al. Molecular and pathogenic variation identified among isolates of Corynespora cassiicola. Mol Biotechnol 2009; 41:145-151
Crossref
Google Scholar
7. de Lamotte F, Duviau MP, Sanier C, Thai R, Poncet J, Bieysse D, et al. Purification and characterization of cassiicolin, the toxin produced by Corynespora cassiicola, causal agent of the leaf fall disease of rubber tree. J Chromatoqr B Analyt Technol Biomed Life Sci 2007;849: 357-362
Crossref
Google Scholar
8. Shrestha SK, Lamour K, Young-Kelly H. Genome sequences and SNP analyses of Corynespora cassiicola from cotton and soybean in the southeastern United States reveal limited diversity. PLoS ONE 2017;12: e0184908.https:// doi.org/10.1371/journal.pone.0184908
Crossref
Google Scholar
9. Revankar SG, Sutton DA. Melanized fungi in human dis- ease. Clin Microbiol Rev 2010;23:884-928
Crossref
Google Scholar
PubMed
10. de Hoog GS, Guarro J, Genè J, Figueras MJ. Atlas of Clinical Fungi, 2nd ed. Utrecht: Centraalbureau voor Schimmelcultures, 2000:596-597
Crossref
Congratulatory MessageClick here!
