pISSN : 3058-423X eISSN: 3058-4302
Open Access, Peer-reviewed
pISSN : 3058-423X eISSN: 3058-4302
Open Access, Peer-reviewed

Hyeong Mok Kwon,Hye Ri Kim,Dong Hoon Shin,Jong Soo Choi
10.17966/JMI.2020.25.1.22 Epub 2020 April 07
Abstract
Tinea pseudoimbricata, a special subset of tinea incognito, is a cutaneous fungal infection with unusual tinea imbricata-like lesions caused by dermatophytes other than Trichophyton concentricum. Here we present a case of tinea pseudoimbricata. An 80-year-old woman presented with mildly pruritic, scaly, annular, erythematous plaques with inner small, annular, polycyclic, or arcuate plaques on the left abdomen and back for 1 month. The lesions enlarged after the application of topical corticosteroids about 2 months previously. A potassium hydroxide test performed on her lesions was positive. Fungal culture, light microscopic findings, and T. rubrum-specific real-time polymerase chain reaction confirmed the presence of T. rubrum. Thus, we diagnosed tinea pseudoimbricata caused by T. rubrum and treated successfully with oral and topical terbinafine.
Keywords
Tinea incognito Tinea pseudoimbricata
Tinea incognito is a cutaneous fungal infection that often has atypical clinical features and is attributed to the prior use of immunosuppressive agents, usually topical or systemic corticosteroids1. Tinea imbricata is a chronic superficial mycosis, and in some regions, it is an endemic superficial mycosis caused by Trichophyton (T.) concentricum3. Tinea pseudoimbricata is a special form of tinea incognito, which involves dermatophytosis caused by dermatophytes other than T. concentrium, showing unusual tinea imbricata-like lesions. This is similarly termed as tinea atypica in Italy4 and tinea indecisiva in India5; however, these different terms with different meanings could confuse health care providers. Here we report a case of tinea pseudoimbricata.
An 80-year-old woman visited our clinic with a complaint of pruritic skin rash on her trunk. She presented with a mildly pruritic annular, erythematous, scaly plaque, measuring 30 cm in diameter, with inner small annular, polycyclic, arcuate plaques on the left abdomen and back (Figure 1A, 1B) for 1 month. The lesions enlarged after the application of topical corticosteroids administered by a local medical center approximately 2 months ago. In addition, she had hypertension and dyslipidemia.

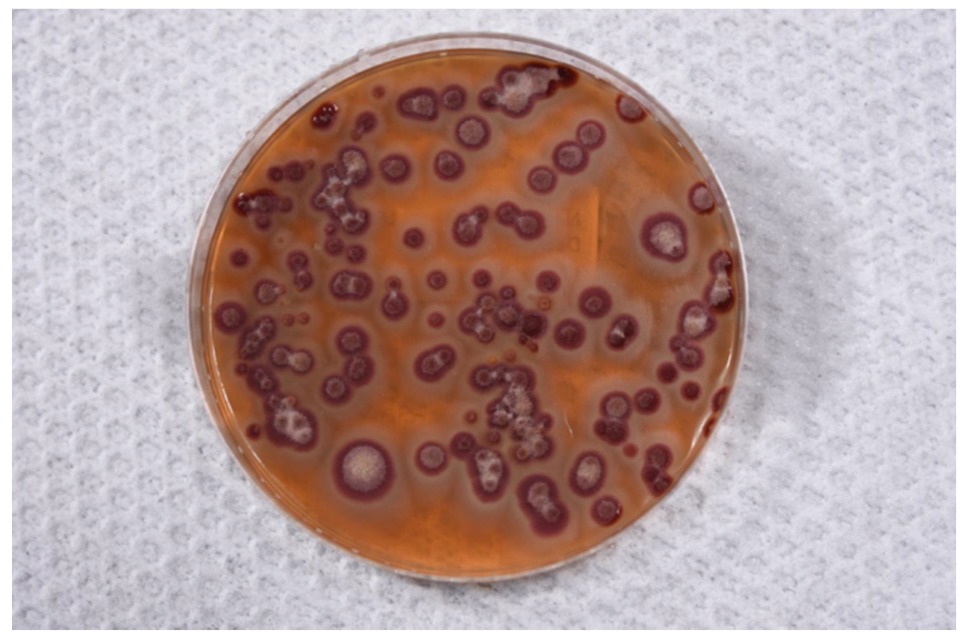
A potassium hydroxide test performed on the skin lesions was positive, and several fungal hyphae were observed. A specimen obtained from the lesions was inoculated in Sabouraud dextrose agar and cultured at 28℃ for 2 weeks, and deep red colonies developed (Figure 2). Using a light microscope, septate and branched hyphae and teardrop-shaped microconidia were observed, and the presence of T. rubrum was finally confirmed via T. rubrum-specific real-time polymerase chain reaction using Real Fungus-ID® (Optipharm M&D, Wongju, Korea). Thus, we diagnosed tinea pseudoimbricata caused by T. rubrum; further, 3 weeks after using an oral antifungal agent (terbinafine, 250 mg) and a topical antifungal agent (terbinafine), the lesions greatly improved, and there was no evidence of recurrence for 1 year.
Tinea incognito is a dermatophytosis that often has atypical clinical features and is attributed to the prior use of systemic or topical corticosteroids or other immunomodulating agents1. In general, tinea incognito may lack the scale and elevated margin, which is typical of dermatophytosis. It tends to be extensive, pruritic, erythematous, and pustular and can be mistaken for other skin disorders, particularly atopic dermatitis2.
Tinea pseudoimbricata, a special subset of tinea incognito, has morphological similarity to tinea imbricata. Tinea imbricata is a chronic superficial mycosis caused by T. concentricum with a characteristic pattern of concentric and/or annular plaques, erythema, and scales, with a restricted geographical distribution in the South West Pacific, Southeast Asia, and Central and South America3. The term "imbricata" is derived from the Latin word "imbrex" and refers to overlapping roof tiles. Cases clinically simulating tinea imbricata but caused by species other than T. concentricum have been labeled as "tinea pseudoimbricata", which is similarly termed as tinea atypica in Italy4 and tinea indecisiva in India5. The terms "atypica" and "indecisiva" may have originated from atypical and indecisive concentric lesions, respectively, of superficial mycosis caused by species other than T. concentricum. Considering the origins of each term, "tinea pseudoimbricata" would be the most specific term referring to these mycotic infections other than tinea atypica and tinea indecisiva6. Tinea pseudoimbricata is usually caused by T. tonsurans, T. mentagrophytes, Microsporum (M.) gypseum, and M. ferrugineum. Moreover, this tinea imbricata-like or a "ring-within-a-ring" appearance has been rarely reported, secondary to topical corticosteroid misuse, or some form of underlying immunosuppression, such as protein-energy malnutrition, HIV infection, or immunosuppressive therapy following transplantation. Because tinea pseudoimbricata has a specific morphology and implicates underlying immunosuppressive status far more than tinea incognito, authors and clinicians can distinguish these terms5.
During dermatophytic invasion, digestion of keratin by the fungus is associated with the secretion of multiple proteases, which play their particularly specialized roles in colonizing and degrading keratinized host structures during infection. The host's defense mechanism depends on both innate and acquired T-cell-mediated immune systems. In genetically susceptible populations of endemic areas, multiple concentric rings of tinea imbricata are hypothesized to result from negative delayed-type hypersensitivity to T. concentricum cytoplasmic antigens and T-lymphocyte hyporeactivity. A ring effect observed in cases of topical corticosteroid misuse may be explained by the fact that although the host reaction occurs in response to actively metabolizing fungal cells, the fungal cells are initially only partly inhibited. When the host's local immune responses decline below a certain threshold, the fungal genes are activated again and initiate another host-induced inflammatory response; this is repeated many times, resulting in several concentric rings of inflammation, which clinically manifest as annular erythema and scaling6.
A total of five cases, including this one, that presented with several concentric rings of tinea imbricata after using topical corticosteroids have been reported in South Korea (Table 1)7-10. Most of these cases occurred in the extremities, except for the present case, and the pathogens were T. rubrum in two cases, T. verrucosum in another two cases, and M. ferrugineum in only one case. All cases were well treated with topical and oral antifungal agents.
|
Case |
Sex/ |
Location |
Morphology |
Pathogen |
Treatment |
|
1987 |
M/9 |
Right forearm |
7~8 concentrically arranged rings of scales forming
an annular patch
|
M.
ferrugineum
|
Topical bifonazole and ciclopirox for |
|
2000 |
M/19 |
Right forearm |
Concentrically arranged rings of |
T. rubrum |
Oral itraconazole for 2 weeks |
|
2006 |
M/7 |
Right thigh |
A solitary, 5.0 × 5.0 cm sized, |
T. verrucosum |
Oral terbinafine and topical lanoconazole |
|
2008 |
F/69 |
Right forearm |
A solitary, 5.0 × 5.0 cm sized, |
T. verrucosum
|
Oral terbinafine and topical lanoconazole |
|
Present |
F/80 |
Left abdomen |
Annular
erythematous scaly plaque |
T. rubrum
|
Oral and
topical terbinafine |
The patient provided written informed consent for the publication and the use of his or her images.
References
1. Stringer T, Gittler JK, Orlow SJ. Tinea incognito in an urban pediatric population. Cutis 2018;102:370-372
Google Scholar
2. Veraldi S, Giorgi R, Pontini P, Tadini G, Nazzaro G. Tinea imbricata in an Italian child and review of the literature. Mycopathologia 2015;180:353-357
Google Scholar
3. Leung AKC, Leong KF, Lam JM. Tinea imbricata. J Pediatr 2018;200:285-285.e1
Google Scholar
4. Atzori L, Pau M, Aste N. Tinea atypica. G Ital Dermatol Venereol 2013;148:593-601
Google Scholar
5. Singal A, Jakhar D, Kaur I, Pandhi D, Das S. Tinea pseudoimbricata as a unique manifestation of steroid abuse: A clinico-mycological and dermoscopic study from a tertiary care hospital. Indian Dermatol Online J 2019;10:422-425
Google Scholar
6. Kansal NK. Tinea pseudoimbricata: A striking
Google Scholar
7. Lee H, Lee ES, Kang WH, Lee SN. An unusual clinical manifestation of tinea corporis caused by Microsporum ferrugineum. Korean J Dermatol 1987;25:383-388
Google Scholar
8. Roh DK, Park CJ, Yi JY, Lee HK. A case of tinea corporis showing tinea imbricate-like clinical appearance. Korean J Med Mycol 2000;5:20-23
9. Lim JW, Lee YH, Suh MK, Ha GY, Kim JR. A case of tinea corporis caused by Trichophyton verrucosum showing tinea imbricata-like clinical appearance. Korean J Dermatol 2006;44:318-321
Google Scholar
10. Kang GS, Go WT, Suh MK, Ha GY, Lee JI. A case of tinea corporis caused by Trichophyton verrucosum showing tinea imbricata-like clinical appearance. Korean J Med Mycol 2008;13:181-186
Google Scholar
Congratulatory MessageClick here!
