pISSN : 3058-423X eISSN: 3058-4302
Open Access, Peer-reviewed
pISSN : 3058-423X eISSN: 3058-4302
Open Access, Peer-reviewed
Yong Woo Choi,Hye Ri Kang,Joonsoo Park,Hyung Joon Kim
http://dx.doi.org/10.17966/KJMM.2017.22.4.186 Epub 2017 December 22
Abstract
Keywords
Fungal keratitis Mycotic keratitis Slit lamp examination
Mycotic keratitis (MK) is a fungal infection to the cornea and has been recognized prevalently in young outdoor workers[1]. MK typically arises from filamentous fungi including Fusarium, Aspergillus, Phaeohyphomycetes and yeast-forming candidal species[1]. Prominent clinical feature of MK presents in ulcerative changes which may progress into irreversible corneal damage. Imaging techniques such as confocal microscopy and anterior segment optical coherence tomography may be used to construe MK[1]. However, mycological evaluation particularly microscopic examination under potassium hydroxide mount and culture of corneal material still remain the cornerstones of diagnosis[1].
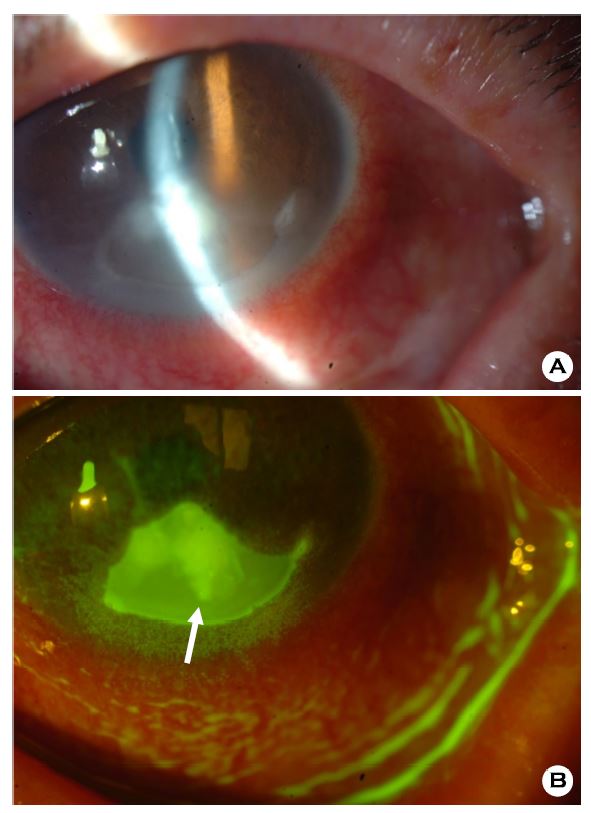
In slit lamp examination, raised edges overlying epithelial defect and hyphate edges are shown in the lower part of the corneal ulcer and conjunctival injection is also pronounced (Fig. 1A). Other features of mycotic keratitis reveal a whitish to grayish infiltrates with feathery borders[2]. Satellite lesions of hypopyon, conjunctival injection and purulent secretions may be noticed as well[2]. Ulcers caused by yeasts present in plaques with slightly more defined borders similar to that of bacterial keratitis[2]. Fluorescein staining may be conducive in identifying corneal epithelial defects. The fluorescein dye retention, observed in green, is more intense and uniform across the ulcers in fungal infeciton[3]. As presented in this image, the center of ulcer shows a homogenous nature indicative of MK (Fig. 1B).
Although, fungal infection must be confirmed through microscopic evaluation under potassium hydroxide mount and fungal cultures, slit lamp examination and fluorescein staining generate a sound evaluative measure for MK.
References
1. Ibrahim MM, Vanini R, Ibrahim FM, Fioriti LS, Furlan EM, Provinzano LM, et al. Epidemiologic aspects and clinical outcome of fungal keratitis in southeastern Brazil. Eur J Ophthalmol 2009;19:355 -361
Google Scholar
2. Dahlgren M, Lingappan A, Wilhelmus K. The clinical diagnosis of microbial keratitis. Am J Ophthalmol 2007;143:940-944
Crossref
Google Scholar
3. Shields T, Sloane PD. A comparison of eye problems in primary care and ophthalmology practices. Fam Med 1991;23:544-546
Google Scholar
