pISSN : 3058-423X eISSN: 3058-4302
Open Access, Peer-reviewed
pISSN : 3058-423X eISSN: 3058-4302
Open Access, Peer-reviewed
Osung Kwon,Hyejoo Ra,Jaehan Park,Joonsoo Park
http://dx.doi.org/10.17966/KJMM.2017.22.4.182 Epub 2017 December 22
Abstract
Keywords
Fungal meningitis has been recognized as a rarer clinical entity that heavily depends on the immunity of the host and virulence factors of fungi[1]. However, incidence of fungal meningitis continues to expand as susceptible risk factors such as organ transplants, chemotherapies, acquired immunodeficiency syndromes increase[2]. An aggressive diagnostic approach through various modalities and subsequent antifungal therapy is imperative to reduce morbidity and mortality.
An 80-year-old male patient was brought to the emergency department complaining of confusion for the past day. The patient was admitted at a secondary-based hospital due to fever and progressive weakness associated with poor oral intake for the past 10 days. Other than chronic hepatitis C infection, the patient was in good health. Neurological evaluation confirmed of drowsy mental status combined with disorientation and speech impairment. Other than fever (38.3℃), leukocytosis (14,900/ mm3) and hyponatremia (122 mEq/L), vital signs and routine laboratory test were within normal limits. Non-enhanced views of computed tomography (CT) revealed no specific hemorrhages or bony abnormalities.
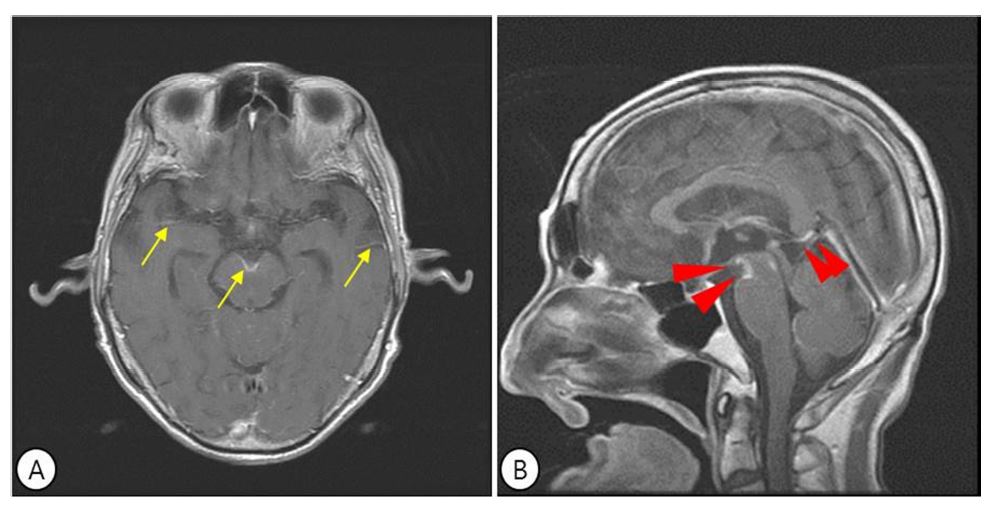
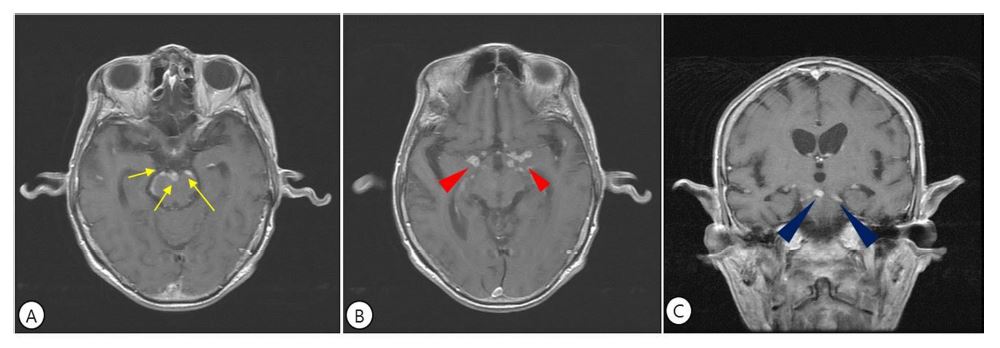
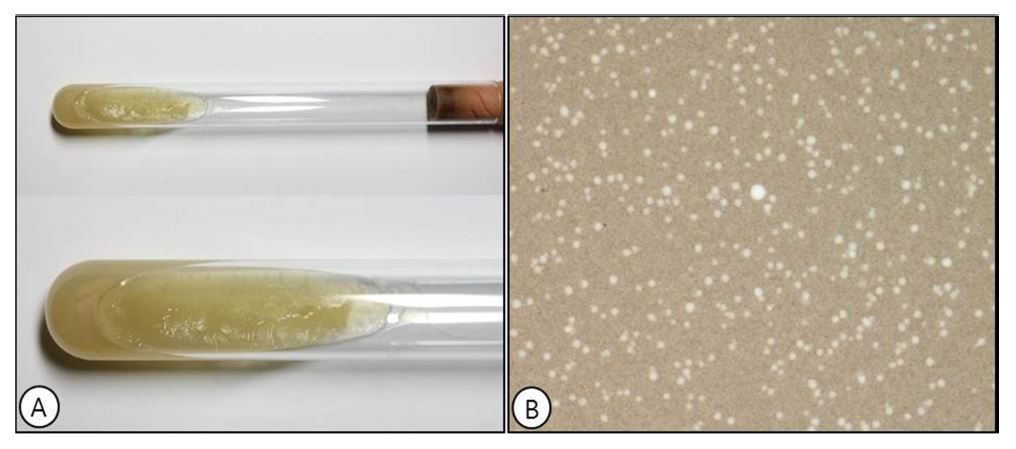
Magnetic resonance imaging (MRI) with T1 weighted gadolinium enhanced image revealed prominent leptomeningeal enhancement of pial surface ambient to cistern and cerebral hemisphere (Fig. 1A, 1B). The nature of the enhancement exhibited smooth, thick, and irregularly discontinuous in nature. Concomitant cerebrospinal fluid (CSF) analysis (leukocyte 90/HPF, PMN 30/HPF, lymphocytes 70/HPF, erythrocytes 60/HPF, glucose 31 mg/dl (serum glucose 102 mg/dl), protein 160.3 mg/ dl) was not consistent with that of viral meningitis and empirical intravenous ceftriaxone 2 g and oral azithromycin 500 mg was started. Cryptococcus antibody along with fungal culture, however, was also tested upon irregularity of focally thickened leptomeningeal enhancement observed in MRI. After administration of intravenous antibiotics for one week, fever persisted and mental confusion did not improve. Follow-up MRI performed and was correlated a higher degree of fungal infection. Multiple patchy nodular enhancement in the basal and perimesencephalic cisterns were more definitive of fungal meningitis (Fig. 2A, 2B, 2C). The fungal infectivity was confirmed by positive Cryptococcus immunoglobulin test and the medication was changed to intravenous amphotericin B (60 mg) and fluconazole (400 mg). Colonies of the fungal culture exhibited shiny light brownish color with mucoid texture and presented highlighted capsules under direct microscopy of India ink, consistent with that of Cryptococcus (Fig. 3A, 3B). Subsequent improvement of in CSF study was observed after 3 weeks of antifungal therapy.
Fungal meningitis is known as a mycotic infection to the central nervous system (CNS)[3]. Immunity and age are the two most important risk factors of the entity. It is prevalently caused by yeasts especially; Cryptococcus and positive antibody to the organism through CSF analysis generates a confirmative diagnosis[4]. Although the diagnosis based on mycological evaluation, neuroimaging exhibits diagnostic value as disease correlation is observed over 40% of the patients[5],[6],[7].
CT scans are regarded nonspecific in most cases for CNS cryptococcosis as 43% of the patients demonstrated unremarkable findings in a retrospective study[8]. MRI provides a more sensitive diagnostic tool for the study[9]. While typical enhancement of the meninges is thin, symmetric, linear, and discontinuous leptomeningeal enhancement in fungal infection may exhibit thicker and nodular nature with poor demarcations[1]. The Cryptococci produce a mucoid material in inflammatory response and deposition of thick gelatinous exudates containing inflammatory cells, fibrin, and clotted materials also prone to developing arachnoiditis[10],[11]. The perivascular spaces may be enlarged as a result of the production of voluminous mucoid material and invites a number of differentials including tuberculosis, sarcoid, or meningeal carcinomatosis[1]. However the imaging appearance of smooth and nodular leptomeningeal enhancement is often encountered in fungal infections and generates further confirmative measures for mycological elucidation.
In the present case, the patient was not immunologically challenged and the laboratory results including CSF study was insufficient to indicate that of a fungal infection. Neurological abnormalities were masked by senility and hyponatremia for muscular weaknesses. Empirical coverage of antibiotics is prevalently administered upon CSF study inconsistent with viral meningitis. However, the insidious nature along with pictorial clues to fungal meningitis in MRI delivered a sounder course of treatment. This case underlines the imagery features and its clinical conduciveness in confronting cases of fungal meningitis.
References
1. Gavito-Higuera J, Mullins CB, Ramos-Duran L, Olivas Chacon CI, Hakim N, Palacios E. Fungal infections of the central nervous system: a pictorial review. J Clin Imaging Sci 2016;6:24
Google Scholar
2. Mohan S, Jain KK, Arabi M, Shah GV. Imaging of meningitis and ventriculitis. Neuroimaging Clin N Am 2012;22:557-583
Crossref
Google Scholar
3. Mathur M, Johnson CE, Sze G. Fungal infections of the central nervous system. Neuroimaging Clin N Am 2012;22:609-632
Crossref
4. Perfect JR, Durack DT. Fungal Meningitis. In: Scheld WM, Whitely RJ, Durack DT. Infections of the cen- tral nervous system. 2nd ed. Philadelphia: Lippincott¬Raven Publishers, 1997:721-724
5. Dubbioso R, Pappata S, Quarantelli M, D'Arco F, Manganelli F, Esposito M, et al. Atypical clinical and radiological presentation of cryptococcal choroid plexitis in an immunocompetent woman. J Neurol Sci 2013;334:180-182
Crossref
Google Scholar
6. Nakajima H, Takayama A, Fujiki Y, Ito T, Kitaoka H. Refractory Cryptococcus neofromans meningo- encephalitis in an immunocompetent patient: para- doxical antifungal therapy-induced clinical deterio- ration related to an immune response to cryptococcal organisms. Case Rep Neurol 2015;7:204-208
Google Scholar
7. Sarkis RA, Mays M, Isada C, Ahmed M. MRI findings in cryptococcal meningitis of the non-HIV population. Neurologist 2015;2:40-45
Crossref
Google Scholar
8. Popovich MJ, Arthur RH, Helmer E. CT of intra- cranial cryptococcosis. AJR Am J Roentgenol 1990; 154:603-606
Crossref
Google Scholar
9. Patronas NJ, Makariou EV. MRI of choroidal plexus involvement in intracranial cryptococcosis. J Comput Assist Tomogr 1993;17:547-550
Crossref
Google Scholar
10. Aiken AH. Central nervous system infection. Neuroimaging Clin N Am 2010;20:557-580
Crossref
11. Arnder L, Castillo M, Heinz ER, Scatliff JH, Enterline D. Unusual pattern of enhancement in cryptococcal meningitis: in vivo findings with postmortem correl- ation. J Comput Assist Tomogr 1996;20:1023-1026
Crossref
Google Scholar
