pISSN : 3058-423X eISSN: 3058-4302
Open Access, Peer-reviewed
pISSN : 3058-423X eISSN: 3058-4302
Open Access, Peer-reviewed
Yong Woo Choi,Hyungrok Kim,Hyunjung Kwon,Moon Hyung You,Jong Soo Choi,Hyun Chung,Joonsoo Park
http://dx.doi.org/10.17966/KJMM.2017.22.4.167 Epub 2017 December 22
Abstract
Keywords
Balanitis Candida balanitis Herpes genitalis Infectious balanitis
INTRODUCTION
Balanitis is defined as inflammation of the glans penis, which often involves the prepuce[1]. Sarah et al reported that it is a common condition affecting 11% of male genitourinary clinic participants[1]. There is a wide variety of causes and predisposing factors[2],[3]. Balanitis is more common among uncircumcised men possibly as a result of poorer hygiene and aeration or irritation[1],[2]. Underlying conditions can also predispose to balanitis, which may be more severe form[2]. It has been reported as candida balanitis may be especially severe in patients with diabetes mellitus[2]. In a series of 321 patients with balanitis, 185 were infectious and the majority was irritable or due to mechanical causes[1],[9]. The cause of balanitis varies, but the symptoms are similar and difficult to differentiate[3],[4]. Herein, we present a case of a 46-year-old patient with candida balanitis, who was first misdiagnosed as herpes simplex infection, with review of literatures.
CASE
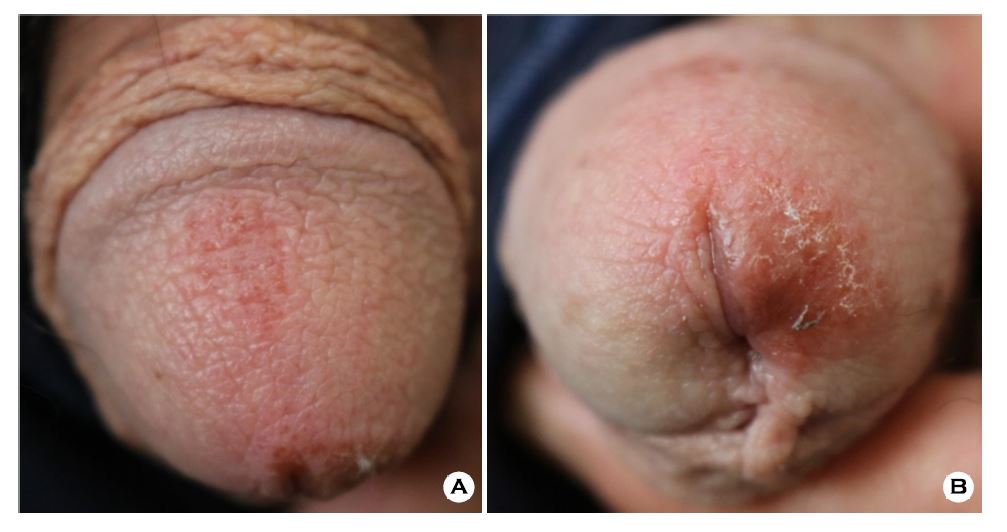
The patient is a 46-year-old male, who had visited dermatologic clinic with complaint of pruritic erythematous macules, vesicles and erosion for a month. Previous treatment included systemic and topical acyclovir and topical mupirocin ointment for 2 weeks under the impression of herpes genitalis, but the symptom had not improved.
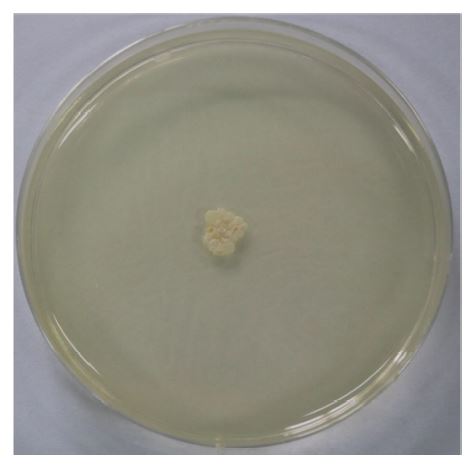
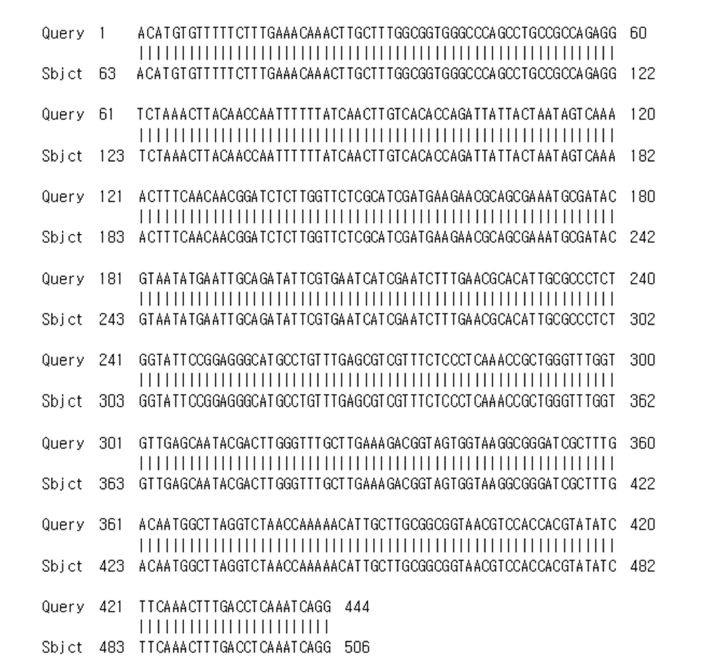
Erythematous macules and grouped vesicles on the glans penis and upper side of prepuce area were noticed. In addition, scales were noticed on the tip of glans penis (Fig. 1A, 1B). Lab findings were within normal range. KOH exam was done on the glans penis, and pseudohyphae and spores were observed. Scales from the lesions were cultured for 48 hours at 25℃ on Sabouraud's dextrose agar plate, revealing colonies with white to cream colored, smooth, and glabrous appearance (Fig. 2). Polymerase chain reaction (PCR) study revealed positive result of Candida albicans (Fig. 3).
We confirmed the diagnosis of candida balanitis by Candida albicans, and the patient applied topical isoconazole cream twice a day for 2 weeks. The patient has recovered over time and the skin lesion improved with crusted lesion.
DISCUSSION
Candida balanitis is considered to be the most common cause of balanitis and is due to infection with candida species, usually Candida albicans[3],[6],[16]. It is generally sexually acquired carriage of yeasts on the penis is common, being 14~18% with no significant differences between carriage rate in circumcised or uncircumcised men[1],[10]. Significantly more of the female partners of men carrying yeasts were found to have candida infection[2],[11],[17]. Diagnosis may be on the clinical feature alone, microscopy or culture. Infection may occur without sexual contact, usually in the presence of diabetes of which it may be the presenting symptom, or after the use of oral antibiotics[2],[18]. Symptoms are of burning and itching of the penis with generalized erythema of the glans penis which dry glazed appearance, with eroded white papules and white discharge[2],[5]. In diabetic patients the presentation may be more severe with edema and fissuring of the foreskin, which may become non-retractile[1],[2]. However, this clinical aspect is often nonspecific.
Treatment must be preceded by accurate diagnosis, and clinical features are one of the most important tools of diagnosis. This is especially important in dermatologic disease, where a number of diseases can be diagnosed with characteristic features alone. However, atypical and nonspecific findings may delay diagnosis and mislead the physicians; candida balanitis is one of such examples.
The patient in this case treated for herpes genitalis without any KOH exam, microorganism culture and biopsy for 2 weeks. The 2016 Korean sexually transmitted disease guidelines recommend treatment of herpes genitalis if there are grouped vesicles presented[3]. In guidelines refer to avoid clinical diagnosis if lesions are atypical presentation and make diagnosis with PCR test3. However, general practitioner cannot do enough laboratory tests like in general hospital due to lack of facilities and low opportunity cost. Usually general practitioners diagnose inevitably with clinical presentation only.
Bacteria represent the second most common cause of infectious balanitis[2],[19]. Such as Streptococcus spp., Staphylococcus aureus, Pseudomonas spp., Gardnerella vaginalis, anaerobes, Treponema pallidum, Chlamydia tracomatis, and Mycoplasma spp. have all been reported as causes of balanitis[2],[13]. Less commonly reported causes of balanitis are viral and parasitic[2],[13]. The clinical features of this disease are slightly different from each other[2],[13]. For example, erythematous grouped natured vesicles on glans penis are characteristic features of herpes genitalis. Nevertheless, clinical presentation of infectious balanitis is still nonspecific to confirm the diagnosis.
Our case was the case of candida balanitis, misdiagnosed as herpes genitalis because of signs of erythematous grouped natured vesicles and macules only. These lesions can be seen in other genital disease, so accurate diagnosis by KOH exam, microorganism culture, and/or biopsy is necessary [2],[15],[16]. Through KOH exam, fungal culture and PCR test, our cases revealed as candida balanitis. We report a case of candida balanitis with features masquerading as herpes genitalis, believing it will help future dermatologic practice.
References
1. Sarah Edwards S. Balanitis and balanoposthitis: a review. Genitourin Med 1996;72:155-159
Crossref
Google Scholar
2. Lisboa C, Ferreira A, Resende C, Rodrigues AG. Infectious balanoposthitis: management, clinical and laboratory features. Int J Dermatol 2009;48:121-124
Crossref
Google Scholar
3. Centers for Disease Control & Prevention, Korean Sexual Transmitted Infection Guideline 2016
4. Pandya I, Shinojia M, Vadukul D, Marfatia YS. Approach to balanitis/balanoposthitis: Current guidelines. Indian J Sex Transm Dis 2014;35:155-157
Crossref
Google Scholar
5. Borelli S, Lautenschlager S. Differential diagnosis and management of balanitis, Hautarzt. 2015;66:6-11
6. Suh MK, Ahn KJ, Ro BI. Superficial cutaneous candidiasis. Korean J Med Mycol 1999;4:98-103
Google Scholar
7. Edwards S, Bunker C, Ziller F, Willem van der M. 2013 European guideline for the management of balanoposthitis. Int J STD AIDS 2014;25:615-626
Crossref
Google Scholar
8. Kang H, Kang HY, Kye YC, Koo DW, Kwon OS, Kim GM, et al. Infectious skin disease. In: Ahn HY, Park SD, Kim GM, Park CJ, Kim HW, Kim JP, et al editors. The compilation committee of Korean der- matology association. Textbook of dermatology 6th ed. Seoul: Daehan medbook Inc, 2014:430-437
9. Birley HDL, Walker MM, Luzzi GA, Bell R, Taylor¬Robinson D, Byrne M, et al. Clinical features and management of recurrent balanitis; association with atopy and genital washing. Genitourin Med 1993;69: 400-403
Crossref
Google Scholar
10. Vohra S, Badlani G. Balanitis and balanoposthitis. Urol Clin North Am 1992;19:143-147
Google Scholar
11. Waugh MA, Evans EGV, Nayyar KC, Fong R. Clotrimazole (Canesten) in the treatment of candida balanitis in men. Br J Venereal Dis 1978;54:184-186
Google Scholar
12. Veller Fornasa C, Calabro A, Miglietta A, Tarantello M, Biasinutto C, Peserico A. Mild balanoposthitis. Genitourin Med 1994;70:345-346
Google Scholar
13. Davidson F. Yeast and circumcision in the male. Br J Vener Dis 1977;53:121-122
Crossref
Google Scholar
14. Rodin P, Kolator B. Carriage of yeasts on the penis. Br Med J 1976;1:1123-1124
Crossref
Google Scholar
15. Dockerty WG, Sonnex C. Candidal balano-posthitis: a study of diagnostic methods. Genitourin Med 1995; 71:407-409
Crossref
Google Scholar
16. Waugh MA. Clinical presentation of candida balanitis¬its differential diagnosis and treatment. Chemotherapy 1982;28(suppl 1):56-60
Google Scholar
17. Oates JK. Sexually transmitted skin disease. Br J Sex Med 1976;3:8-10
18. Lisboa C, Santos A, Dias C, Azevedo F, Pina-Vaz C, Rodrigues A. Candida balanitis: risk factors. J Eur Acad Dermatol Venereol 2010;24:820-826
Crossref
Google Scholar
19. Buechner SA. Common skin disorder of the penis. BJU Int 2002;90:498-506
Crossref
Google Scholar
