pISSN : 3058-423X eISSN: 3058-4302
Open Access, Peer-reviewed
pISSN : 3058-423X eISSN: 3058-4302
Open Access, Peer-reviewed
Min Woo Park,Moo Kyu Suh,Gyoung Yim Ha
http://dx.doi.org/10.17966/KJMM.2017.22.4.159 Epub 2017 December 22
Abstract
Background: Tinea incognito is the dermatophytoses of atypical clinical appearance that is induced by topical and systemic steroid treatment or topical calcineurin inhibitor.
Objective: The purpose of this study was to investigate the clinical and etiological aspects of tinea incognito.
Methods: In the 10-year-period 2007-2017, we reviewed fifty-one patients with tinea incognito with regards to the age, gender, duration, and associated diseases. The patients with tinea incognito were further evaluated concerning the clinical manifestations and culture of organisms.
Results: Age of the tinea incognito was most prevalent in the fifties (23.5%). The male-to-female ratio was 1:1.3. The most common type of infection was tinea corporis (52.9%), followed by tinea faciei (35.3%), tinea manus (5.9%), tinea barbae (3.5%), and tinea cruris (2.0%). The clinical features were to some extent diverse, ranging from eczema-like, seborrheic dermatitis-like, psoriasiform, folliculitis-like, rosacea-like, pyoderma-like, and purpura-like, and discoid lupus erythematosus-like. Trichophyton(T.) rubrum was the most common etiological agent (35.3%), followed by T. mentagrophytes (11.8%), Microsporum(M.) canis (7.8%), T. verrucosum (5.9%), T. erinacei, and M. gypseum (2.0%), respectively.
Conclusion: Because of the increase in tinea incognito, there is a need for careful mycological examination in patients with tinea incognito.
Keywords
Dermatophytoses Steroid Tinea incognito
서 론
잠행백선(tinea incognito)은 스테로이드의 부적절한 전신적 또는 국소적 치료를 지속적으로 사용하여 기존의 특징적인 병변의 형태가 소실된 백선증이다[1]. 또한 tacrolimus나 pimecrolimus 같은 비스테로이드성 면역조절 약제의 국소적 치료로 인해 발생할 수도 있다[2]-[7]. 최근 국소 스테로이드나 면역조절 약제의 남용으로 잠행백선의 발생 빈도가 증가하는 경향을 보이고 있으며[8],[9], 본 증에 대한 보고의 증가로[10]-[25], 본 증에 대한 관심이 증가되고 있다.
이에 저자는 2007년 7월부터 2017년 6월까지 최근 10년간 본원 피부과를 내원한 잠행백선 환자 51명을 대상으로 임상적 관찰과 함께 진균배양 검사로 원인균을 동정하여 문헌고찰과 함께 보고한다.
대상 및 방법
1. 대상
2007년 7월부터 2017년 6월까지 10년간 본원에 피부과에 내원한 환자 중 피부 병소에 KOH 검사로 균사가 발견되었거나 KOH 검사상 음성이나 진균배양 검사에서 피부사상균(dermatophyte)이 배양된 잠행백선 환자 51명을 대상으로 하였다.
2. 방법
잠행백선 환자의 병력을 후향적으로 조사하여 연령별, 성별, 유병기간, 동반질환, 임상양상 및 병변부위, 병형 및 원인균주에 대해 조사하였다.
결 과
1. 연령 및 성별분포
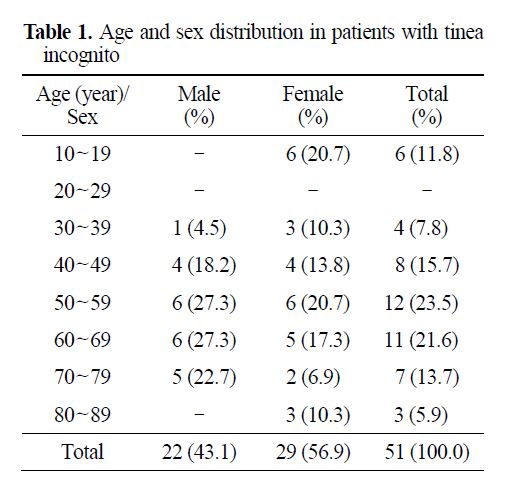
연령별로는 50대가 12명(23.5%)으로 가장 많았고, 60대가 11명(21.6%), 40대가 8명(15.7%), 70대가 7명(13.7%), 10대가 6명(11.8%), 30대가 4명(7.8%), 80대가 3명(5.9%) 순으로 평균 연령은 54.0세였으며 40대에서 70대 사이의 중노년층이 43명(74.5%)으로 많았다. 남녀의 발생 빈도는 남자가 22명, 여자가 29명으로 남녀비는 1:1.3로 여자에서 조금 더 호발하여 기존 연구들과 큰 차이를 보이지 않았다(Table 1).
2. 유병기간
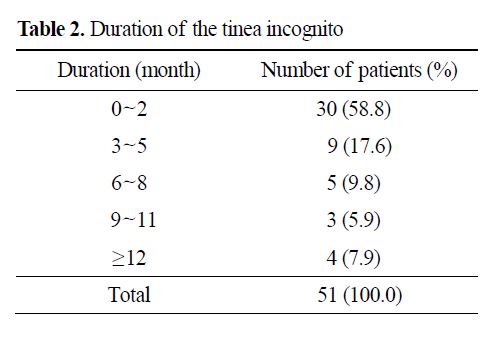
잠행백선의 유병기간은 3개월 미만이 30명(58.8%)으로 가장 많았고, 3개월 이상 6개월 미만이 9명(17.6%), 6개월 이상 9개월 미만이 5명(9.8%), 9개월 이상 12개월 미만이 3명(5.9%) 순이었고 12개월 이상도 4명(7.9%)이 있었다(Table 2).
3. 동반질환
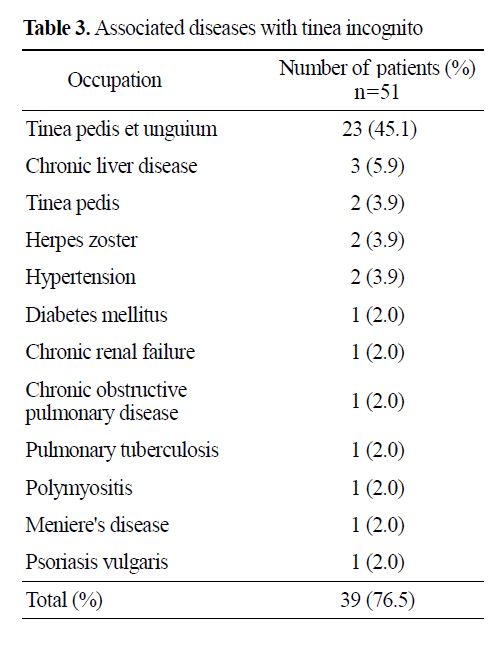
잠행백선 환자 51명 중 39명(76.5%)에서 동반질환이 있었으며, 발백선 및 손발톱진균증이 동반된 경우가 23명(45.1%)으로 가장 많았고, 만성간질환 3명(5.9%), 발백선, 대상포진, 고혈압이 각각 2명(3.9%), 당뇨, 만성신부전, 만성폐쇄성폐질환, 폐결핵, 다발근육염, 메니에르병, 건선이 각각 1명(2.0%) 순이었다(Table 3).
4. 임상양상 및 병변부위
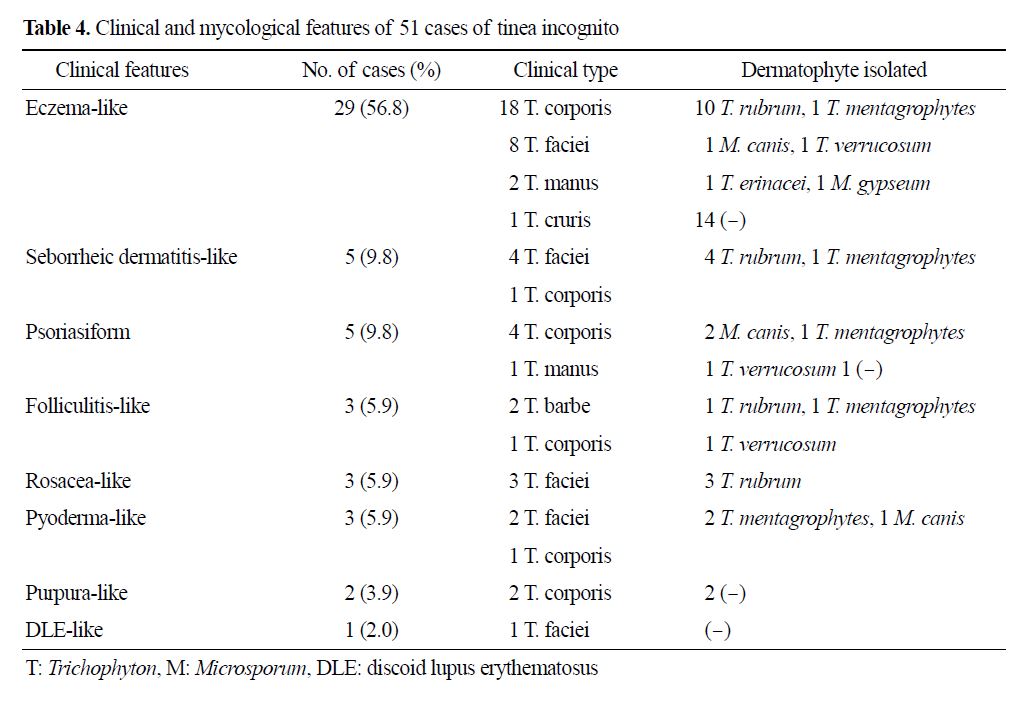
잠행백선의 임상양상으로 습진모양이 29명(56.8%)으로 가장 많았고, 지루피부염모양, 건선모양이 각각 5명(9.8%), 모낭염모양, 주사모양, 피부고름증모양이 각각 3명(5.9%), 자색반모양 2명(3.9%), 원판홍반루푸스모양 1명(2.0%) 순이었다(Table 4, Fig. 1).
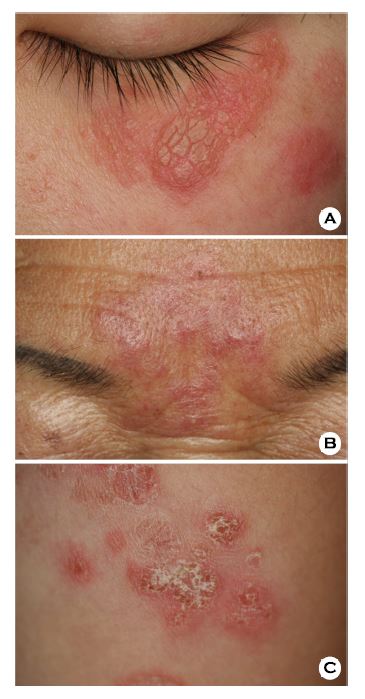
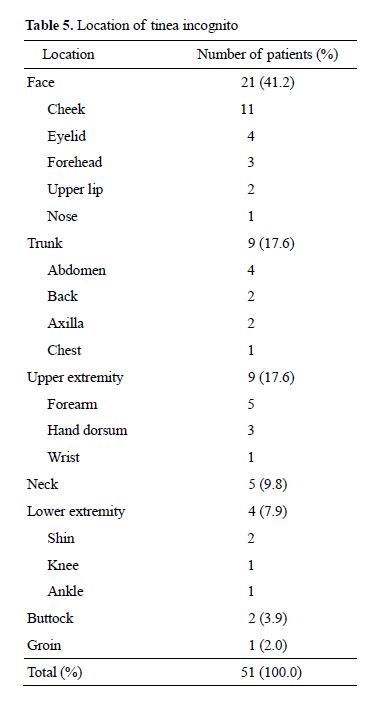
병변부위는 얼굴이 21명(41.2%)으로 가장 많았고, 몸통, 상지가 각각 9명(17.5%), 목 5명(9.8%), 하지 4명(7.9%), 궁둥이 2명(3.9%), 샅고랑부위 1명(2.0%) 순이었다. 얼굴 중에서는 뺨 11명, 눈꺼풀 4명, 이마 3명, 윗입술 2명, 코 1명이었고, 몸통 중에서는 배 4명, 등, 겨드랑이가 각각 2명, 가슴 1명이었고, 상지 중에서는 아래팔 5명, 손등 3명, 손목 1명이었고, 하지 중에서는 정강이 2명, 무릎, 발목이 각각 1명이었다(Table 5).
5. 병형별 분류
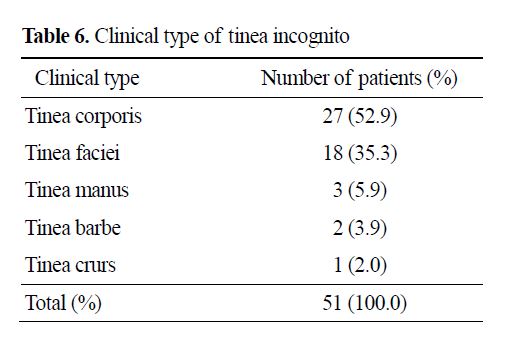
병형별로 보면 몸백선이 27예(52.9%)로 가장 많았고, 얼굴백선 18예(35.3%), 손백선 3예(5.9%), 수염백선 2예(3.9%), 샅백선 1예(2.0%) 순이었다. 습진양 형태는 몸백선이 18예로 가장 많았고, 얼굴백선 8예, 손백선 2예, 샅백선 1예 순이었고, 지루피부염모양은 얼굴백선 4예, 몸백선 1예 순이었고, 건선모양은 몸백선이 4예, 손백선이 1예 순이었고, 모낭염모양은 수염백선 2예, 몸백선 1예 순이었고, 주사모양은 3예 모두 얼굴백선이었고, 피부고름증모양은 얼굴백선이 2예, 몸백선 1예 순이었고, 자색반모양은 2예 모두 몸백선이었고, 원판홍반성푸루스모양은 얼굴백선 1예이었다(Table 4, 6).
6. 원인균주
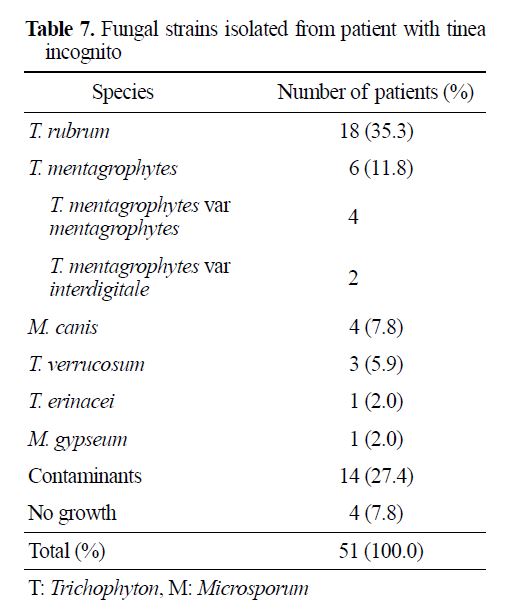
잠행백선 51예 중 47예(92.2%)에서 KOH 검사에서 양성을 보였으며, 4예(7.8%)에서는 KOH 검사에서 음성을 보였으나 진균배양에서 양성소견을 보였다. 또한 51예 중 오염균 14예(27.4%)와 균주가 자라지 않은 경우 4예(7.8%)를 제외한 33예(64.7%)에서 배양 양성소견을 보였다.
피부병변의 진균배양 검사로 분리 동정된 원인균주는 Trichophyton(T.) rubrum이 18주(35.3%)로 가장 많았고, T. mentagrophytes 6주(11.8%), Microsporum(M.) canis 4주(7.8%), T. verrucosum 3주(5.9%), T. erinacei, M. gypseum 각각 1주(2.6%) 순이었으며 T. mentagrophytes 6주 중에서는 동물친화성(zoophilic) 균인 T. mentagrophytes var mentagrophytes가 4주, 사람친화성(anthropophilic) 균인 T. mentagrophytes var interdigitale가 2주이었다(Table 7).
습진모양은 T. rubrum이 10주로 가장 많았고, T. mentagrophytes 1주, M. canis, T. verrucosum, T. erinacei, M. gypseum 각각 1주 순이었고, 지루피부염모양은 T. rubrum이 가장 많았고, T. mentagrophytes 1주 순이었고, 건선모양은 M. canis가 2주로 가장 많았고, T. mentagrophytes, T. verrucosum 각각 1주 순이었고, 모낭염모양은 T. rubrum, T. mentagrophytes, T. verrucosum 각각 1주이었고, 주사모양은 3주 모두 T. rubrum이었고, 피부고름증모양은 T. mentagrophytes가 2주, M. canis 1주 순이었고, 자색반모양 및 원반홍반루푸스모양은 분리 동정된 균주가 없었다(Table 4).
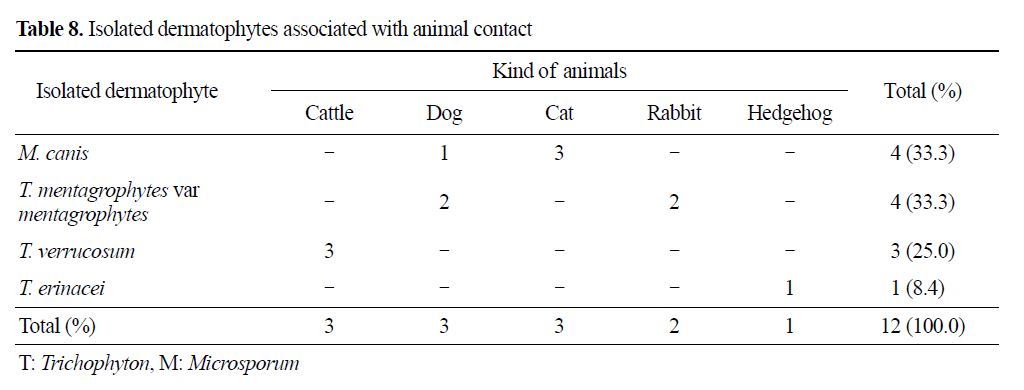
원인균주 중 사람친화성 피부사상균은 T. rubrum 18주, T. mentagrophytes var interdigitale 2주로 총 20주로 가장 많았고, 동물친화성 피부사상균은 M. canis, T. mentagrophytes var mentagrophytes 각각 4주, T. verrucosum 3주, T. erinacei 1주로 총 12주, 흙친화성(geophilic) 피부사상균은 M. gypseum 1주 순이었다. 이 중 동물친화성 피부사상균 12주의 전염원인 접촉 동물은 M. canis 4예(33.3%)는 고양이와 접촉된 경우 3예, 개와 접촉된 경우 1예 순이었고, T. mentagrophytes var mentagrophytes 4예(33.3%)는 개와 접촉한 경우, 토끼와 접촉한 경우 각각 2예이었고, T. verrucosum 3예(25.0%)는 모두 소와 접촉한 경우 이었고, T. erinacei 1예(8.4%)는 고슴도치와 접촉한 경우였다(Table 8).
고 찰
잠행백선은 1968년 Ive와 Marks[1]에 의해 처음으로 명명되었으며, 대부분이 백선증을 다른 피부질환으로 오인하는 경우가 많다[2],[6],[14],[16],[20]-[23]. 백선증의 치료에 스테로이드제제나 비스테로이드성 면역조절 약제를 부적절하게 장기간 사용하는 것은 세포 매개성 면역을 감소시키고 염증반응을 억제하며 비전형적인 백선증인 본 증을 유발하는데, 임상적으로 경계가 불분명한 홍반과 인설 및 염증반응의 소실 등으로 습진모양, 지루피부염모양, 모낭염모양, 주사모양, 자색반모양, 원반홍반성루푸스모양 등의 다양한 형태를 보일 수 있다[23]. 더욱이 최근에는 스테로이드 국소도포제와 달리 장기간의 사용에도 혈관확장이나 피부위축 등의 부작용이 없는 비스테로이드성 면역조절 약제의 국소도포제가 여러 피부질환 치료에 사용하는 경우가 늘어 본 증에 대한 보고의 증가로[10]-[25] 본 증에 대한 관심이 필요할 것으로 생각되어 본 연구를 시작하였다.
연령별 분포는 50대가 가장 많았고, 평균 연령은 54.0세로 2006년 Romano 등[23]이 이탈리아에서 15년간 본 증 환자 200명에 대한 연구의 42세, 2011년 Ansar 등[19]이 이란에서 16년간 본 증 환자 56명에 대한 연구의 32.6세, 2013년 Kim 등[17]이 국내 피부과에서 9년간 본 증 환자 283명에 대한 다기관 연구의 44.6세 보다 높은 연령층에 많았다. 그리고 남녀간의 발생 빈도를 보면 1:1.3으로 여자에 조금 더 호발하였는데 Romano 등[23]의 1:1.1의 보고와 비슷하였으나 Kim 등[17]의 1.3:1, Ansar 등[19]의 1.1:1로 남자에서 조금 더 많다는 보고와는 차이를 보였다. 유병기간은 3개월 미만이 가장 많았는데 Kim 등[17]의 평균 15개월 보다는 유병기간이 짧았다. 동반질환은 발백선 및 손발톱진균증이 동반된 경우가 가장 많았는데 Kim 등[17]도 본 증의 위험인자로 발백선 및 손발톱진균증이 동반된 경우라고 하여 본 증이 있는 환자는 반드시 발백선 및 손발톱진균증이 동반되었는지 확인할 필요가 있을 것으로 생각된다. 임상양상으로 다른 보고자들[17],[19],[23]과 마찬가지로 습진모양이 가장 많았고, 그 외 지루피부염모양, 건성모양, 모낭염모양, 주사모양, 피부고름증모양, 자색반모양, 원판홍반푸루스모양 순이었는데 Kim 등[17]의 백반모양, Romano 등[23]의 경피증모양은 없었다. 병변부위는 얼굴이 가장 많았고, 몸통, 사지, 목, 하지, 궁둥이, 샅고랑부위 순이었는데, Kim 등[17]의 몸통, 얼굴 순이었다는 보고와 비슷하였다. 병형별로 보면 Ansar 등[19]과 마찬가지로 몸백선이 가장 많았고, 그외 얼굴백선, 손백선, 수염백선, 샅백선 순이었다.
원인균주로는 Kim 등[17] 및 Romano 등[23]과 마찬가지로 T. rubrum이 가장 많이 분리 동정되었고, T. mentagrophytes, T. verrucosum, T. erinacei, M. gypseum 순이었는데, Ansar 등[19]은 T. verrucosum이 가장 많이 분리 동정된 원인균주라고 하여 다소 차이를 보였는데 이는 이란이라는 지역적 피부사상균 분포 차이에 기인한 것으로 생각된다.
원인균주 중 동물친화성 피부사상균은 M. canis, T. mentagrophytes var mentagrophytes, T. verrucosum, T. erinacei 순이었는데, 이들의 전염원인 접촉동물은 Lee 등[26]의 보고와 마찬가지로 개, 고양이, 소, 토끼 및 고슴도치 이었는데, 본 증이 있는 경우 반드시 환자 집에 가축이나 애완동물을 키우는지 확인해야 할 것으로 생각된다.
본 논문은 단일기관에서 조사한 결과이므로 결론에 한계점이 있어 향후 더 많은 증례를 가지고 조사해야 할 것으로 생각된다.
결 론
2007년 7월 1일부터 2017년 6월 30일까지 10년간 동국대학교 경주병원에 내원한 환자 중 피부 병소에서 KOH 검사로 균사가 발견되었거나 KOH 검사상 음성이나 진균배양 검사에서 피부사상균이 배양된 잠행백선 환자 51명을 대상으로 임상적 관찰과 함께 원인균을 분리 동정한 결과 다음과 같은 결론을 얻었다.
잠행백선 환자의 연령별로는 50대에서 23.5%로 가장 높았고 40대 이상 중노년층이 74.5%로 대부분을 차지하였다. 남녀의 발생 빈도는 1:1.3으로 여자에서 조금 더 호발하였다. 유병기간은 3개월 미만이 58.8%로 가장 많았고, 동반질환은 발백선 및 손발톱진균증이 동반된 경우가 45.1%로 많았다. 잠행백선의 임상양상으로 습진모양이 56.8%로 가장 많았고, 지루피부염모양, 건선모양이 각각 9.8%, 모낭염모양, 주사모양, 피부고름증모양이 각각 5.9%, 자색반모양 3.9%, 원반홍반루푸스모양 2.0% 순이었다. 병변부위는 얼굴이 41.2%로 가장 많았고, 몸통, 상지가 각각 17.6%, 목이 9.8%, 하지 7.9%, 궁둥이 3.9%, 샅고랑부위 2.0% 순이었다. 병형별로 보면 몸백선이 52.9%로 가장 많았고, 얼굴백선 35.3%, 손백선 5.9%, 수염백선 3.9%, 샅백선 2.0% 순이었다. 잠행백선의 원인균주는 T. rubrum이 35.3%로 가장 많았고, T. mentagrophytes 11.8%, M. canis 7.8%, T. verrucosum 5.9%, T. erinacei, M. gypseum 각각 2.0% 순이었다.
References
1. Ive FA, Marks R. Tinea incognito. Br Med J 1968; 3:149-152
Crossref
Google Scholar
2. Aremas R, Moreno-Coutino G, Vera L, Welsh O. Tinea incognito. Clin Dermatol 2010;28:137-139
Google Scholar
3. Choi YL, Kim JA, Rho NK, Lee DY, Lee JH, Yang JM, et al. A case of tinea incognito induced by 1% pimecrolimus (Elidel®) cream. Korean J Dermatol 2006;44:731-733
Google Scholar
4. Crawford KM, Bostrom P, Russ B, Boyd J. Pimecrolimus-induced tinea incognito. Skinmed 2004; 3:352-353
Crossref
Google Scholar
5. Siddaiah N, Erickson Q, Miller G, Elston DM. Tacrolimus-induced tinea incognito. Cutis 2004;73: 237-238
Google Scholar
6. Hwang SM, Kim DM, Suh MK, Ha GY, Kim JR. Eczema-like tinea incognito occurring leg. Korean J Med Mycol 2011;16:51-55
Google Scholar
7. Rallis E, Koumantaki-Mathioudaki E. Pimecrolimus induced tinea incognito masquerading as intertriginous psoriasis. Mycoses 2007;51:71-73
Crossref
Google Scholar
8. Ann HH, Park SD, Kim KM, Park CJ, Kim HW, Kim JP, et al. Dermatophytosis. In: Korean dermato- logical association, editors. Textbook of dermatology, 6th ed. Seoul: Korean medical books, 2014:422-423
9. del Boz J, Crespo V, Rivas-Ruiz F, de Troya M. Tinea incognito in children: 54 cases. Mycoses 2011;54: 254-258
Crossref
Google Scholar
10. Verma SB, Vasani R. Male genital dermatophytosis¬clinical features and the effects of misuse of topical steroids and steroid combinations - an alarming pro- blem in India. Mycoses 2016;509:606-614
11. Liu ZH, Shen H. Tinea incognito in an old patient with bullous pemphigoid receiving topical high potency steroids. J Mycol Med 2015;25:245-246
Google Scholar
12. Kye H, Kim DH, Seo SH, Ahn HH, Kye KC, Choi JE. Polycystic annular lesion masquerading as lupus erythematosus and emerging as tinea faciei incognito. Ann Dermatol 2015;27:322-325
Google Scholar
13. Park YW, Choi JW, Paik SH, Kim DY, Jin SP, Park HS, et al. Tinea incognito simulating herpes simplex virus infection. Ann Dermatol 2014;26:267-269
Crossref
Google Scholar
14. Tan Y, Lin L, Feng P, Lai W. Dermatophytosis caused by Trichophyton rubrum mimicking syphilid: a case report and review of literature. Mycoses 2014;57: 312-315
Google Scholar
15. Lee MH, Yoo JY, Song YB, Suh MK, Ha GY, Kim JR, et al. Periocular tinea caused by Trichophyton rubrum. Korean J Dermatol 2013;51:997-998
Google Scholar
16. Zisova LG, Dobrev HP, Tchernev G, Semkova K, Aliman AA, Chorleva KI, et al. Tinea atypia: report of nine cases. Wien Med Wochenschr 2013;163:549 -555
17. Kim WJ, Kim TW, Mun JH, Song M, Kim HS, Ko HC, et al. Tinea incognito in Korea and its risk factors: nine-year multicenter survery. J Korean Med Sci 2013; 28:145-151
Crossref
Google Scholar
18. Atzori L, Pau M, Aste N, Aste N. Dermatophyte infections mimicking other skin diseases: a 154-person case survey of tinea atypia in the distinct of Cagliari (Italy). Int J Dermatol 2012;51:410-415
Google Scholar
19. Ansar A, Farshchian M, Nazeri H, Ghiasian SA. Clinico-epidemiological and mycological aspects of tinea incognito in Iran: a 16-year study. Med Mycol J 2011;52:25-32
Crossref
Google Scholar
20. Kang GS, Hwang SM, Suh MK, Ha GY, Jang TJ. A case of rosacea-like tinea faciei caused by Tricho- phyton rubrum. Korean J Med Mycol 2010;15:22-26
Google Scholar
21. Aste N, Pau M, Aste N, Atzori L. Tinea corporis mimicking herpe zoster. Mycoses 2010;54:463-465
Crossref
Google Scholar
22. Serarslan G. Pustular psoriasis-like tinea incognito due to Trichophyton rubrum. Mycoses 2007;50:523-524
Crossref
Google Scholar
23. Romano C, Maritati E, Gianni C. Tinea incognito in Italy: a 15-year survey. Mycoses 2006;49:383-387
Crossref
Google Scholar
24. Sanchez-Castellanos M, Mayorga-Rodriguez JA, Sandoval-Tress C, Hernandez-Torres M. Tinea incog- nito due to Trichophyton mentagrophytes. Mycoses 2006;50:85-87
Crossref
Google Scholar
25. Gorani A, Schiera A, Oriani A. Case report. rosacea¬like tinea incognito. Mycoses 2002;45:135-137
Crossref
Google Scholar
26. Lee YW, Lim SH, Yim SM, Choe YB, Ahn KJ. A clinical and mycological study of dermatophytosis associated with animal contact. Korean J Med Mycol 2005;10:151-159
Google Scholar
