pISSN : 3058-423X eISSN: 3058-4302
Open Access, Peer-reviewed
pISSN : 3058-423X eISSN: 3058-4302
Open Access, Peer-reviewed

Tae Heum Park,Woo Il Kim,Moon Kyun Cho,Kyu Uang Whang,Sooyoung Kim
10.17966/JMI.2020.25.1.17 Epub 2020 April 07
Abstract
Tinea capitis is more common in children than in adults. Due to the low incidence of this condition among adults, it is frequently misdiagnosed as other scalp diseases, such as seborrheic dermatitis, psoriasis, and cellulitis. Herein, we describe an 82-year-old woman who presented with erythematous scaly patches and alopecia. Mycological examinations revealed tinea capitis caused by Microsporum canis. The patient was then successfully treated with antifungal medications.
Keywords
Fungal infection Microsporum canis Tinea capitis
Tinea capitis is a superficial fungal infection of the scalp that is characterized by scaly patches and alopecia. Moreover, this condition is more common in children than in adults1. Due to its low incidence, it can be misdiagnosed as other scalp diseases, such as seborrheic dermatitis, psoriasis, and chronic cutaneous lupus2. Delayed treatment can result in permanent scarring alopecia. Thus, special attention must be paid to prevent misdiagnosis and inappropriate treatment.
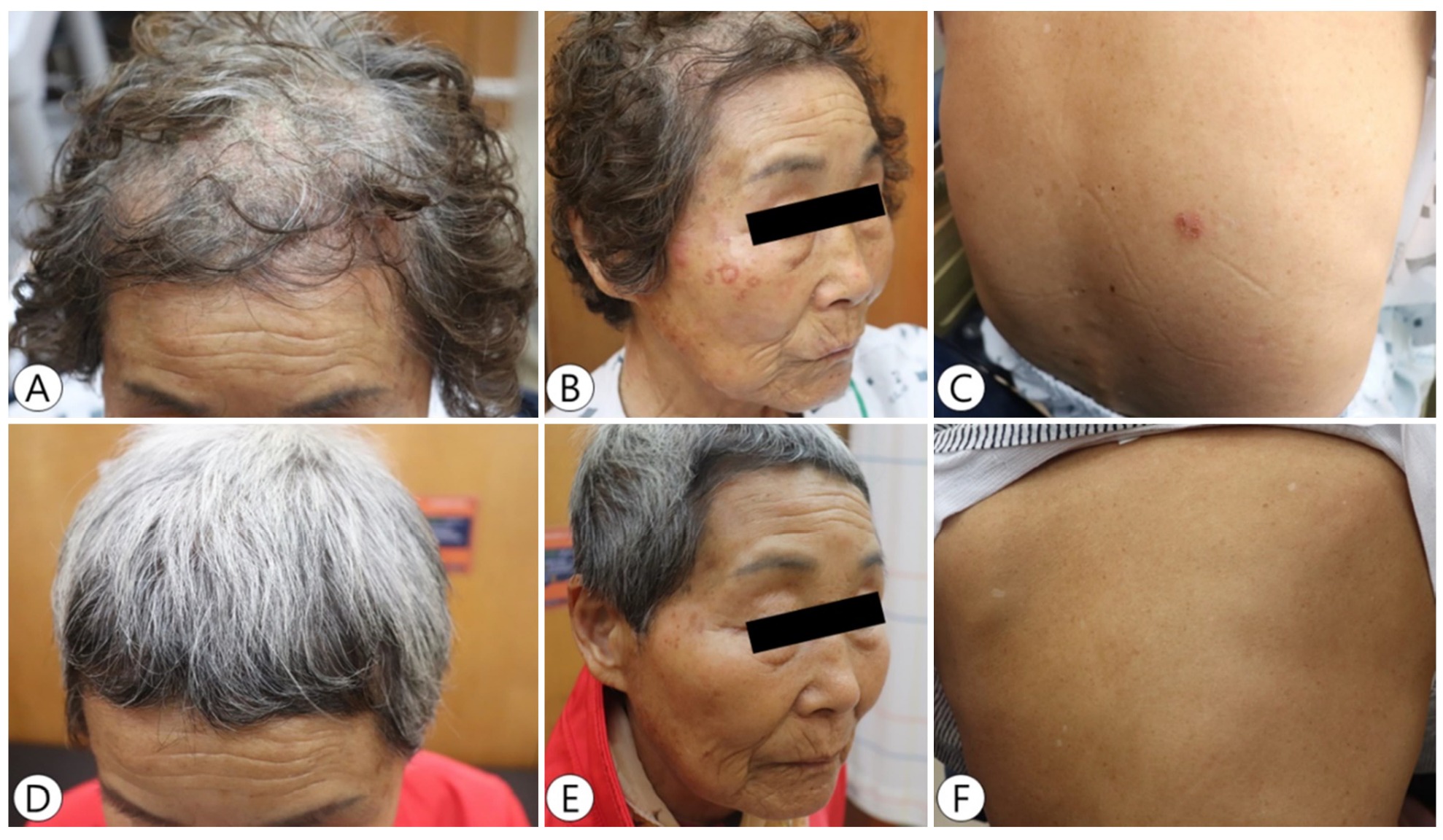
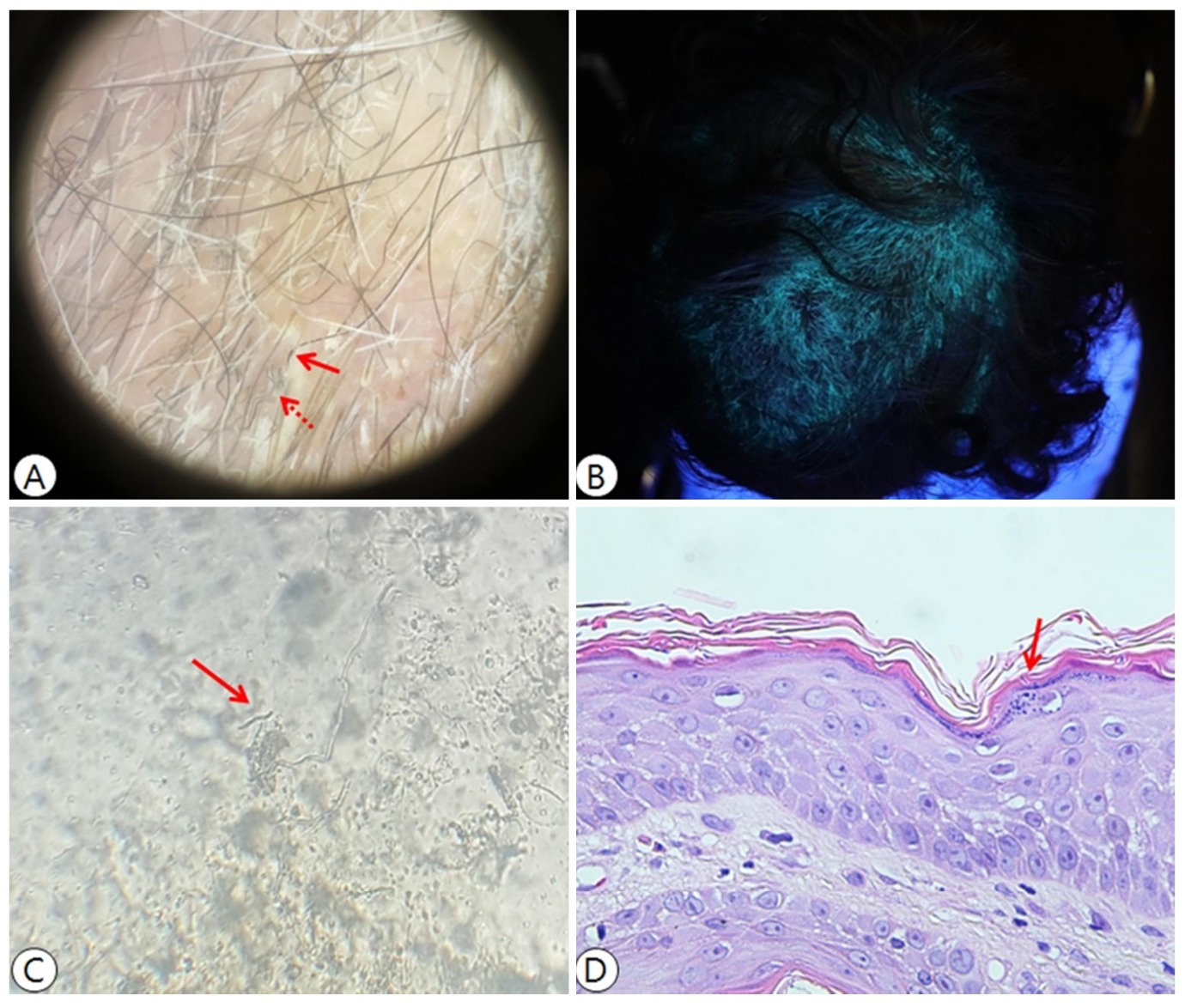
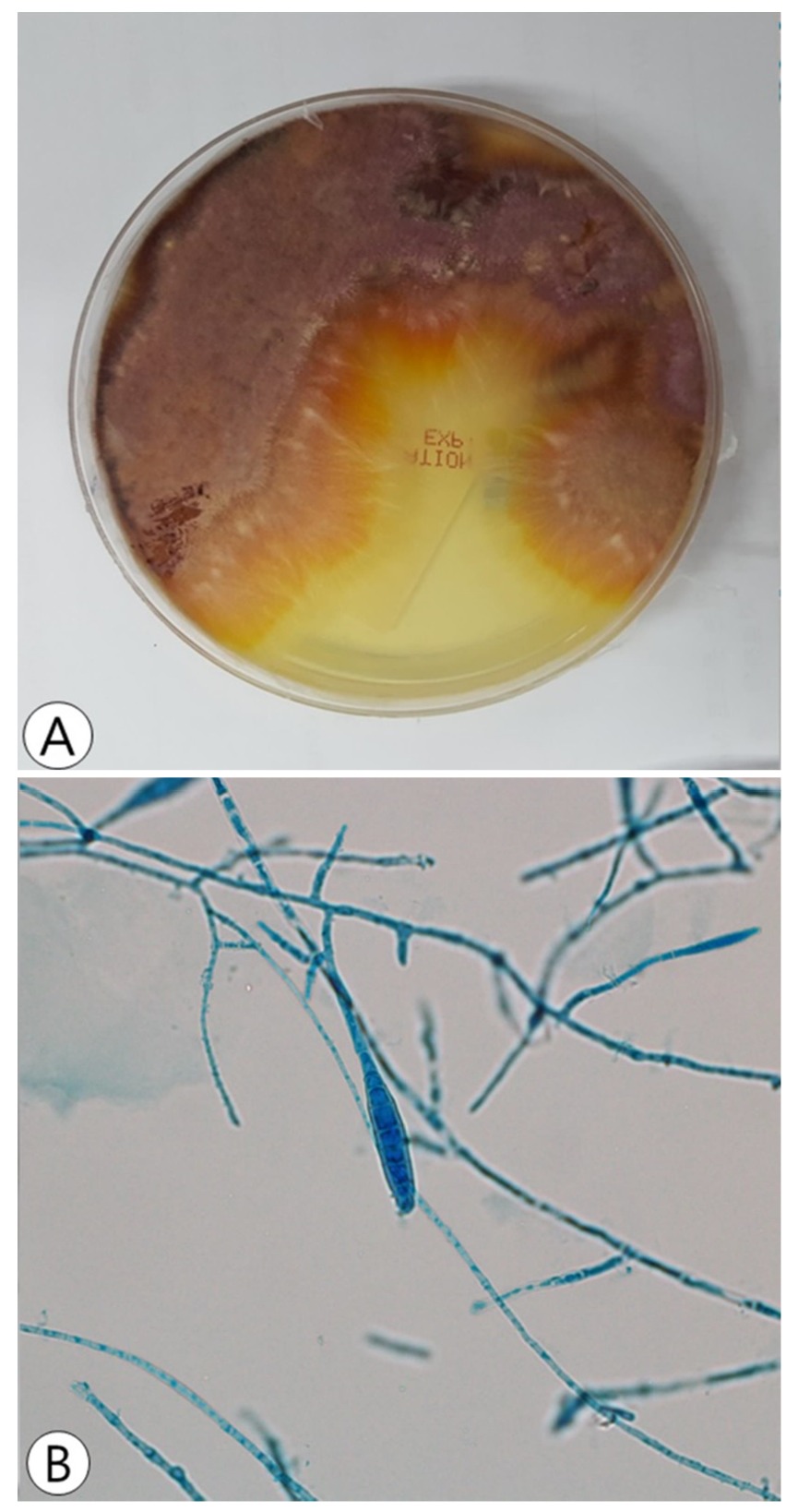
An 82-year-old woman presented with a 6-week history of painful inflammatory erythematous scaly patches and diffuse alopecia. Based on the physical examination, most areas of the frontal scalp were affected, and the patient also had 1x1-cm erythematous scaly patches with pruritus on the right cheek, right forearm, and back (Figure 1A-C). However, no lesions were observed on the palms, soles, and nails. The patient farmed in the countryside and did not have any pets. However, she sometimes cleaned up the stools of neighborhood dogs or stray cats that roam around her house. The laboratory examination findings were as follows: C-reactive protein level, 1.19 mg/dL; fasting serum glucose level, 283 mg /dL; and urine glucose, 1+. Moreover, her kidney and liver functions were normal based on blood chemistry test. She had been taking medication for angina pectoris and was newly diagnosed with diabetes mellitus based on the following examination results: postprandial 2-hour blood glucose of 282 mg/dL and hemoglobin A1c level of 6.3 mg/dL. Based on dermoscopic examination, there were comma-shaped and zigzag hairs on the alopecic area (Figure 2A). According to the Wood's lamp examination, the scalp had yellow-to-green fluorescence (Figure 2B). After strands of hair and scales were collected from the fluorescent lesions, microscopic examination with 20% potassium hydroxide (KOH) preparation was performed, and results showed fungal hyphae on the outside of the hair (Figure 2C). In addition, the strands of hair and scales were inoculated in Sabouraud dextrose agar and were incubated at room temperature. After 3 weeks, red and cottony fungal colonies grew, which were indicative of Trichophyton (T.) rubrum (Figure 3A). The microscopic observation of lactophenol cotton blue stain in the colonies revealed a few macroconidia that had fusiform structures containing 5~15 cells, which indicates Microsporum (Figure 3B). Then, a punch biopsy was performed on the alopecic scalp, which revealed intracorneal fungal hyphae and spores, consistent with tinea capitis (Figure 2D). To identify the definite causative organism, polymerase chain reaction and direct sequencing were performed on the cultured fungal colonies, and the fungus was identified as M. canis. Based on these results, we made a diagnosis of tinea capitis caused by M. canis. The patient was treated with oral terbinafine, topical amorolfine, and topical steroid shampoo with a low-dose systemic steroid for 3 weeks. After 3 months, the subsequent KOH examination result was negative, and symptoms, such as pruritus, erythematous scaly patches, and hair loss, were not observed (Figure 1D-F). Moreover, the patient did not present with complications, including scarring alopecia.
Tinea capitis is commonly observed in children, and it is rarely observed in adults1. This phenomenon is attributed to the relatively immature immune system and low production of sebum in children. Tinea capitis rarely occurs in adults due to the active secretion of fatty acid in the sebum, which has antifungal properties, and the fully mature immune system after puberty3. However, when the immune system is compromised, adults can easily develop tinea capitis. In our case, the patient was newly diagnosed with diabetes mellitus, which is the common cause of immunosuppression. In particular, postmenopausal women whose secretion of sebum decreases due to hormonal changes are at risk4.
In severe cases, the clinical symptoms of tinea capitis include brittle hair, papules, pustules, nodules, and kerion celci, which can leave permanent scarring from alopecia if treatment is delayed. Dermoscopy or trichoscopy can be an effective tool for the diagnosis of tinea capitis and the presence of comma, corkscrew, zigzag, and Morse code-like hair or whitish sheath is indicative of tinea capitis5
When a fungal infection is suspected, the fungal species must be confirmed. The patient's hairs were pulled out and cultured using Sabouraud dextrose agar, and results revealed red and white cottony colonies with maroon-colored reverse pigment. Based on this culture finding, the patient was initially misdiagnosed with T. rubrum infection. Therefore, a multimodal examination was required to identify the causative fungal species. M. canis and T. tonsurans are the most common pathogens of tinea capitis. In particular, in the case of tinea capitis, KOH examination, fungus culture, Wood's lamp examination, and clinical correlation analysis can be effective in determining the causative fungus. On Wood's lamp examination, M. canis, M. audounii, and M. distorum have yellow-green flourescence6. A KOH examination can confirm whether it is an ectothrix or endothrix infection, which can help in determining the causative organism7. If an ectothrix infection is identified via KOH examination, as in this case, the causative organisms can be M. canis, M. audouinii, M. distortum, M. fulvum, M. gypseum, T. megninii, and T. rubrum. The analysis of clinical correlation is also important. Clinically, zoophilic fungi-like M. canis can frequently cause excessive inflammatory reactions, as observed in this case4, which often require higher doses and longer courses of antifungal therapy and early steroid treatment to prevent scarring alopecia8. Taken together, the Wood's lamp examination, KOH examination, and clinical examination findings indicated that this infection was more consistent with M. canis than T. rubrum. Therefore, we initiated empirical antifungal treatment based on a putative Microsporum infection. To accurately identify the causative fungus, we repeatedly subcultured and observed the organism microscopically, which revealed characteristic spindle-shaped macroconidia containing 5~15 cells. Furthermore, we decided to perform molecular tests, which are extremely effective in identifying the species of the pathogen9,10. We performed polymerase chain reaction and direct sequencing on the cultured fungal colonies. First, the nucleotide sequence of the internal transcribed spacer of rRNA gene was obtained. Then, the nucleotide sequence was analyzed using BLAST, and the species was identified as M. canis.
M. canis is one of the primary causes of tinea capitis worldwide11. The number of infections caused by M. canis, which was first reported in Korea in 195712, increased rapidly until 198613. However, the trend in M. canis infections has decreased as people learn about proper hygiene13. M. canis infection occurs mainly after close contact with animals, such as dogs and cats14. In our case, the patient did not raise pets. However, she claimed that dogs and cats often roam around her house and she cleaned up the waste of these animals with her bare hands. Thus, animal waste was considered the possible transmission route.
In adults, tinea capitis with alopecia should be considered with differential diagnoses of other scalp diseases, such as chronic cutaneous lupus erythematosus, lichen planopilaris, and folliculitis decalvans, which require skin biopsies. Because delayed treatment of tinea capitis can leave permanent alopecia, suspicion, detailed history taking, and fungal tests, as observed in this case, are extremely important. Thus, tinea capitis should be considered in adults who present with hair loss and other scalp diseases, and molecular diagnostic testing is effective in identifying fungal infections.
The patient provided written informed consent for the publication and the use of his or her images.
References
1. Elewski BE. Tinea capitis: a current perspective. J Am Acad Dermatol 2000;42:1-20;quiz 21-24
Google Scholar
2. Pandya AG. Seborrheic dermatitis or tinea capitis: don't be fooled. Int J Dermatol 1998;37:827-828
Google Scholar
3. Wagner DK, Sohnle PG. Cutaneous defenses against der- matophytes and yeasts. Clin Microbiol Rev 1995;8:317-335
Google Scholar
4. Gupta AK, Summerbell RC. Tinea capitis. Med Mycol 2000;38:255-287
Google Scholar
5. Dhaille F, Dillies AS, Dessirier F, Reygagne P, Diouf M, Baltazard T, et al. A single typical trichoscopic feature is predictive of tinea capitis: a prospective multicentre study. Br J Dermatol 2019;181:1046-1051
Google Scholar
6. Nenoff P, Krüger C, Schaller J, Ginter-Hanselmayer G, Schulte-Beerbühl R, Tietz HJ. Mycology - an update part 2: dermatomycoses: clinical picture and diagnostics. J Dtsch Dermatol Ges 2014;12:749-777
7. Hay RJ. Tinea capitis: current status. Mycopathologia 2017;182:87-93
Google Scholar
8. Cheng N, Wright DR, Cohen BA. Dermatophytid in tinea capitis: rarely reported common phenomenon with clinical implications. Pediatrics 2011;128:e453-457
Google Scholar
9. Petti CA, Brandt ME, Church DL, Emler S, Simmon K, Zelazny AM. Interpretive criteria for identification of bacteria and fungi by DNA target sequencing; Approved guideline 2nd Edition. Clinical and Laboratory Standards Institute 2018:107-116
Google Scholar
10. Park Y, Shin HB, Kim CK, Roh KH, Yum JH, Yong D, et al. Identification of bacterial and fungal isolates by sequence analysis of 16S rRNA and internal transcribed spacer. Korean J Clin Microbiol 2010;13:34-39
Google Scholar
11. Aly R, Hay RJ, del Palacio A, Galimberti R. Epidemiology of tinea capitis. Med Mycol 2000;38 Suppl 1:183-188
Google Scholar
12. Suh SB. A study of dermatophytes in Korea. J Daegu Med 1959;2:1-33.
13. Lee WJ, Song CH, Lee SJ, Kim DW, Jun JB, Bang YJ. Decreasing prevalence of Microsporum canis infection in Korea: through analysis of 944 cases (1993-2009) and review of our previous data (1975-1992). Mycopathologia 2012;173:235-239
Google Scholar
14. Aly R. Ecology and epidemiology of dermatophyte infections. J Am Acad Dermatol 1994;31:S21-25
Congratulatory MessageClick here!
