pISSN : 3058-423X eISSN: 3058-4302
Open Access, Peer-reviewed
pISSN : 3058-423X eISSN: 3058-4302
Open Access, Peer-reviewed
Osung Kwon,Hyun Chung,Joonsoo Park
http://dx.doi.org/10.17966/KJMM.2017.22.4.149 Epub 2017 December 22
Abstract
Background: Tinea capitis has been recognized as the most commonly misdiagnosed scalp disease. Inappropriate medication and delayed intervention leads to a broad array of complications from prolongation of treatment to scarring of the scalp. The financial deficits and problems imparted on patients continue to be a clinical and social burden.
Objective: The clinical and financial aspects between the initially misdiagnosed group and the properly diagnosed group were analyzed, to provide the epidemiologic basis and to address improvements for misdiagnoses of tinea capitis.
Methods: A retrospective review of electronic and written chart was performed on all patients diagnosed of tinea capitis at Daegu Catholic University Medical Center (DCUMC) from January 2006 to June 2016. A total of 100 patients were included in the study and an initially misdiagnosed group and initially diagnosed group were evaluated.
Results: Significant differences between the groups were not observed in variables including age, sex and occupation. The highest diagnostic precision was observed in dermatologists (78.4%) by using standard microscopic (31.0%) and culture studies (13.0%). Misdiagnosis rate was highest in pediatrics (34.9%) and erroneous examination such as laboratory test (48.4%) and Gram stain (19.4%) were countered in the misdiagnosed group. Additional clinic visits, prescriptions and extra trips to clinics resulted financial disadvantage in the misdiagnosed group.
Conclusion: The misdiagnosed tinea capitis was found to arise from unawareness of the disease that leads to inappropriate approach and medication prescription. The duration, complications and financial loss were reported to be higher in misdiagnosed group based on the study.
Keywords
Comparative analysis Misdiagnosis Scalp disease Tinea capitis
INTRODUCTION
Tinea capitis (TC) is defined as superficial fungal infection of the scalp and still presents with a high incidence, which poses a public health concern around the world[1]. Effective control was brought in industrialized countries after introduction of griseofulvin while other third world regions still remain endemic[2]. Initial stages of the infection is usually asymptomatic, however it can easily spread and present in various clinical forms. Ranging from asymptomatic carrier state to inflammatory favus, the differential diagnoses encompass seborrheic dermatitis, atopic dermatitis, psoriasis vulgaris, alopecia areata, furunculosis, and trichotillomania[3]. Especially, an inflammatory type otherwise known as kerion usually establishes a pustular mass[4]. A combination of lymph node enlargement and fever may lead to the presumption of bacterial infections and treatment with antibiotics is likely administered[5]. Moreover TC has been recognized as the most commonly misdiagnosed scalp diseases referred to a tertiary hospital and concurrent diagnostic challenge result in irreversible complications and prolong unnecessary hospitalization[6]. In Korea, the majority of patients with TC are less than 15 years of age and patients seek medical treatment from clinicians often unwary of dermatophytosis[7]. Predictive symptoms and signs in diagnosing TC should be done by adequate modalities such as potassium hydroxide mount with culture for accurate diagnosis in order to limit financial and clinical burden of the disease. In the present study, the clinical aspects between the initially misdiagnosed group and the properly diagnosed group were analyzed, to provide the epidemiologic basis and to address improvements for further limiting diagnostic difficulties.
MATERIALS AND METHODS
1. Data collection
A retrospective review of electronic and written chart was performed on all patients diagnosed of TC at Daegu Catholic University Medical Center (DCUMC) from January 2006 to June 2016. The following data retrieved from the medical record include admission note, progress note, diagnostic measures and treatment options before and during visits at DCUMC, laboratory results along with basic vital signs. The result of following test methods evaluated in the studies include potassium hydroxide preparation, fungal culture, Grams swab stain, blood culture, trichogram, woods lamp examination, and skin biopsy. Subjects with indefinite history of their primary diagnoses were excluded in the study. A total of 100 patients were gathered under the stated inclusion criteria. The patients were divided into two groups upon whether TC was primarily misdiagnosed or primarily diagnosed and subsequent clinical manifestation, diagnostic measures, complications and treatment duration were analyzed between the two groups.
2. Statistical analysis
All data was gathered and was encoded in numerical values. Frequency and inclination were evaluated with descriptive and multiple response analyses. The variables in continual forms were evaluated with two-sample t-test. The descriptive data are expressed in percentage and mean ± standard deviation. All analysis was performed using SPSS 19.0 version (SPSS, INC®., Chicago, USA) with a p-value of less than 0.05 as statistically significant value.
RESULTS
1. Demographic study
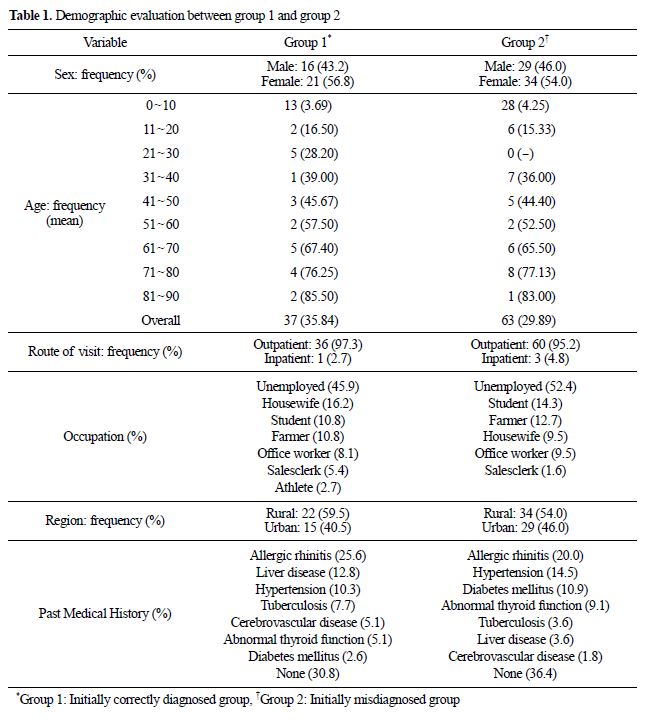
The selected subject groups compliant with the inclusion criteria were a total of 100 patients and 37 were diagnosed of TC on their first visits while remaining 63 were misdiagnosed as other disease entity. The correctly diagnosed group was referred as group 1 and the misdiagnosed group was referred as group 2. For the demographic study, sex, age, route of medical visit, region, occupation and past medical history were evaluated. Regarding the sex, both groups 1 and group 2 displayed similar compositions where female was more dominant. The age ranged from 0 to 89 years with the mean age of 35.84 in group 1, and similarly the age ranged from 0 to 83 years with the mean age of 29.89 in group 2. Outpatient visits were more dominant in both groups and regional variance also showed similar results with slight dominance in urban areas. As for the occupation, unemployed patients were dominant in both groups followed by housewife, farmer, student, office staff, sales clerk, athlete in group 1 and student, housewife, farmer, office staff, sales clerk in group 2 (Table 1).
2. Comparative frequency analysis
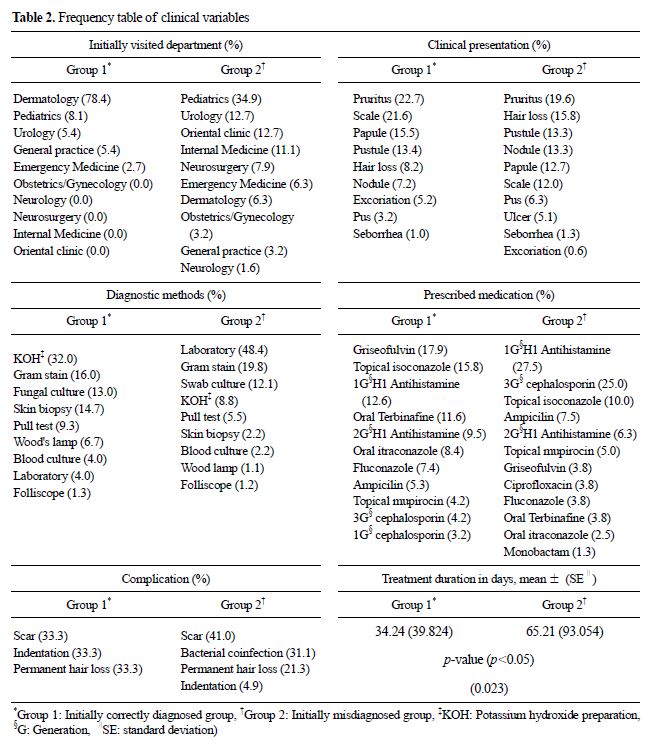
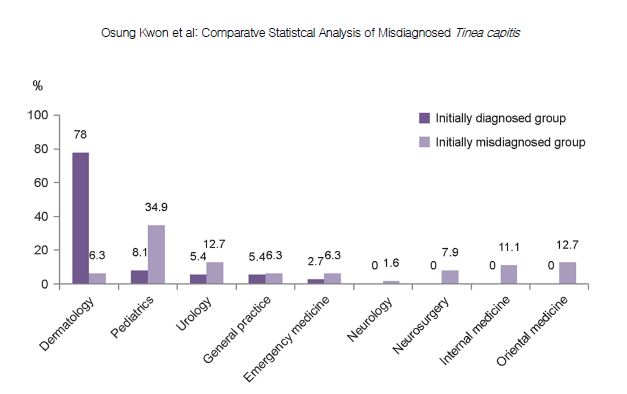
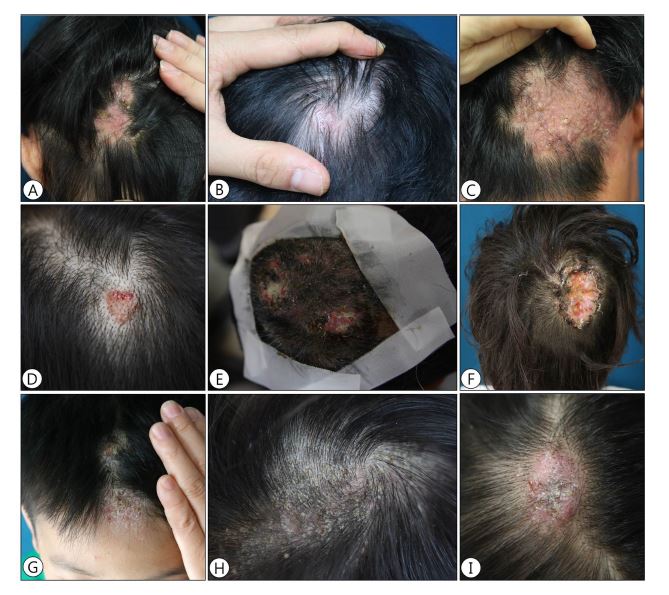
Comparative frequencies of the following variables were measured: initial visited consultant type, symptoms, diagnostic methods, complications, treatment choices. Additionally, duration of treatment was also evaluated between two groups by using two sample t-test. Primarily correct diagnoses were mostly achieved by dermatologist, followed by pediatrician, internists, general practitioners, and lastly emergency medical doctor. Misdiagnosis was most prevalent in pediatricians, followed by dermatologists, urologists, internists, general practitioners and lastly by emergency medical doctors (Fig. 1). Presented symptoms between two groups showed similar results as pruritus was the most common symptom presented by patients in both groups followed by scales, pustules, papules, nodules, hair loss and excoriations. Varying degree of cutaneous lesions including alopecia dominant presentation, pustular inflammatory ulcerative presentation and seborrheic scaly presentation ranged among different patients (Fig. 2A-I). However, in group 1, seborrhea and other symptoms including gastrointestinal trouble were also noticed while ulcer was more presented in group 2. Complication was also more noticeable in group 2. Among 67 patients 61 cases of complication was reported and scar was the most common form. Treatment choices were significantly different between group 1 and group 2. In group 1, initial treatment modalities were based on targeting antifungal effects. The highest prescribed medication was griseofulvin, followed by topical isoconazole, oral terbinafine and oral itraconzole. Antibiotics was more prevalently prescribed in group 2 as the major prescribed drug was third generation cephalosporin with counting up to 25% of all prescription followed by first gene- ration cephalosporin, topical mupirocin, and topical isoconazole. First generation H1 antihistamine was both counting up to 12.6% and 27.5% prescribed respectively in groups 1 and 2. In consideration of various factors, the duration of the illness was measured between the two groups. The mean days of contraction for group 1 was, on average, 34 days compared to 65 days in group (Table 2).
3. Compensatory analysis of misdiagnosed group
The frequency regarding misdiagnosed group was separately measured to calculate the days, visited specialties, diagnostic methods and estimated financial deficits required to a correct diagnosis. The average time for misdiagnosed group to achieve a correct diagnosis was 64 days. Dermatologist was the most commonly visited specialist to sign out proper diagnosis followed by general practitioners, pediatricians, and urologists. For the diagnosis, hair plucking tests was most commonly performed followed by potassium hydroxide preparation, skin biopsy, and Gram swab culture. The estimated financial loss included the extra visits to local medical clinics, tertiary based hospitals, additional fee for medication, and management for complication. In the present study, the misdiagnosed group was visited on average of 3.4 local clinics and 1.7 tertiary based hospitals before coming to DCUMC for the correct diagnosis. On average of 2.5 prescriptions were given to these patients and each patient had made 7.2 trips on average before achieving the right diagnoses.
DISCUSSION
TC is the most common form of scalp disease misdiagnosed by clinicians and a highly inflammatory type may confound medical practitioners unfamiliar with the disease[1],[2],[3],[4],[5],[6]. Treatment with antibiotics frequently occurs and may account for unnecessary costs and morbidity[8]. TC presents in a number of specific patterns including diffuse scale type, black dotted type, discrete areas of pustules with excoriation and lastly kerion, which is an isolated inflammatory lesion[9]. Each pattern must list a differential diagnosis encompassing seborrheic dermatitis, psoriasis vulgaris, alopecia, furunculosis, and trichotillomania[3]. The level of host immunity and the type of fungal organism involved with the disease can lead to inflammatory type of tinea capititis which is highly confounding with symptoms that of bacterial infection[10],[11],[12]. Although numerous case studies and reports regarding the misdiagnosis have been reported no clinical survey of multi-centered study regarding the rate or burden of misdiagnosis has been evaluated. In the present study, a retrospective analysis between the correctly diagnosed group (group 1) and initially misdiagnosed group (group 2) were compared to evaluate various clinical aspects with the following burden created from the difference.
1. Demographic analysis
The demographic study revealed that TC was most commonly misdiagnosed in children. As the most common age group of TC occurs in children, definitive number also outnumbers rest of the population. The mean age and the percentage of the misdiagnosed group under 18 years of age was 5.82 and 63.29%, respectively. It was found that most of pediatric patients seek management initially from pediatricians and the highest misdiagnosed group of specialty was pediatrics with over 34.9% of all misdiagnosed cases. This was similar with group 1, where only 8% of the cases were correctly diagnosed by pediatricians (Table 2). On the other hand dermatologists were the group with the highest diagnostic precision, summing up to 78.4% in group 1. Additionally revisits in group 2 for making the correct diagnosis was most prevalent in dermatology clinics (55.6%) (Table 2). Dermatophytosis commonly presents in cutaneous manifestation and dermatologists are highly aware of the disease[13]. In addition, the methods used to diagnose TC such as potassium hydroxide smear and fungal culture prevalently prescribed by dermatologist additionally factor accurate diagnosis. Moreover, a retrospective study regarding the epidemiology of TC in the United States reported that 0.1% of the study population was hospitalized from their primary physicians and 71% of the patients were newly diagnosed of TC[14]. Therefore pediatricians or any medical provider regardless of specialty should be aware of the symptoms of TC and make appropriate referrals upon suspicious cases. In fact, guidelines stated by the American Family Physicians insist a thorough history of risk factors including recent contact with livestock, moist boggy appearance in addition to stressing the importance of fungal specific examinations[15]. Lower incidences of TC were reported expected in various clinical studies based on misdiagnosis or under-diagnosis of the disease. Spreading of infection among indigent African Americans along with the group lacking health insurance may factor the cause as well[14].
2. Clinical manifestation and complications
The symptoms and lesions presented between two groups were comparable in terms of progression and complication of the disease. In group 1, pruritus was the highest complaint with 22.7% fol- lowed by scales, pustule and papules. The symptoms and lesions reported in group 1 are consistent with the primary lesions that are usually present in TC. On the contrary, although pruritus and primary lesions were also noticed in group 2, scarring alopecia was the most commonly presented lesion with higher rates of ulcers and seborrhea (Table 2). The result indicates that the misdiagnosed group was more susceptible to lesions that were consistent with complication. Concurrently, the misdiagnosed group showed a higher rate of complication. In group 1 only 41% (9 cases) were left with complications which included scars, hair loss, and dents on scalps. In group 2, 96% (61 cases) suffered complication and scar (41%) was the major complication followed by bacterial co-infection, and hair loss (Table 2). Bacterial co-infection may occur under large superficial crusts and present in forms of folliculitis[16].
3. Diagnosis, treatment and financial deficit
Statistically, potassium hydroxide preparation was the highest form of diagnostic measure per- formed in group 1 followed by fungal culture, Gram swab culture, skin biopsy and hair pluck tests (Table 2). The least valuable test used for differentiating TC was blood culture, and folliscope examination. A Bayesian analysis of conventional methods used for TC, including microscopic evaluation and fungal culture revealed 87.5% of efficiency in true positive values and 76.4% of efficiency in true negative values in which states the high sensitivity arriving at a diagnosis[17]. In other words, differential with microscopic evaluation and fungal culture must be encountered for making fewer misdiagnoses. Due to the confounding symptoms and lack of proper diagnostic measures, the majority of patients in group 2 was initially diagnosed of bacterial infection and was treated with oral antibiotics. In fact, there are numerous reports concerning TC and its clinical mimicry to bacterial infection. Dissecting cellulitis, bullous impetigo, and folliculitis were some of the commonly reported misdiagnosis in relation to bacterial colonization of TC[18],[19],[20]. Additionally psoriasis, seborrheic dermatitis, and allergic urticarial were inflammatory disorders that were frequently misdiagnosed[21],[22].
Treatments in regards to the misdiagnoses result in inappropriate medical prescriptions and prolongation of the disease course. The difference between group 1 and group 2 was noticed as oral or topical anitfungals were more prevalently prescribed in group 1, while third generation cephalosporin followed by first generation cephalosporin was more commonly prescribed in the misdiagnosed group. Efficacy regarding the treatment upon prescribed medication revealed a statistically significant level time difference for group 2 with a p-value of 0.023 (Table 2). Pomeranz et al. reported that majority of admitted patients presumed bacterial infection resulted in major management changes consisting either addition of griseofulvin, or discontinuation of antibiotics[6]. From our experience, it takes about 34.24 days in group 1 and 65.21 days in group 2 until clinical manifestation resolve and mycological identification to be negative. Two cases of the misdiagnosed group suffered extensive surgical debridement, however clinical improvement was not achieved and unnecessary hospitalization with prolongation of treatment was required before providing appropriate treatment[6],[7].
Misdiagnosis of TC leads to further complication and results in significant finical deficits within the groups. In the present study, the misdiagnosed group was visited on average of 3.4 local clinics and 1.7 tertiary based hospitals before coming to DCUMC for the correct diagnosis. On average of 2.5 prescriptions were given to these patients and each patient had made 7.2 trips on average before achieving the right diagnoses. Higher number of clinic visits, medication prescriptions, and trips were the main factors to consider the financial loss of the misdiagnosed subjects. An exact number of costs, however, was not achieved due to the limitations of a retrospective study. However the financial burden, complication and prolonged treatment course all factor negative outcomes in the disease progression. A comparative study states an average loss of 37,955 United States Dollars (USD) for ten unnecessary admission caused by misdiagnosis tinea capitis as bacterial infection[6]. In United States, annual cost of treating TC patients was estimated to be on average $253 per patient, composed of $158 for prescription drugs and $95 for medical services. Misdiagnosis adds additional financial burden up to double the amount[6],[23],[24].
CONCLUSION
Currently, there
are no carefully controlled studies regarding the epidemiologic analysis of misdiagnosed
TC and its evaluation of its clinical and social impact. The misdiagnosed
TC usually arises from unawareness of the disease that leads to inappropriate
diagnostic approach resulting in misleading medication prescription. The
clinical duration and complications were reported to be higher and the
financial loss was evident in the misdiagnosed group. Limited
cases and retrospective study nature in a single center remain limitations to the study.
However, based on the findings, the present study should provide a basis for
further epidemiologic analysis and it is recommended to explore solutions for early diagnosis and
solving patients' quality of lives with economic burden of TC.
References
1. Zienicke HC, Korting HC, Lukacs A, Braun-Falco O. Dermatophytosis in children and adolescents: epidemiological, clinical, and microbiological aspects changing with age. J Dermatol 1991;18:438-446
Crossref
Google Scholar
2. Hay RJ. Tinea capitis: current status. Mycopathologia 2017;182:87-93
Google Scholar
3. Elewski BE. Tinea capitis: a current perspective. J Am Acad Dermatol 2000;42:1-20
Crossref
Google Scholar
4. Thoma-Greber E, Zenker S, Röcken M, Wolff H, Korting HC. Surgical treatment of tinea capitis in childhood. See comment in PubMed Commons below Mycoses 2003;46:351-354
5. Hubbard TW. The predictive value of symptoms in diagnosing childhood tinea capitis. Arch Pediatr Adolesc Med 1999;153:1150-1153
Crossref
Google Scholar
6. Pomeranz AJ, Fairley JA. Management errors leading to unnecessary hospitalization for kerion. Pediatrics 1994;93:986-988
Google Scholar
7. Hyun DN, Chung H, Park JS, Jun JB. A clinical and mycological study of dermatophytoses in children. Korean J Med Mycol 2009;14:69-78
Google Scholar
8. Krowchuk DP, Lucky AW, Primmer SI, McGuire J. Current status of the identification and management of tinea capitis. Pediatrics 1983;72:625-631
Google Scholar
9. Gupta AK, Hofstader SL, Adam P, Summerbell RC. Tinea capitis: an overview with emphasis on management. Pediatr Dermatol 1999;16:171-189
Crossref
Google Scholar
10. Stein DH. Fungal, protozoa, and helminth infections. In: Schachner LA, editors. Pediatric Dermatology. New York: Churchil Livingstone, 1988:1415-1421
11. Ormsby OS. Montgomery H. Diseases of the skin. Philadelphia: Lea & Febiger 1984:1074
Crossref
12. Davidson AM, Gregory PH, Birt AR. A clinical and mycological study of suppurative ringworm. Can Medical Assoc J 1934;31:587-591
Google Scholar
13. John AM, Schwartz RA, Janniger CK. The kerion: an angry tinea capitis. Int J Dermatol 2016. doi: 10.1111 /ijd.13423
Crossref
Google Scholar
14. Suh DC, Friedlander SF, Raut M, Chang J, Vo L, Shin HC, et al. Tinea capitis in the United States: diagnosis, treatment, and costs. J Am Acad Dermatol 2006;55:1111-1112
15. Ely JW, Rosenfeld S, Seabury Stone M. Diagnosis and management of tinea infections. Am Fam Physician 2014;90:702-710
Google Scholar
16. McGinley KJ, Leyden JJ. Antifungal activity of dermatological shampoos. Arch Dermatol Res 1982;272: 339-342
Crossref
Google Scholar
17. Rath S, Panda M, Sahu MC, Padhy RN. Bayesian analysis of two diagnostic methods for paediatric ringworm infections in a teaching hospital. J Mycol Med 2015;25:191-199
Crossref
Google Scholar
18. Torok RD, Bellet JS. Tinea capitis mimicking dissecting cellulitis. Pediatr Dermatol 2013;30:753-754
Crossref
Google Scholar
19. Feetham JE, Sargant N. Kerion celsi: a misdiagnosed scalp infection. Arch Dis Child 2016;101:503. doi: 10.1136/archdischild-2015-309756
Crossref
Google Scholar
20. Stein LL, Adams EG, Holcomb KZ. Inflammatory tinea capitis mimicking dissecting cellulitis in a postpubertal male: a case report and review of the literature. Mycoses 2013;56:596-600
Crossref
Google Scholar
21. Chowdhury B, Kwon O, Kim H, Kwon H, Park K, Chung H, et al. Histopathologically confirmed tinea capitis misdiagnosed as psoriasis. Korean J Med Mycol 2016;21:135-137
Google Scholar
22. Mirmirani P, Tucker LY. Epidemiologic trends in pediatric tinea capitis: a population-based study from Kaiser Permanente Northern California. J Am Acad Dermatol 2013;69:916-921
Crossref
Google Scholar
23. Pomeranz AJ, Sabnis SS. Tinea capitis: epidemiology, diagnosis and management strategies. Paediatr Drugs 2002;4:779-783
Crossref
Google Scholar
24. Williams JV, Eichenfield LF, Burke BL, Barnes-Eley M, Friedlander SF. Prevalence of scalp scaling in prepubertal children. Pediatrics 2005;115:1-6
Crossref
Google Scholar
