pISSN : 3058-423X eISSN: 3058-4302
Open Access, Peer-reviewed
pISSN : 3058-423X eISSN: 3058-4302
Open Access, Peer-reviewed
Jung Hwan Lee,Chung Kee Chough,Su Mi Choi
http://dx.doi.org/10.17966/KJMM.2017.22.3.117 Epub 2017 September 29
Abstract
Keywords
Candida albicans Candidemia Spondylitis Discitis
INTRODUCTION
Candida infections are increasing due to the growth of predisposing factors such as neutropenia, prior receipt of broad-spectrum antibiotics, prolonged corticosteroids or intravascular catheters[1]. Also, repeated Candida infection is increasing[1],[2],[3]. Infections such as Candida endocarditis or oropharyngeal candidiasis are well recognized to recur despite antifungal therapy[4],[5]. But, few data exist on candida spondylodiscitis following bloodstream Candida infection. We report on a rare case of Candida spondylodiscitis after candidemia.
CASE
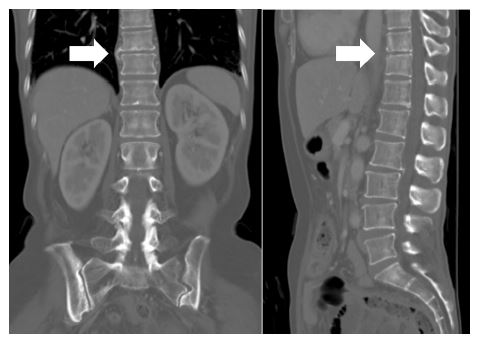
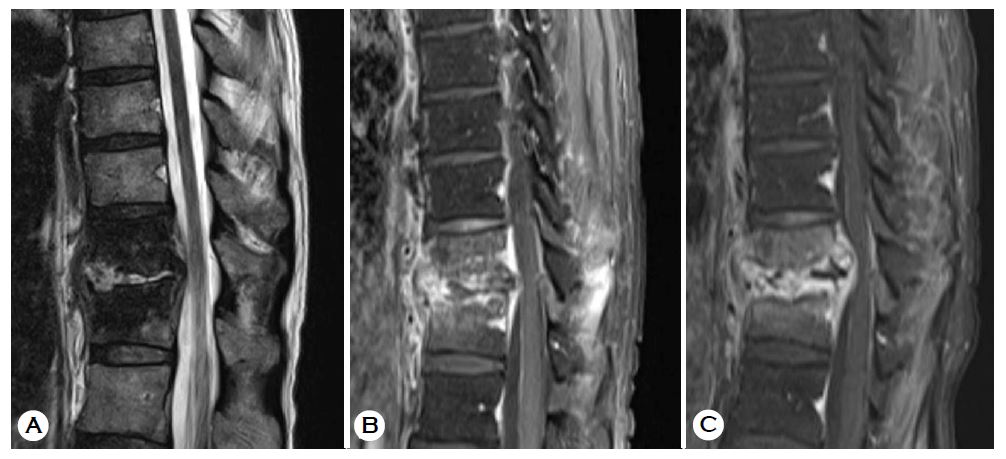
A 66-year-old woman to have been underwent chemotherapy (Carboplatin-Paclitaxel) for ovarian cancer was diagnosed with candidemia associated with the central venous catheter. Ocular candidiasis also diagnosed but, there was no evidence of endocarditis. Ocular involvement was confirmed only in the vitreous body. The catheter was removed, and antifungal agent (fluconazole) was administrated until two weeks after no detection of fungus in the blood culture. The doe of fluconazole was 400 mg/day and total duration of fluconazole use was 5 weeks. Then, after the Chemoport® insertion, the 4th chemotherapy for ovarian cancer was performed. Neutropenic fever occurred after the 4th chemotherapy. Blood cultures were negative and piperacillin-tazobactam was administrated. The number of neutrophil was recovered and no more fever was identified. There was no complication during the 5th and 6th chemotherapy. But, she was hospitalized after the 6th chemotherapy because of abdominal pain and diarrhea. Computed tomography (CT) scans of abdomen demonstrated non- specific colitis. Abnormal finding was not identified in the spine (Fig. 1). Pseudomembranous colitis (PMC) was diagnosed through sigmoidoscopy. After metronidazole administration, she was improved and discharged. But, she revisited after 2 weeks due to severe back pain and fever. Magnetic resonance image (MRI) demonstrated spondylodiscitis on the 10th~11th thoracic spine with epidural abscess (Fig. 2). But, it was negative study in culture from vertebral bone biopsy and blood, so second generation cephalosporin (cefoxitin) was administrated. However, the infection was worsen on follow-up MRI study after a month (Fig. 2). Open curettage and spinal stabilization was performed (Fig. 3). C. albicans was identified. The isolate was sensitive to amphotericin B, caspofungin, fluconazole, flucytosine and voriconazole. Eye examination was per- formed, but ocular candidiasis was much improved. Fluconazole was administrated intravenously for two months and the patient was discharged. Additional oral fluconazole was administrated. The dose was 400 mg/day. Total duration of fluconazole was 4 months. C-reactive protein (CRP) and erythrocyte sedimentation rate (ESR) were normalized at 6 weeks after using oral fluconazole. The back pain was improved and there was no neurologic deficit. The follow-up x-ray image showed no significant difference from the initial postoperative image, and there was no evidence of spondylodiscitis aggravation.

DISCUSSION
The contamination routes of infective spondylitis were generally known to hematogenous spread, spread from contiguous infected tissue, direct inoculation or post-operative infection[6]. In our case, we suspected that the spondylodiscitis happened through the hematogenous route. There were several reasons. At first, there was no infection focus to be contiguous to thoracic spines on abdomen CT scans before two weeks. Second, there was no history of penetrating wound to enable direct inoculation. Finally, there was no medical history of the invasive procedure or the surgery at the thoracic spine. So, this spondylodiscitis might result from bloodstream infection of C. albicans.
Candida spondylodiscitis after candidemia has been rarely reported[7]. Early detection and treatment of spondylodiscitis was important because that caused severe disability such as paraplegia. Early symptom of spondylodiscitis was simple back pain. However, because simple back pain was relatively a common symptom, so it was easy to overlook. Thus, clinicians should be aware of this entity, if the patient who completely treated candidemia complained of back pain.
The ideal treatment of Candida spondylodiscitis has been not established. Amphotericin B has been considered as the treatment of choice, but the azoles, if susceptible, have also been used with good results[8],[9]. Miller et al recommend 4~6 weeks of intravenous amphotericin B therapy followed by oral fluconazole for 2~6 months[8]. The Infectious Diseases Society of America (IDSA) recommendations for vertebral Candida osteomyelitis include surgical debridement and an initial course of amphotericin B for 2~3 weeks, followed by fluconazole for a total duration of 6~12 months[10]. The European Society for Clinical Microbiology and Infectious Disease (ESCMID) guidelines for treating Candida spondylodiscitis recommended strongly to use fluconazole for 6~12 months if the species is susceptible, and fluconazole may be preceded by induction phase with lipid-based amphotericin B[11]. In this case, we initially administrated fluconazole intravenous for two months. Then, oral fluconazole was administrated for two months. ESR and CRP was normalized after using fluconazole for 3.5 months.
For candidemia management, many authors have emphasized the importance of intravascular catheter removal[1],[12],[13]. In the first cadidemia, we followed this principle. However, this patient's the central venous line (Chemoport®) was not removed when treating spondylodiscitis. Because other venous lines for the intravenous antifungal agent could not find due to repetitive chemotherapy and there was no evidence of the central venous line infection. There was no tenderness or redness near the central venous line and blood culture from the central venous line was negative.
CONCLUSION
We report a rare case of late onset Candida spondylodiscitis following candidemia. And, although back pain is an ambiguous symptom, clinicians should be aware of this entity if they have sustained back pain in a recently treated candidemia patient.
References
1. Clancy CJ, Barchiesi F, Falconi DiFrancesco L, Morris AJ, Snydman DR, Yu VL, et al. Clinical manifestations and molecular epidemiology of late recurrent candidemia, and implications for manage- ment. Eur J Clin Microbiol Infect Dis 2000;19:585 -592
Crossref
Google Scholar
2. Asmundsdottir LR, Erlendsdottir H, Gisladottir AL, Gottfredsson M. Molecular epidemiology of late recurrent candidaemia--a population-based study in Iceland. Clin Microbiol Infect 2012;18:195-201
Crossref
Google Scholar
3. Da Matta DA, Melo AS, Guimaraes T, Frade JP, Lott TJ, Colombo AL. Multilocus sequence typing of sequential Candida albicans isolates from patients with persistent or recurrent fungemia. Med Mycol 2010;48:757-762
Google Scholar
4. Nguyen MH, Nguyen ML, Yu VL, McMahon D, Keys TF, Amidi M. Candida prosthetic valve endo- carditis: prospective study of six cases and review of the literature. Clin Infect Dis 1996;22:262-267
Google Scholar
5. Sangeorzan JA, Bradley SF, He X, Zarins LT, Ridenour GL, Tiballi RN, et al. Epidemiology of oral candidiasis in HIV-infected patients: colonization, infection, treatment, and emergence of fluconazole resistance. Am J Med 1994;97:339-346
Crossref
Google Scholar
6. Tyrrell PN, Cassar-Pullicino VN, McCall IW. Spinal infection. Eur Radiol 1999;9:1066-1077
Crossref
Google Scholar
7. Richaud C, De Lastours V, Panhard X, Petrover D, Bruno F, Lefort A. Candida vertebral osteomyelitis (CVO) 28 cases from a 10-year retrospective study in France. Medicine (Baltimore) 2017;96:e7525
Crossref
Google Scholar
8. Miller DJ, Mejicano GC. Vertebral osteomyelitis due to Candida species: case report and literature review. Clin Infect Dis 2001;33:523-530
Google Scholar
9. Cho K, Lee SH, Kim ES, Eoh W. Candida parap- silosis spondylodiscitis after lumbar discectomy. J Korean Neurosurg Soc 2010;47:295-297
Google Scholar
10. Pappas PG, Kauffman CA, Andes D, BenJamin DK Jr., Calandra TF, Edwards JE Jr., et al. Clinical prac- tice guidelines for the management of candidiasis: 2009 update by the Infectious Diseases Society of America. Clin Infect Dis 2009;48:503-535
Google Scholar
11. Cornely OA, Bassetti M, Calandra T, Garbino J, Kullberg BJ, Lortholary O, et al. ESCMID* guide- line for the diagnosis and management of Candida diseases 2012: non-neutropenic adult patients. Clin Microbiol Infect 2012;18 Suppl 7:19-37
Google Scholar
12. Rex JH, Bennett JE, Sugar AM, Pappas PG, Serody J, Edwards JE, et al. Intravascular catheter exchange and duration of candidemia. NIAID Mycoses Study Group and the Candidemia Study Group. Clin Infect Dis 1995;21:994-996
Crossref
Google Scholar
13. Nguyen MH, Peacock JE Jr., Tanner DC, Morris AJ, Nguyen ML, Snydman DR, et al. Therapeutic appro- aches in patients with candidemia. Evaluation in a multicenter, prospective, observational study. Arch Intern Med 1995;155:2429-2435
Crossref
Google Scholar
