pISSN : 3058-423X eISSN: 3058-4302
Open Access, Peer-reviewed
pISSN : 3058-423X eISSN: 3058-4302
Open Access, Peer-reviewed
Byung Gon Choi,Yang Won Lee,Yong Beom Choe,Kyu Joong Ahn
http://dx.doi.org/10.17966/KJMM.2017.22.2.78 Epub 2017 June 25
Abstract
Keywords
Actinic cheilitis Candidiasis Ingenol mebutate gel
INTRODUCTION
Candida is a genus of yeast and usually a com- mensal
organism in humans. However, it occasionally causes various clinical signs
and symptoms depending on the infected anatomical location. Oral
candidiasis, the most common fungal infection in humans, involves lip
manifestations[1]. Angular cheilitis is a typical lesion that is
derived from the inflammation of Candida-affected lips. However, Candida-associated lip lesions can
appear at both the corners of the mouth and the
mid-portion of the lips[2]. Thus, it is sometimes difficult to
distinguish it from other diseases involving lip inflammation, such as actinic
cheilitis (AC).
AC, a major precancerous lesion of the lip, is considered an actinic keratosis on the lip and can progress to squamous cell carcinoma (SCC)[3]. Therefore, early detection and proper treatment are important.
Here we reviewed the medical records of patients with chronic cheilitis who
visited our dermatology clinic. We found two cases of refractory chronic
cheilitis that were initially assessed as Candida associated
lesions. Here we report our experience with chronic cheilitis cases that were
reassessed and managed after histological examinations.
CASE REPORT
Case 1
A
65-year-old woman presented with an erythematous and whitish plaque with
crusting and erosion on the lower lip that had persisted for several months.
There was a white pseudomembranous patch on the lower lip at the initial
visit, and oval budding cells were observed in a potassium
hydroxide (KOH) smear. She had no specific medical history other than
hypertension controlled by medication. We prescribed itraconazole 200 mg/ day for 2 weeks according
to a clinical diagnosis of candidiasis. The pseudomembranous
patch disappeared after antifungal treatment; however, the underlying
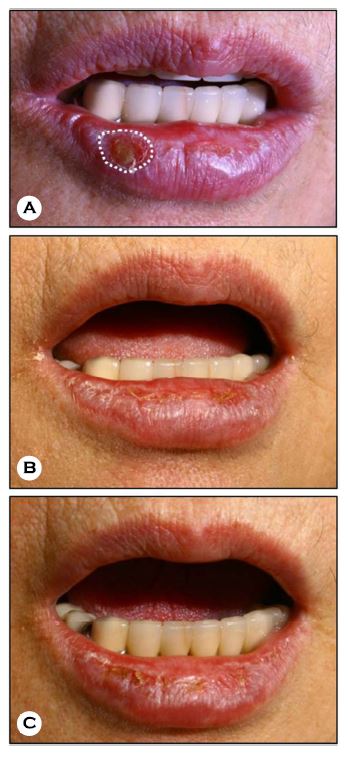
crusting and erosive lesions persisted (Fig. 1A).
A punch biopsy was performed. In the
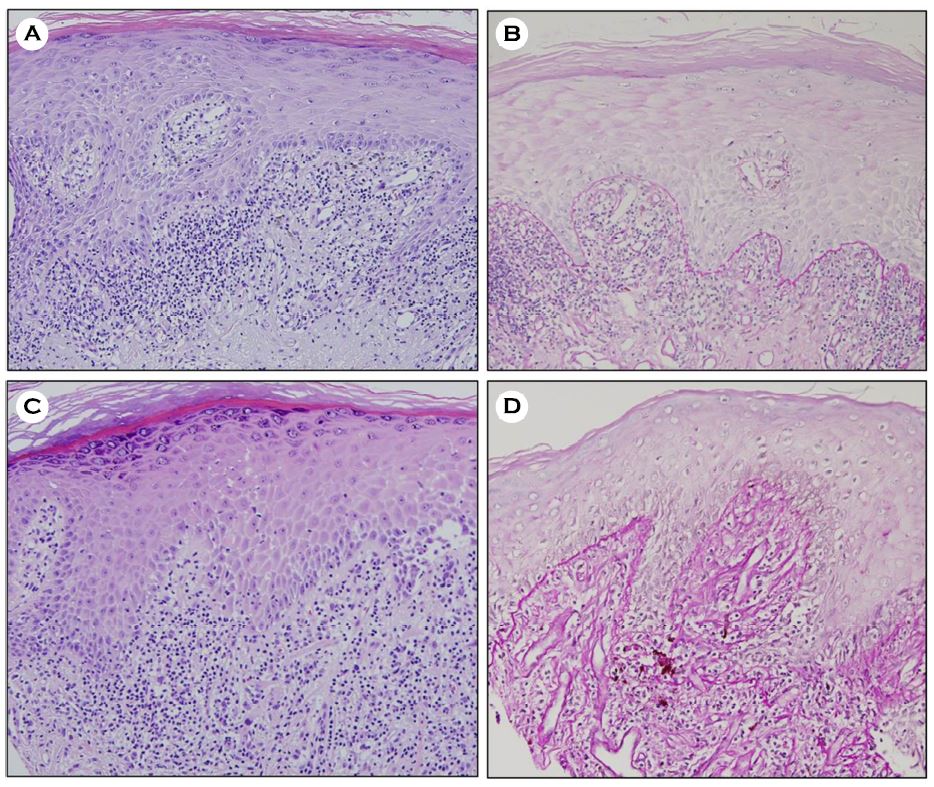
pathologic examination, the epidermis showed hyperkeratosis and acanthosis
with cytologic atypia in the basal cell layer. Solar elastosis and moderate
infiltration of inflammatory cells were observed in the dermis (Fig. 2A). There were no
observed microorganisms on periodic acid-Schiff (PAS) staining (Fig.
2B). Based on the histologic findings, AC was diagnosed.
Cryotherapy was performed; however, no clinical improvement was noted. For further
treatment, we applied 0.015% ingenol
mebutate (IM) gel once daily for 3 days. Because there was insufficient information
about its local skin reaction (LSR) on the lip, the
application was performed in a restricted area (Fig. 1A, white dotted line). We
created a physical barrier with antimicrobial ointment surrounding the
treatment area to minimize the LSR and prevent flow of the IM gel into the
intraoral cavity.
At 4 weeks after
treatment, clinically significant improvement was observed in the treated area. The crusts and erosions
disappeared but the erythema with dead skin remained (Fig. 1B). At 12 weeks
after treatment, however, a mild crust developed (Fig. 1C). The LSR was
tolerable and we planned to apply IM gel to the extended area. However, the patient did not return for
follow-up.
Case 2
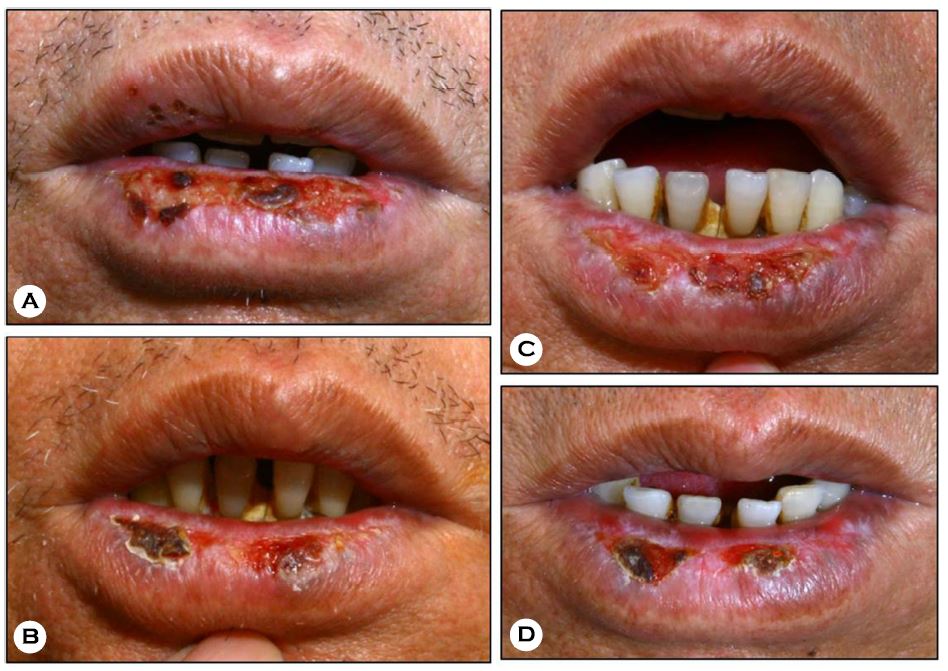
A 65-year-old man presented with an ulcerative plaque and crusting surrounded by a yellowishwhite keratotic rim on the lower lip. Symptoms waxed and waned over several years' time (Fig. 3A). A KOH smear was conducted of the yellowishwhite rim and assembled yeast-like cells with pseudohyphae were observed. He had no specific medical history. We prescribed itraconazole 200 mg/ day for 2 weeks according to the clinical diagnosis of candidiasis. However, no clinical improvement was observed.
A punch biopsy was performed. On the pathology examination, hyperkeratosis, acanthosis, and mild basal cell atypia were observed in the epidermis with lichenoid infiltration of the papillary dermis (Fig. 2C). No fungal material was seen on PAS staining (Fig. 2D) and a diagnosis of AC was made.
Because the lesion did not respond to cryotherapy, we applied 0.015% IM gel for 3 days on all of the erosive and crusty surfaces. We created a barrier with antibiotic ointment as described in case 1. At 8 weeks, partial improvement was noted but the erosion and crusting persisted (Fig. 3B). At 12 weeks after treatment, the lesion widened (Fig. 3C) and we reapplied the IM gel. At 8 weeks after the second application, the lesion had decreased in size but complete remission was not achieved (Fig. 3D).
DISCUSSION
Cheilitis can be classified by its causative factors. For example, sun exposure induces actinic cheilitis, inflammation of the minor salivary glands causes cheilitis glandularis, continuous physical damage can induce exfoliative cheilitis, an allergic reaction causes contact cheilitis, and a candidal infection can cause angular cheilitis. Angular cheilitis is an inflammatory condition of the corners of the mouth that is caused by infection, irritation, or allergies, and Candida is one of the major infection sources[4]. Candidal infection, however, occasionally occurs on the mid-portion of the lip as well as the corners of the mouth[2]. In the present cases, there was a concomitant fungal infection on the existing AC lesions that prevented a precise evaluation at the first assessment.
AC is a precancerous condition of the lip that can progress to SCC, which has a higher risk of metastasis and disease-specific death than SCC at other locations[5]. Therefore, early detection and effective treatment of AC are important. Surgery, cryotherapy, topical 5-fluorouracil, topical imiquimod, and pulsed carbon dioxide laser are possible treatments of choice; however, unsatisfactory responses and recurrences are common[6]. Photodynamic therapy is reportedly an effective and safe modality that can be used in field therapy[7]. However, it is not always available.
IM, a plant extract from Euphorbia peplus, has been used as a traditional medicine by Australian aborigines to treat skin lesions. Two concentrations of IM gel were approved for the topical treatment of actinic keratosis by the US Food and Drug Administration in 2012: 0.015% for facial lesions and 0.05% for lesions on the trunk or extremities. Although the exact mechanism of action of IM is not fully understood, it is thought to have a dual mechanism consisting of rapid lesion necrosis followed by a lesion-specific immune response[8]. Treatment trials with IM gel have been performed for AC in Europe[9][10][11], but there are no reports from Asian countries, including Korea.
Since IM gel was originally used to treat actinic keratosis based on the concept of field therapy, its use could be effective in wide AC lesions. However, considering the anatomical features noted in these cases, namely a thin epidermis and inner mucous membrane of the lip, we were concerned about a severe LSR and the flow of IM gel into the oral cavity. Therefore, we used 0.015% IM gel as spot therapy with a physical barrier.
Six of 12 previously reported cases showed complete clearance of the AC lesion after treatment with IM gel. Most LSR were tolerable and resolved within 1~2 weeks. Some patients, however, complained of pain and severe discomfort when eating and one showed an intolerable LSR involving >50% of the lower lip[9][10][11].
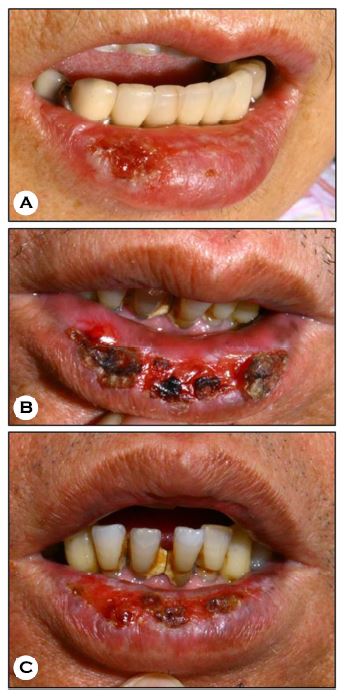
The LSR was tolerable in each of our cases (Fig. 4). However, patients did not show a sufficient response compared to those in previous reports. The local treatment regimen and relatively small amount of gel applied compared with that used in actinic keratosis cases are possible contributing factors. We planned to apply IM gel in a sufficiently wide area to obtain a satisfactory outcome; however, neither patient attended followed-up sessions.
In conclusion, coexisting candidiasis or the development of normal flora in the oral cavity can occur in cases of cheilitis. Furthermore, reassessment by histopathological examination is required to ensure diagnostic accuracy in cases of refractory cheilitis. In addition, IM gel showed acceptable therapeutic effects and a tolerable LSR in the treatment of AC.
Conflict of interest
In relation to this article, I declare that there is no conflict of interest.
References
1. Sharon V, Fazel N. Oral candidiasis and angular cheilitis. Dermatol Ther 2010;23:230-242
Crossref
Google Scholar
2. Terai H, Shimahara M. Cheilitis as a variation of Candida-associated lesions. Oral Dis 2006;12:349 -352
Crossref
Google Scholar
3. Vieira RA, Minicucci EM, Marques ME, Marques SA. Actinic cheilitis and squamous cell carcinoma of the lip: clinical, histopathological and immunogenetic aspects. An Bras Dermatol 2012;87:105-114
Crossref
Google Scholar
4. Park KK, Brodell RT, Helms SE. Angular cheilitis, part 1: local etiologies. Cutis 2011;87:289-295
5. Thompson AK, Kelley BF, Prokop LJ, Murad MH, Baum CL. Risk factors for cutaneous squamous cell carcinoma recurrence, metastasis, and disease-specific death: A systematic review and meta-analysis. JAMA Dermatol 2016;152:419-428
Crossref
Google Scholar
6. Picascia DD, Robinson JK. Actinic cheilitis: a review of the etiology, differential diagnosis, and treatment. J Am Acad Dermatol 1987;17:255-264
Google Scholar
7. Yazdani Abyaneh MA, Falto-Aizpurua L, Griffith RD, Nouri K. Photodynamic therapy for actinic cheilitis: a systematic review. Dermatol Surg 2015;41:189-198
Crossref
Google Scholar
8. Rosen RH, Gupta AK, Tyring SK. Dual mechanism of action of ingenol mebutate gel for topical treatment of actinic keratoses: rapid lesion necrosis followed by lesion-specific immune response. J Am Acad Dermatol 2012;66:486-493
Crossref
Google Scholar
9. Barrado Solis N, Moles Poveda P, Lloret Ruiz C, Pont Sanjuan V, Velasco Pastor M, Quecedo Estebanez E, et al. Ingenol mebutate gel treatment for actinic cheilitis: report of four cases. Dermatol Ther 2015;28:79 -82
Crossref
Google Scholar
10. Florez A, Batalla A, de la Torre C. Management of actinic cheilitis using ingenol mebutate gel: A report of seven cases. J Dermatolog Treat 2017;28:149-151
Crossref
Google Scholar
11. Tzika E, Masouye I, Muhlstadt M, Laffitte E. Ingenol mebutate for recalcitrant chronic actinic cheilitis. Dermatology 2016;232(Suppl. 1):1-3
Crossref
Google Scholar
