pISSN : 3058-423X eISSN: 3058-4302
Open Access, Peer-reviewed
pISSN : 3058-423X eISSN: 3058-4302
Open Access, Peer-reviewed
Yo Sup Shin,Bok Won Park,Eun Byul Cho,Eun Joo Park,Kwang Ho Kim,Kwang Joong Kim
http://dx.doi.org/10.17966/KJMM.2017.22.2.73 Epub 2017 June 25
Abstract
Keywords
Atopic dermatitis Folliculitis Steroid Tinea incognito
INTRODUCTION
Steroid is one of the most commonly prescribed medication for various dermatologic diseases, providing effect through various pharmacologic activity like immunosuppression and anti-inflammation. However, even with proper usage, long-term use of steroid can cause iatrogenic dermatologic diseases. Tinea incognito is a steroid-induced skin condition of a superficial mycosis, characterized by loss of its typical feature such as elevated margin or scale due to decreased inflammatory response[1]. Many case reports and study concludes these atypical feature most often resemble eczema (82%), and others resemble psoriasis, lupus erythematous, or impetigo[2]. Herein, we present a case of a 27-year-old patient with tinea incognito of trunk and upper arms, who was first misdiagnosed as aggravated atopic dermatitis with folliculitis, with review of literatures.
CASE
The patient is a 27-year-old male, who had visited dermatologic clinic with complaint of pruritic erythematous macules and nodules, first manifested a month ago. Previous treatment included systemic and topical steroid and systemic roxithromycin for six weeks under the impression of aggravation of atopic dermatitis and secondary bacterial infection, but the symptom had not improved.
Since childhood he had been
taking both oral and topical steroid and antihistamine for atopic dermatitis;
he had a history of truncal folliculitis which was
treated with oral doxycycline. There was no specific family or social history,
nor a history of animal contact.
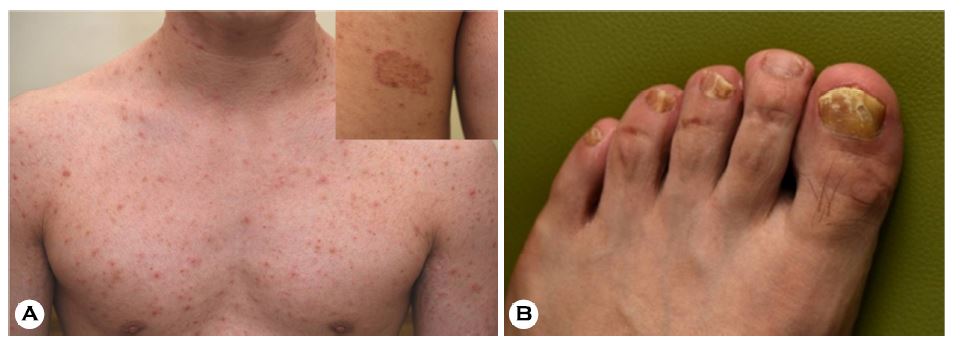
Erythematous macules and
papules, scattered widely on the upper trunk involving front chest and back area was noticed, and
the same lesions were also found on both shoulders and upper arms (Fig. 1A). In
addition, thick and easily broken yellow toenails with onset of two years ago were noticed (Fig.
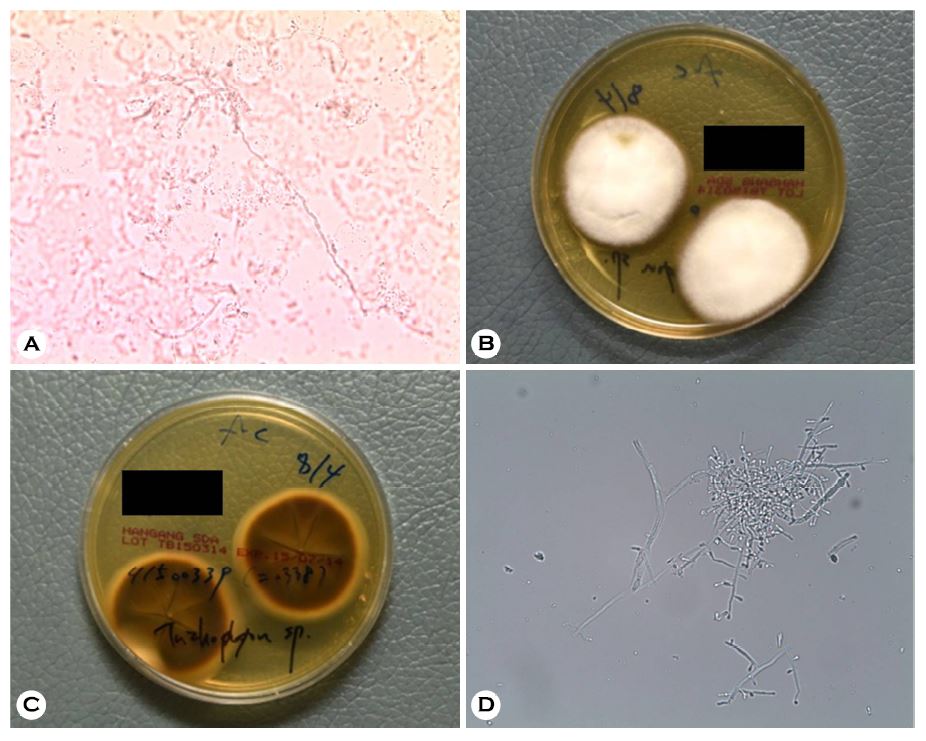
1B). Lab findings were within normal range. KOH exam was done on one of the papules and first
toenail, and hyphae were observed in both specimens (Fig. 2A). Scales from the
lesions were cultured for three weeks on Sabouraud's dextrose agar plate,
revealing elevated white cotton-like hyphae with dark reddish colony on the
back side of the plate (Fig. 2B, 2C). Slide
specimen was made from this colony and dyed with lactophenol cotton blue,
which showed many teardrop-like microcon- idia under the
microscope; the pathogen was identified as Trichophyton
rubrum (Fig. 2D).
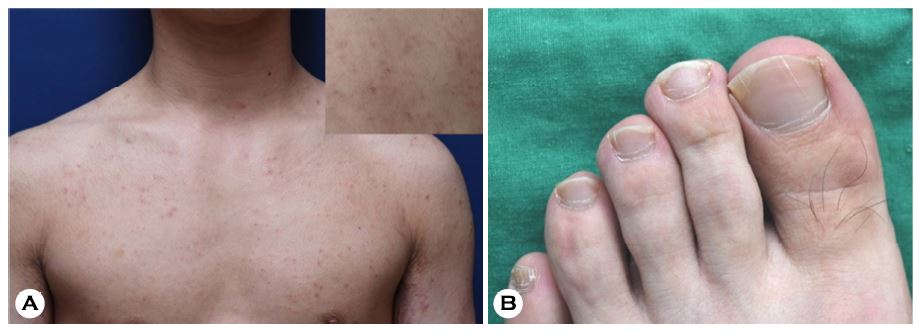
With confirmed diagnosis of tinea incognito by Trichophyton rubrum and concomitant
onycho- mycosis, 12 weeks course of oral itraconazole 200 mg/day and 1%
Flutrimazole ointment was started. The patient has recovered over time and the
skin lesion improved with partial pigmentation (Fig. 3A, 3B).
DISCUSSION
Treatment must be preceded
by accurate diagnosis, and visual inspection is one of the most important
tools of diagnosis. This is especially true in dermatologic diseases,
where a number of diseases can be diagnosed with visual inspection
alone. However,
atypical presentation may delay diagnosis and mislead the doctors; tinea
incognito is one of such examples.
Tinea incognito is defined as superficial fungal infection with loss of typical presentation due to prior use of steroid medication, and was first reported by Ive and Marks in 1968[3]. As topical steroids and immunosuppressants like calcineurin inhibitors are being more and more used in many skin diseases like atopic dermatitis, psoriasis, contact dermatitis, or seborrheic dermatitis, tinea incognito has become more common and more studies are being published[2]. Its atypical presentation is thought to be caused by suppression of inflammation against fungi by immunosuppressants[4]. This allows fungi to slowly proliferate with relatively less erythema and scale, resulting in the lack of typical features.
Various
fungi are responsible for tinea incognito, and Trichophyton rubrum consists about 70% of total pathogen
in Korea, followed by Trichophyton mentagrophytes
and Microsporum canis. This is in accordance
with the study published in Italy, while the study in Iran
reported Trichophyton verrucosum to be most common, and Trichophyton rubrum accounts for about
12% of the cases[5][6]. The reason Trichophyton rubrum is the most common pathogen is that it is one of anthropophilic
dermatophyte, and is also the most common pathogen of human superficial fungal
infection. In Iran, the most common fungus causing superficial
infection is reported to be Epidermophyton
floccosum, and Trichophyton verrucosum is the third most common pathogen[7]. Tinea
incognito in Iran occurs mostly in rural area where contact with livestocks are
common, and the superficial infection in the case of frequent contact with
livestocks is most often caused by Trichophyton
verrucosum, explaining how the same pathogen is responsible for tinea
incognito in the most cases[8].
The patient in this case had had treatment for atopic dermatitis, and had onychomycosis since two years ago. Patients with atopic dermatitis are more prone to fungal infection, and onychomycosis may cause autoinoculation of the pathogen[9][10]. One study suggests the risk factors of tinea incognito are 1) Persistent erythematous, scaly skin lesion, 2) Lesions unresponsive to steroid or calcineurine inhibitors, 3) Lesions on truncal or facial area, 4) Concomittant fungal infection such as tinea pedis, onychomycosis, etc., 5) patients with suppressed immunity or taking immunosuppressants. If these risk factors are present, one must suspect tinea despite inconsistent features, and confirm the diagnosis with KOH exam and fungal culture[2].
Tinea incognito has shown various manifestations, but folliculitis-like features have been rarely reported. Akram A et al.[6] have argued topical steroids against skin infection might cause deeper fungal invasion into follicles.
Our case was the case of tinea incognito, misdiagnosed
as folliculitis with atopic dermatitis aggravation
because of previous history of folliculitis a year
ago and signs of erythematous nodules, macules and patch. These lesions can spread to
trunk and upper extremities and exacerbate atopic dermatitis, so
accurate diagnosis by KOH exam and fungal culture, and antifungal
treatment is necessary. Pityrosporum folliculitis can be considered as a differential
diagnosis. However, the presence of macular patch lesions and surrounding
papular lesions is thought to have spread from dermatophyte
infection. In addition, folliculitis lesions were confirmed by Trichophyton rubrum through myco- logical
examination. Therefore, it was diagnosed to be tinea incognito by Trichophyton rubrum rather than
pityrosporum folliculitis
We authors report a case of tinea incognito with
features mimicking folliculitis, in the patient with atopic dermatitis and
onychomycosis, believing it will help future dermatologic practice.
Conflict of interest
In relation to this
article, I declare that there is no conflict of interest.
References
1. Kim SY, Youn HJ, Jung HJ, Jung JW, Lee YW, Choe YB, et al. Tinea incognito due to Trichophyton rubrum in atopic dermatitis patient. Korean J Med Mycol 2014;19:59-63
Google Scholar
2. Kim WJ, Kim TW, Mun JH, Song M, Kim HS, Ko HC, et al. Tinea incognito in Korea and its risk factors: nine-year multicenter survey. J Korean Med Sci 2013;28:145-151
Crossref
Google Scholar
3. Ive Fa, Marks R. Tinea incognito. Br Med J 1968; 3:149-152
Crossref
Google Scholar
4. Rallis E, Koumantaki-Mathioudaki E. Pimecrolimus induced tinea incognito masquerading as intertriginous psoriasis. Mycoses 2008;51:71-73
Crossref
Google Scholar
5. Romano C, Maritati E, Gianni C. Tinea incognito in Italy: a 15-year survey. Mycoses 2006;49:383-387
Crossref
Google Scholar
6. Ansar A, Farshchian M, Nazeri H, Ghiasian SA. Clinico-epidemiological and mycological aspects of tinea incognito in Iran: A 16-year study. Med Mycol J 2011;52:25-32
Crossref
Google Scholar
7. Aghamirian MR, Ghiasian SA. Dermatophytoses in outpatients attending the Dermatology Center of Avicenna Hospital in Qazvin, Iran. Mycoses 2008; 51:155-160
Crossref
Google Scholar
8. Aghamirian MR, Ghiasian SA. Dermatophytes as a cause of epizoonoses in dairy cattle and humans in Iran: epidemiological and clinical aspects. Mycoses 2011;54:e52-56
Crossref
Google Scholar
9. Yoo KH, Kim JY, Li K, Seo SJ, Hong CK. Superficial fungal infection in patients with atopic dermatitis. Korean J Dermatol 2009;47:1-5
10. Szepietowski JC, Matusiak L. Trichophyton rubrum autoinoculation from infected nails is not such a rare phenomenon. Mycoses 2008;51:345-346
Crossref
Google Scholar
