pISSN : 3058-423X eISSN: 3058-4302
Open Access, Peer-reviewed
pISSN : 3058-423X eISSN: 3058-4302
Open Access, Peer-reviewed
Yeong Ho Kim,Young Min Park,Jun Young Lee,Ji Hyun Lee
http://dx.doi.org/10.17966/KJMM.2017.22.1.34 Epub 2017 March 31
Abstract
Keywords
Cryptococcus Bone marrow transplant Leukemia
서 론
크립토콕쿠스(Cryptococcus) 종은 5~10 μm 직경의 구형 내지 타원 형태로 다당류로 이루어진 피막에 쌓여 있고, 좁은 기저부 형태로 발아(narrow-based budding)하는 효모이다[1],[2]. C. neofor- mans, C. gattii 등과 같은 크립토콕쿠스 종에 의해 크립토콕쿠스증(Cryptococcosis)이 발생하고, 이중에서도 면역 저하 환자에서 주요한 감염을 일으키는 것은 C. neoformans이다[1]. C. neoformans는 조류 분비물로 오염된 토양이나 부패한 나무, 채소, 먼지 등에서 존재하여 어디에서나 발견될 수 있다[2]. 피부 병변은 보통 여드름 모양이고, 이외에 결절, 궤양, 봉와직염, 지방종, 농양, 켈로이드, 육아종, 괴저성 농피증, 기저세포암, 사마귀, 전염물렁종, 각화 극세포종 등의 다양한 형태로 나타날 수 있다,[2],[3],[4]. 크립토콕쿠스증을 진단하는 방법에는 첫 번째로 뇌척수액이나 체액의 India ink를 이용해 진단하거나, 두 번째로 감염된 조직으로 크립토콕쿠스의 특징적인 형태를 이용해 다양한 염색을 통하여 진단할 수 있고, 세 번째로 체액의 혈청학적 검사로 피막 항원으로 진단할 수 있으며, 네 번째로 체액이나 조직을 배양하여 진단할 수 있다[1],[5]. 본 저자들은 급성 림프구성 백혈병으로 골수이식한 환자에서 발생한 크립토콕쿠스 감염을 경험하고 드문 증례로 생각되어 보고한다.
증 례
환 자: E OO, 16세, 남자 (국적: 아랍에미레이트)
주 소: 2주 전부터 전신에 발생한 다발성의 홍반성 내지 갈색의 구진들
현병력: 급성 림프구성 백혈병으로 1년 전 골수이식 받고, 1개월 전 재발하여 재유도 항암 치료 후 발생한 중성구 감소증과 동반된 폐렴으로 중환자실에서 치료 중인 환자로 2주 전부터 전신에 발생한 다발성의 홍반성 내지 갈색의 구진들을 주소로 입원 중 협진 의뢰됨
과거력: 급성 림프구성 백혈병으로 치료받고 있고, 수두 과거력 있음
가족력: 특이사항 없음
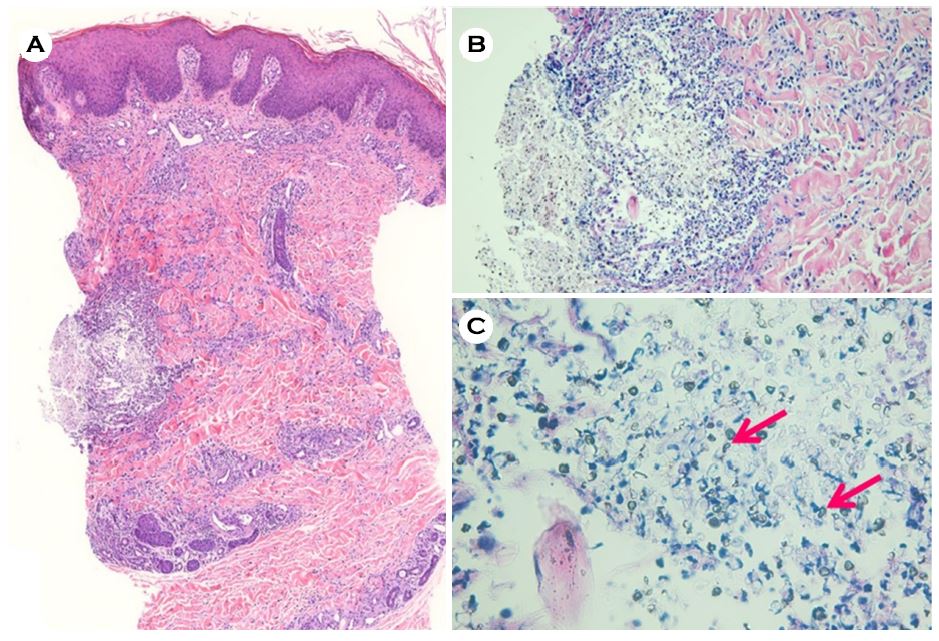
피부 소견: 전신에 다발성의 0.2~0.3 cm 크기의 홍반성 내지 갈색의 구진들이 관찰되었음(Fig. 1)

이학적 소견: 피부 소견 외에 특이 소견 없음
검사 소견: 전체혈구계산에서 전혈구 감소증이 관찰되었고, 흉부 X선에서 우측 폐에 폐렴 소견이 관찰되었다. Human immunodeficiency virus (HIV) 항원, 항체는 음성이었고, 혈액에서 시행한 크립토콕쿠스 항원 검사와 배양결과는 음성이었다. 뇌척수액 검사는 시행하지 못하였다.
진균 검사 소견: 진균 배양 검사 시행하지 못함
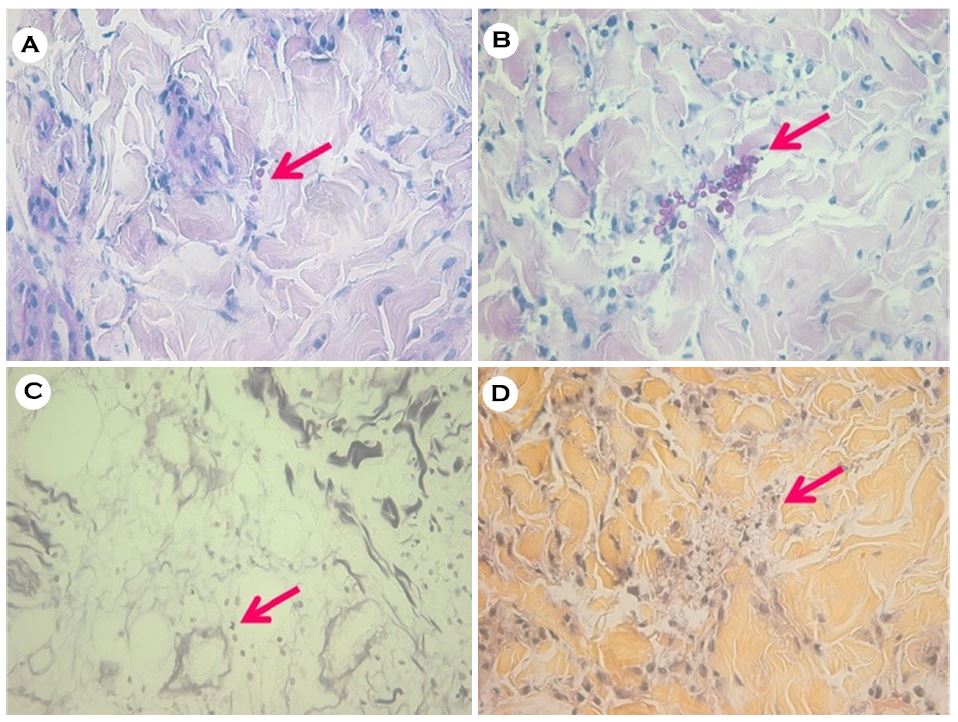
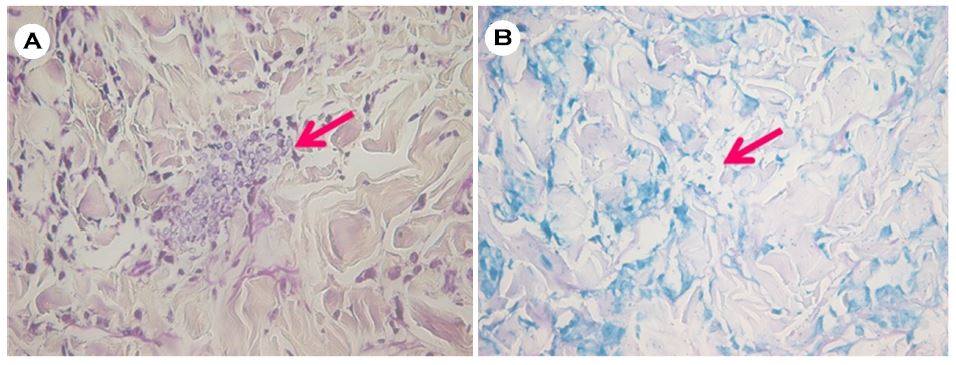
병리조직학적 소견: 홍반성 내지 갈색의 구진에서 시행한 피부 조직 검사상 H&E 염색에서 진피층에 좁은 기저부 형태로 발아하는 효모가 관찰되었다(Fig. 2). 추가적으로 시행한 PAS 염색과 PAS-diastase (PAS-D) 염색에서 분홍색의 효모균이 관찰되었고, GMS 염색에서는 검은색의 효모균이, mucicarmine 염색에서는 분홍색의 피막으로 둘러싸인 효모균이 관찰되었다(Fig. 3). 그람 염색과 Ziehl Neelsen 염색에서는 염색되지 않은 효모균이 관찰되었다(Fig. 4).
진단, 치료 및 경과: 크립토콕쿠스증의 전신 감염에 의한 심재성 진균증으로 진단하고, flucona- zole (600 mg/day)을 정주하였으나 폐렴에 따른 호흡 부전으로 사망하였다.
고 찰
크립토콕쿠스는 주로 중추 신경계에 감염을 일으키는 효모로, 전세계적으로 1년에 60만 명 이상이 크립토콕쿠스 뇌수막염으로 사망한다고 보고되었다[6]. 지난 30년간 HIV 감염이나 스테로이드, 항암 치료, 이식 후 거부 반응 억제 치료와 같은 약제에 의한 후천성 면역 저하 환자들이 증가함에 따라 크립토콕쿠스 감염도 같이 증가하고 있다[7].
크립토콕쿠스증은 호흡기를 통하여 주로 폐가 일차적으로 감염되고, 이어 중추 신경계, 골격, 비뇨생식기, 피부 등 다른 조직으로 전파될 수 있다[1],[2],[3],[4]. 이러한 전신적 감염에서 10~20%에서 피부 침범이 일어날 수 있고, 피부를 관통하는 외상에 의해 일차성 피부 감염도 가능하지만 매우 드물다[2],[3],[4],[8],[9],[10]. 이차성 피부 감염은 주로 면역 저하 환자에서 일어나는 반면에 일차성 피부 감염은 면역 저하 환자뿐만 아니라 정상 면역을 가진 사람에게서도 일어난다[2],[8],[10]. 호흡기를 통해 폐가 일차적으로 감염이 되었을 경우 대부분 무증상이고 혈행성 전파로 중추 신경계에 감염을 일으키면 뇌수막염의 형태로 나타나 두통, 고열, 오심, 경련 등의 증상이 나타난다[3],[11]. 본 증례에서는 급성 림프구성 백혈병으로 조혈모세포 이식 후 면역억제제를 복용하는 환자에서 뇌수막염을 의심할 만한 신경계 증상 없이 피부에 다발적으로 병변이 발생하였고, 특징적인 병리 조직학적 소견으로 피부 크립토콕쿠스증으로 진단하였다. 피부에 특이 외상력이 없었고, 동시에 다발적으로 피부 병변이 발생했다는 점에서 폐를 통한 감염에 이차성 피부 감염이 발생되었을 것으로 추측된다.
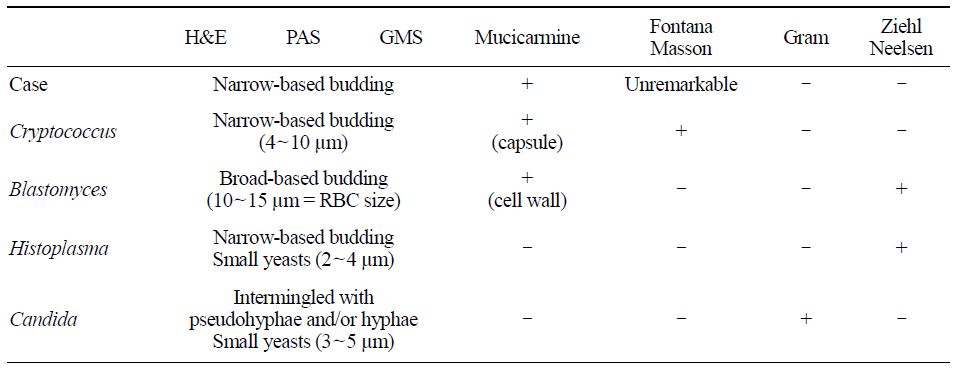
크립토콕쿠스는 좁은 기저부 형태로 발아하는 피막으로 둘러싸인 효모이다. 좁은 기저부 형태로 발아하는 점에서 Candida나 Histoplasma와 감별이 필요한데 Candida는 연속적으로 발아하면서 pseudohyphae의 형태를 띠게 되고, Histoplasma는 주로 대식세포 안에 집단으로 모여있는 점에서 차이가 있다[1]. 또한 크립토콕쿠스는 특징적으로 멜라닌을 함유하고 있어 Fontana-Masson 염색에서 검은색을 띄고, Gram 염색에서는 Histoplasma가 자주색 내지 파란색으로, Ziehl Neelsen 염색에서는 Candida가 붉은색으로 염색이 된다는 점에서 쉽게 감별할 수 있다[1]. PAS, GMS 염색에서는 glycoprotein으로 이루어진 세포벽이 염색이 되면서 다른 진균들과 마찬가지로 각각 분홍색, 검은색을 띄게 된다[1],[2]. 크립토콕쿠스의 세포를 둘러싸고 있는 피막은 두꺼운 polysaccharide로 이루어져 mucicarmine 염색으로는 분홍색으로, alcian blue 염색으로는 파란색으로 염색이 되는 특징이 있어 형태학적 특징과 더불어 다른 진균들과 감별이 가능하다[1],[2]. 본 증례에서는 Fontana Masson 염색에서 특징적으로 검은색으로 염색이 잘 되지는 않았지만 H&E 염색에서 좁은 기저부 형태로 발아하는 효모를 발견할 수 있었고, PAS, PAS-D, GMS에서 염색되는 효모가 관찰되고, mucicarmine 염색에서 분홍색 피막을 관찰하였으며, Gram, Ziehl Neelsen 염색은 되지 않는 것으로 주요한 효모 형태 진균들과 감별하여 크립토콕쿠스증으로 진단할 수 있었다(Table 1). 크립토콕쿠스의 조직을 이용한 형태학적 진단 외에 다른 방법으로는 혈청과 뇌척수액에서 크립토콕쿠스 항원을 검출하는 방법이 있고, 특이도, 민감도가 90% 이상이고, 위양성율이 7% 정도 된다[1]. 하지만 이 검사는 크립토콕쿠스의 피막에 있는 항원을 감지하는 방법을 사용하기 때문에 피막이 잘 발달되어 있지 않았을 때에는 별로 도움이 되지 않는다[1]. 본 증례에서도, 피막을 염색하는 mucincarmine 염색에서 다른 증례에서와 같이 뚜렷한 분홍색으로 잘 염색이 되지는 않았고, 이를 통해 잘 발달되어 있지 않은 피막 때문에 혈액에서 시행한 크립토콕쿠스 항원 검사가 음성으로 나왔을 가능성이 있다. 진단하는 또 다른 방법으로 혈액이나 뇌척수액 혹은 기타 체액을 canavanine-glycine-bromthymol blue 배지에 배양함으로써 C. gatti와 C. neoformans를 구분할 수 있다[1]. 본 증례에서와 같이 피부 병변을 동반한 크립토콕쿠스증에서는 반드시 조직 검사와 다양한 염색 방법을 통해 크립토콕쿠스 감염을 확인하고 호흡기 감염이 동반된 이차성 피부 감염에서 신경 증상이 있을 경우 뇌척수액의 India ink 검사를 통하여 중추 신경계 감염의 여부를 확인하는 것을 권장한다.
크립토콕쿠스증의 치료는 크게 중추 신경계 침범 여부, HIV 감염 여부, 이식 여부에 따라 이들 중 한 가지라도 해당이 되면 유도 치료, 공고 치료, 유지 치료 세 단계에 나누어 총 최소 9개월에서 1년 이상 치료하도록 되어 있고, 해당되지 않더라도 심한 폐 크립토콕쿠스증이나 크립토콕쿠스 혈증이 확인되면 중추 신경계 침범했을 때와 같이 치료하도록 권고하고 있다[12],[13]. 세 단계의 치료를 할 때 유도 치료는 liposomal amphotericin B나 amphotericin B deoxycholate와 함께 5-flucytosine을 체중별로 상황에 따라 2주에서 4주 이상 투여하고, 공고 치료는 fluconazole 400~800 mg/day를 8주간 투여하며, 유지 치료는 fluconazole 200~400 mg/day을 상황에 따라 6개월 내지 1년 이상 투여한다[12],[13]. 정상 면역 환자에서 중추 신경계 침범이나, 폐 크립토콕쿠스증, 크립토콕쿠스 혈증이 없을 경우에는 fluconazole 400 mg/day를 6~12개월간 투여한다[12],[13]. 본 증례에서는 조혈모세포 이식 이후 면역 저하 상태에 있었고, 피부 병변이 발생하기 전부터 중성구 감소증과 함께 폐렴 증상이 있어 경험적 항생제와 liposomal amphotericin B 150 mg을 4주간 투여 중에 있었고, 피부 조직 생검에서 크립토콕쿠스증을 확인하고 fluconazole 600 mg을 투여 시작하였으나 폐렴에 따른 호흡 부전으로 사망하였다.
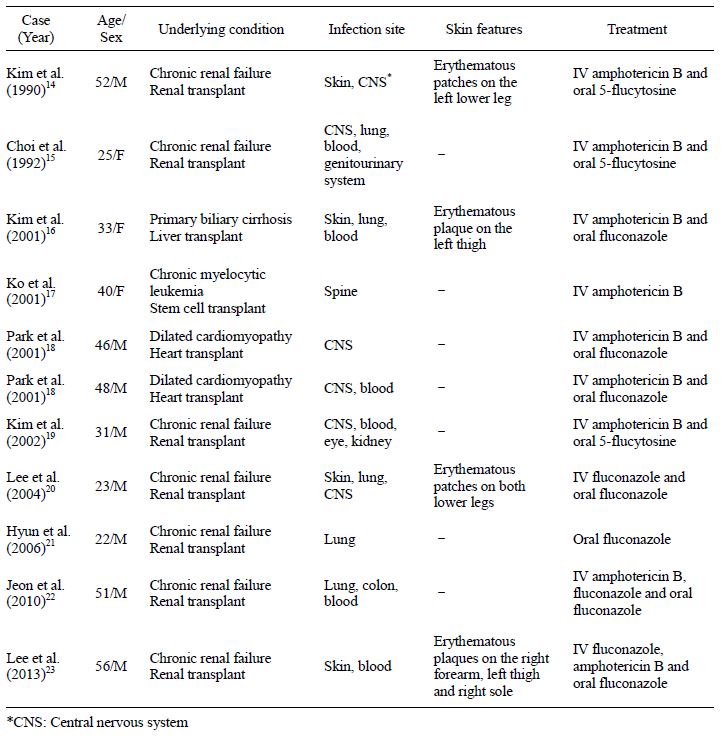
현재까지 국내에 보고된 이식 환자에서 발생한 크립토콕쿠스증은 총 11예로, 신장 이식 환자에서 7예로 가장 많았으며 피부 증상을 동반한 환자는 4예 보고되었다(Table 2)[14],[15],[16],[17],[18],[19],[20],[21],[22],[23]. 만성 골수성 백혈병으로 조혈모세포 이식 받은 환자에서 피부 감염은 없이 척추에 발생한 크립토콕쿠스증 1예가 보고된 바 있다[17]. 아직까지 본 증례에서처럼 백혈병으로 골수이식 받은 환자에서 발생한 피부 크립토콕쿠스증은 보고된 바가 없다. 이와 같이 이식 환자가 증가하는 시점에서 전신에 다발성 구진이 발생한 경우 크립토콕쿠스 감염 등의 진균 감염을 염두에 두어야 할 것으로 생각하고 문헌고찰과 함께 보고한다.
Acknowledgements
"This work was supported by the National Re- search Foundation of Korea(NRF) grant funded by the Korea government (MSIP) (No. NRF-2015R1C1- A2A01054767)".
Conflict of interest
In relation to this article, I declare that there is no conflict of interest.
References
1. Guarner J, Brandt ME. Histopathologic diagnosis of fungal infections in the 21st century. Clin Microbiol Rev 2011;24:247-280
Crossref
Google Scholar
2. Fernandez-Flores A, Saeb-Lima M, Arenas-Guzman R. Morphological findings of deep cutaneous fungal infections. Am J Dermatopathol 2014;36:531-553; quiz 554-536
Crossref
Google Scholar
3. Chung WG, Park J, Park YK, Lee KH. A case of cutaneous cryptococcosis resembling verrucous granu- loma. Korean J Med Mycol 2002;7:42-46
Google Scholar
4. Kim HJ, Min HG, Lee ES. Two cases of cutaneous cryptococcosis mimicking cellulitis. Korean J Med Mycol 1998;3:190-194
Google Scholar
5. Perfect JR, Bicanic T. Cryptococcosis diagnosis and treatment: What do we know now. Fungal Genet Biol 2015;78:49-54
Crossref
Google Scholar
6. Desalermos A, Kourkoumpetis TK, Mylonakis E. Update on the epidemiology and management of cryptococcal meningitis. Expert Opin Pharmacother 2012;13:783-789
Crossref
Google Scholar
7. Pukkila-Worley R, Mylonakis E. Epidemiology and management of cryptococcal meningitis: develop- ments and challenges. Expert Opin Pharmacother 2008;9:551-560
Google Scholar
8. Christianson JC, Engber W, Andes D. Primary cuta- neous cryptococcosis in immunocompetent and immu- nocompromised hosts. Med Mycol 2003;41:177-188
Crossref
Google Scholar
9. Yuge S, Bastazini Junior I, Coelho MC, Soares CT. Cutaneous cryptococcosis in an immunocompetent host. Acta Derm Venereol 2006;86:165-166
Google Scholar
10. Neuville S, Dromer F, Morin O, Dupont B, Ronin O, Lortholary O, et al. Primary cutaneous cryptococcosis: a distinct clinical entity. Clin Infect Dis 2003;36:337 -347
Crossref
Google Scholar
11. Hernandez AD. Cutaneous cryptococcosis. Dermatol Clin 1989;7:269-274
12. Perfect JR, Dismukes WE, Dromer F, Goldman DL, Graybill JR, Hamill RJ, et al. Clinical practice guide- lines for the management of cryptococcal disease: 2010 update by the infectious diseases society of america. Clin Infect Dis 2010;50:291-322
Crossref
Google Scholar
13. Chen SC, Sorrell TC, Chang CC, Paige EK, Bryant PA, Slavin MA. Consensus guidelines for the treatment of yeast infections in the haematology, oncology and intensive care setting, 2014. Intern Med J 2014;44: 1315-1332
Crossref
Google Scholar
14. Kim YS, Kim SI, Park KI, Kim KH, Park CI, Lee HY, et al. Cryptococcal infection in renal trasnplant patient J Korean Soc Transplant 1990;4:121-130
15. Choi SC, Lim DS, Chang K, Song JH. A disseminated crytococcosis after renal transplantation. J Wonkwang Med Sci 1992;24:211-217
16. Kim KJ, Kim HH, Choi JH, Sung KJ, Moon KC, Koh JK. A case of cryptococcosis with skin involvement in a liver transplant recipient Korean J Dermatol 2001;39:1446-1448
Google Scholar
17. Ko Y-H, Lim D-J, Lee S-S, Cho Y-K, Lee D-G, Choi J-H, et al. A case of cryptococcal spondylitis following allogeneic hematopoietic stem cell transplantation. Korean J Infect Dis 2001;33:298-301
Google Scholar
18. Park JH, Lee YJ, Kang SJ, Jeong YH, Jang JS, Chung JW, et al. Cryptococcal meningitis in cardiac trans- plant patients. J Korean Soc Chemother 2001;19: 341-347
19. Kim IT, Kim JY, Kim HG. A case of cryptococcal chorioretinitis in a renal transplant patient. J Korean Ophthalmol Soc 2002;43:922-926
Google Scholar
20. Lee YA, Kim HJ, Lee TW, Kim MJ, Lee MH, Lee JH, et al. First report of Cryptococcus albidus - induced disseminated cryptococcosis in a renal trans- plant recipient. Korean J Med Mycol 2004;19:53-57
Crossref
Google Scholar
21. Hyun Y-Y, Lee J-W, Choi HM, Ko GJ, Kim JY, Kim MG, et al. Asymptomatic cryptococcus and subse- quent symptomatic tuberculosis infection in a renal transplant patient. J Korean Soc Transplant 2006;20: 117-120
Google Scholar
22. Jeon JM, Oh JS, Kim SM, Son YK, Park YK, Sin YH, et al. A case of asymptomatic disseminated cryptococcosis in a renal transplant patient. Korean J Nephrol 2010;29:310-314
Google Scholar
23. Lee SK, Kim HS, Lee JG, Choi JM, Jung IS, Yhi JY, et al. Disseminated cryptococcosis with cutaneous manifestation in a renal transplant recipient. J Korean Soc Transplant 2013;27:132-137
Google Scholar
