pISSN : 3058-423X eISSN: 3058-4302
Open Access, Peer-reviewed
pISSN : 3058-423X eISSN: 3058-4302
Open Access, Peer-reviewed
Tae-Hyoung Kim,Mi-Kyung Lee
http://dx.doi.org/10.17966/KJMM.2017.22.1.15 Epub 2017 March 30
Abstract
Methods: A total 509 isolates including 504 C. albicans and 5 C. dubliniensis were examined for LA test, the presence of "spiking" on blood agar plate, and the germ tube test. Also all isolates were tested using the VITEK 2 ID-YST system.
Conclusions: The data show that the prevalence of C. dubliniensis in Korea is still expected to be extremely low and LA test is very rapid, simple, and reliable tool for the differentiation of C. albicans and C. dubliniensis.
Keywords
Candida albicans Candida dubliniensis Latex agglutination
서 론
최근 진균감염은 지속적으로 증가하고 있으며, 특히 면역이 저하된 환자와 심각한 질병을 가진 환자에서 감염의 중요한 원인이 되고 있다. 칸디다 속은 진균감염의 가장 흔한 원인균이며, 약 40여종이 사람에서 감염을 일으키는 것으로 알려져 있다[1]. 이중 Candida albicans가 가장 흔히 분리되고 있고, 그 다음으로 Candida glabrata, Candida tropicalis, Candida parapsilosis 등이 사람에서 감염을 일으키는 중요한 병원균으로 생각되고 있다[2]. 1995년 아일랜드의 더블린에서 재발성 구강염을 가진 human immunodeficiency virus (HIV) 감염 환자의 구강으로부터 처음 분리된 Candida dublini- ensis도 다양한 검체에서 분리되면서 새로운 병원균으로 보고되고 있다[3],[4].
C. dubliniensis는 발아관(germ tube) 형성, 비후막홀씨(chlamydospore) 형성, 37℃에서의 성장 등의 표현형적 성상이 C. albicans와 매우 유사하여, 최근 칸디다 동정 방법의 발전에도 불구하고 여전히 그 분리빈도가 과소평가되었을 것으로 생각되고 있다[5]. C. dubliniensis의 빈도는 칸디다혈증에서 0.2~3%4, 보관된 효모균에서는 0.2~16.6%의 다양한 빈도로 보고되었으며 지속적으로 폐렴이나 뇌막염 등의 원인균으로 보고되고 있다[6],[7],[8]. 국내에서의 C. dubliniensis 분리빈도를 확인하기 위하여, 2004년에서 2005년 사이 국내 17개 병원에서 수집하여 보관 중인 효모균 1,596균주와[9] 2007년에서 2008년 국내 단일 기관의 호흡기 검체에서 분리된 효모균 434균주에서[10] C. dubliniensis를 검색하였으나 한 균주도 확인되지 않았다. 이후 2010년 칸디다혈증 환자의 혈액에서 C. dubliniensis가 원인균으로 분리되어 국내 최초로 보고되었다[11].
C. albicans와 C. dubliniensis의 감별 동정은 크게 표현형적 특성과 유전형적 특성을 이용한 방법으로 나누어 볼 수 있으며, 표현형적 특성에 의한 감별 동정법 중의 하나인 혈청학적 특성을 이용한 라텍스 응집(Latex agglutination, LA) 검사가 정확하고 신속하게 C. albicans와 C. dubliniensis를 구별하는 것으로 보고된 바 있다[12],[13],[14].
이에 본 연구에서는 국내에서 C. dubliniensis가 처음으로 분리된 기간 전후의 임상 검체에서 분리되어 보관 중인 C. albicans 균주를 대상으로, LA 검사를 이용하여 C. albicans로부터 C. dubliniensis를 감별하고 C. albicans로 동정된 균주에서의 C. dubliniensis 빈도를 확인하고자 하였다.
대상 및 방법
1. 대상 균주
2010년 1월부터 2011년 12월까지 중앙대학교병원을 내원한 환자들의 각종 임상 검체(소변 419검체, 혈액 61검체, 중심정맥 카테터 끝 6검체, 피부상처 6검체, 질 분비물 4검체, 기타 8검체)에서 분리되어 발아관 시험 또는 Vitek 2 ID-YST System (bioMerieux Vitek, Hazelwood, MO, USA)으로 동정 후 -70℃에 냉동 보관 중인 C. albicans 504균주, 1명의 칸디다혈증 환자의 혈액과 중심정맥 카테터 끝에서 연속적으로 분리된 C. dubliniensis 5균주, 그리고 8종류의 표준균주 10균주(C. albicans ATCC 18804, C. albicans ATCC 14053, C. dubliniensis ATCC MYA-646, C. dubliniensis KCTC-17427, C. glabrata ATCC 2001, Candida guilliermondii ATCC 6260, Candida krusei ATCC 6258, Candida lusitaniae ATCC 34449, C. parapsilosis ATCC 22019, C. tropi- calis ATCC 750)를 대상으로 하였다.
2. 방법
-70℃에 냉동 보관된 시험균주와 표준균주는 Sabouraud dextrose agar (SDA)에 계대 배양한 후 혈액한천배지와 SDA를 사용하여 35℃, 5% CO2 배양기에 2차 배양하였다. 혈액한천배지에서 자란 균주에서는 집락의 "spiking" 모양을 관찰하였고, SDA에서 자란 균주는 발아관 시험과 LA 검사에 사용하였다. 발아관 시험은 SDA에 자란 집락을 사람 혼주 혈청(human pooled serum)에 잘 풀어 37℃에 3시간 배양하여 현미경으로 발아관 형성을 관찰하였다. LA 검사는 Bichro-Dubli Fumouze® (Fumouze Diagnostics, Levallois-Perret, France) 키트를 사용하였으며, 제조사의 지침에 따라 20 μL의 라텍스 시약에 SDA에 자란 집락 2~3개를 잘 풀어준 후 3~5분 사이에 응집유무를 확인하였다. 발아관 시험에 의해 C. albicans로 예비 동정 후 보관하였던 균주의 칸디다 균종 동정은 Vitek 2 ID-YST System을 이용하여 제조사의 지침에 따라 시행하였다.
결 과
C. dubliniensis를 감별하기 위한 LA 검사는 8종류의 표준균주 10균주 중 C. dubliniensis 2균주(C. dubliniensis ATCC MYA-646와 KCTC-17427)에서만 양성을 보였고, 나머지 7종류의 표준균주 8균주 (C. albicans ATCC 18804, C. albicans ATCC 14053, C. glabrata ATCC 2001, Candida guilliermondii ATCC 6260, Candida krusei ATCC 6258, Candida lusitaniae ATCC 34449, C. parapsilosis ATCC 22019, C. tropi- calis ATCC 750)에서는 모두 음성이었다. 2010년 1월부터 2011년 12월까지 각종 임상 검체에서 분리되어 C. albicans로 동정된 후 -70℃에 냉동 보관된 504균주는 모두 LA 검사에서 음성이었고, 2010년 11월 1명의 환자에서 연속적으로 분리된 C. dubliniensis 5균주는 모두 LA 검사에서 양성이었다(Table 1). 그러므로 C. albicans로 동정되었던 504균주에서 C. dubliniensis는 한 균주도 없었다.
발아관 형성은 2종류의 표준균주(C. albicans와 C. dubliniensis) 모두에서 관찰되었고, 나머지 6종류의 표준균주에서는 관찰되지 않았다. 임상분리 균주에서는 C. albicans의 97.6%(492/504 균주)와 C. dubliniensis 5균주 모두 발아관 형성이 관찰되었다(Table 1).
혈액한천배지에서의 "spiking" 모양은 표준균주 중에서는 C. albicans 2균주에서만 관찰되었고 나머지 7종류의 표준균주에서는 관찰되지 않았으며, 임상분리 균주에서는 C. albicans의 84.7%(427/504 균주)에서만 관찰되었다(Table 1).
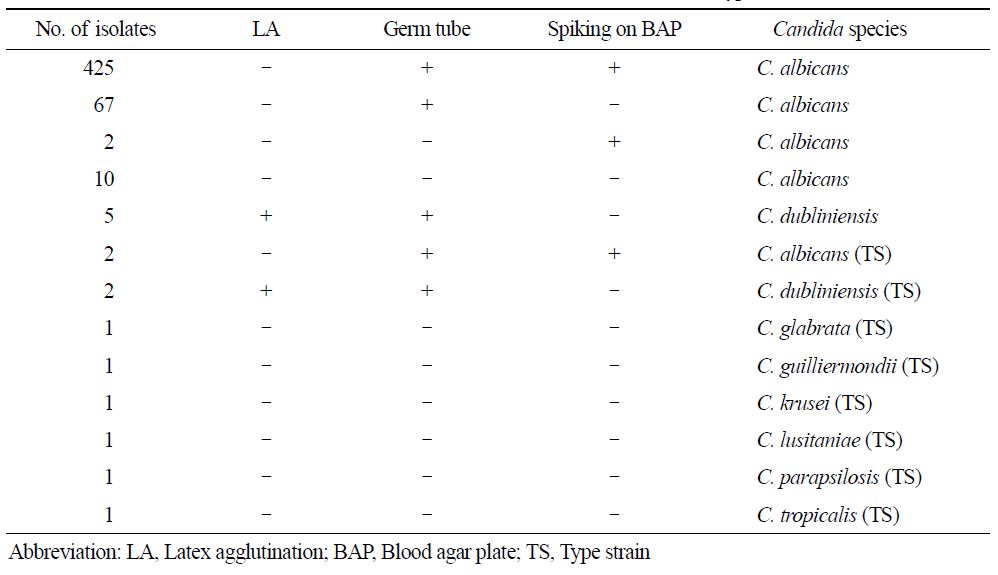
Table 1. Comparison
of results by "spiking" on blood agar plate,
germ tube and latex agglutination for 509 Candida clinical isolates (504
isolates of C. albicans and 5 isolates of C.
dubliniensis) and
10 type strains
고 찰
1995년 HIV 감염 환자의 구강에서 처음으로 분리되어 새로운 종인 C. dubliniensis로 명명된[3] 이후 보관되어 있던 효모균을 대상으로 한 연구에서, 객담에서 분리되어 1952년 C. albicans로 동정되었던 균주(네덜란드)와 1957년에 Candida stel- latoidea로 동정되었던 균주(영국)가 가장 오래된 C. dubliniensis로 확인되었다[6],[15]. C. dubliniensis는 주로 HIV 감염 환자의 구강에서 분리되었으나 HIV에 감염되지 않은 환자에서도 분리되고 있으며, 구강뿐 아니라 호흡기, 혈액, 중추신경계, 질, 소변, 대변 등의 다양한 검체에서도 지속적으로 분리되고 있고 가끔 치명적인 전신감염을 일으키기도 한다[6]. 또한 새의 배설물에 있던 진드기 표면에서도 C. dubliniensis가 분리되어 사람에 국한되지 않고 환경에 존재할 수 있음을 보여주었다[16]. C. dubliniensis의 분리빈도는 기저질환, 대상군, 검체종류, 검출 방법, 지역, 인종 등에 따라 매우 다양하게 보고되고 있다. 특히 C. dubliniensis는 HIV 감염 환자의 구강에서는 1.2~48%까지 보고된 반면 HIV 음성인 환자의 구강에서는 1.36~8.9%로 보고되었다[6]. 국내에서는 2010년 칸디다혈증의 원인균으로 C. dubliniensis가 분리되기[11] 이전, 국내 다 기관에서 수집된 효모균(1,596균주)과 단일 기관의 호흡기 검체에서 분리된 효모균(434균주)에서 C. dubliniensis가 검출되지 않았다[9],[10]. 국내에서 C. dubliniensis가 처음으로 분리된 기간 전후에 C. albicans로 동정되어 보관 중이던 임상균주를 대상으로 C. dubliniensis를 C. albicans로 잘못 동정했을 빈도를 확인하고자 LA 검사를 시행하였으나 이들 균주 중 C. dubliniensis는 동정되지 않았다. 이에 2010년 1월부터 2011년 12월까지 본 검사실의 임상 검체에서 분리된 칸디다 균주(2,497균주)에서의 C. dubliniensis 분리빈도는 대략 0.2% (5/2,497)로 추정할 수 있었고 여전히 국내 C. dubliniensis 빈도는 매우 낮을 것으로 생각되었다. 그러나 C. dubliniensis가 국내에서 2010년 11월 칸디다혈증의 원인균으로 확인되었고 전세계적으로 다양한 감염의 원인균으로 지속적으로 보고되고 있으므로, 다 기관의 다양한 검체에서 C. dublini- ensis 빈도에 대한 지속적인 조사가 필요할 것으로 생각되었다.
칸디다 균종 동정은 크게 표현형적 특성과 유전형적 특성을 이용한 방법으로 나누어 볼 수 있다. 표현형적 특성에 의한 칸디다 균종 동정은 발아관 시험, 비후막홀씨 생산 확인, 6.5% NaCl을 함유한 배지에서의 성장 확인, 온도에 따른 성장 확인, 발색배지를 사용하는 방법, 상품화된 동정 키트 사용, 혈청학적 특성을 이용한 LA 검사, 자동화 장비를 사용하는 방법 등이 있으며, 유전형적 특성을 이용한 방법으로는 중합효소연쇄반응, 제한절편길이다형성(restriction fragment length poly- morphism), 유전자 염기서열 분석 등의 방법이 있다[6],[12],[13],[17]. 또한, 최근 미생물의 단백질 성분을 분석하여 균종 동정을 할 수 있는 matrix-assisted laser desorption ionization time-of-flight mass spectrometry (MALDI-TOF MS)도 임상에서 분리되는 다양한 진균에 관한 데이터베이스를 계속 추가함으로 임상 검사실에서의 사용이 가능해지고 있다[17].
C. dubliniensis는 발아관 형성, 비후막홀씨 형성, 37℃에서의 성장 등 표현형적 성상이 C. albicans와 매우 유사하여, 발아관 형성과 같은 일부 표현형적 방법으로 동정할 경우 C. albicans로 동정될 수 있다[9],[11],[17]. 상품화된 키트나 자동화 장비를 사용하는 경우 C. dubliniensis와 C. albicans를 비교적 정확하게 감별할 수 있으나, 배양에 기초한 방법이므로 1~2일 정도의 시간이 소요되고 임상에서 분리되는 칸디다를 모두 동정하기에는 비용이 많이 들 수 있고, MALDI-TOF MS의 경우 정확하게 구별하는 것으로 보고되었지만[18] 고가의 장비가 필요하다. 따라서 C. albicans로부터 C. dublini- ensis를 감별하기 위한 방법으로 색 또는 형광을 내는 배지 사용, 온도에 따른 배양, 고장액에서의 성장 등을 사용하기도 하였으나, 낮은 특이도, 균주 보관에 따른 표현형적 특성의 변화, 또는 일반 검사실에서 일상적으로 사용하지 않는 배지를 사용하여야 하는 등의 문제점이 있었다[6],[9],[17],[19].
본 연구에서 사용된 LA 검사는 C. dubliniensis의 분아포자(blastoconidia) 표면에 있는 항원을 검출할 수 있는 단클론 항체(12F7-F2)가 부착된 입자를 사용한 상품화된 방법으로, C. dubliniensis와 C. albicans를 감별하는데 5분 이내에 결과 확인이 가능하고 SDA 배지에서 자란 균주로 검사할 경우 민감도와 특이도가 97.1~100%와 100%로 보고되었다12-14,19,20. 본 연구에서도 LA 검사는 3~5분에 결과 판독이 가능하였고, 8종류의 표준균주 10균주 중 C. dubliniensis 2균주에서만 양성이었고 C. albicans를 포함한 나머지 7종류의 표준균주에서는 모두 음성이었다. 또한 -70℃에 냉동 보관되었던 임상분리 균주 중 동일 환자에서 연속적으로 분리된 C. dubliniensis 5균주에서만 LA 검사 양성이었고 나머지 C. albicans로 최종 동정된 504균주는 모두 음성이었다. 그러므로 신속하고 간편하게 사용할 수 있는 LA 검사(Bichro-Dubli Fumouze®)는 다양한 칸디다 균주에서 C. dublini- ensis를 정확하게 감별할 수 있을 것으로 판단되었다.
또한 C. dubliniensis 표준균주 2균주와 임상분리 균주 5균주는 모두 발아관 형성이 관찰되었고 혈액한천배지에서의 "spiking"은 관찰되지 않았다. 그러나 이미 알려진 바와 같이 발아관 형성은 C. albicans에서도 양성이고 혈액한천배지에서의 "spiking"은 본 연구에 포함된 C. albicans의 15.3%(77/504 균주)에서 음성이었기 때문에, 발아관 형성과 혈액한천배지에서의 "spiking"은 C. albicans로부터 C. dubliniensis를 감별할 수 없었다.
결론적으로 본 연구에서는 2010년 1월부터 2011년 12월까지 국내 단일 기관의 임상 검체에서 분리되어 보관된 C. albicans 균주에서 C. dubliniensis가 없음을 확인하여 C. dubliniensis의 빈도는 매우 낮을 것으로 생각되었고, C. albicans로부터 C. dubliniensis를 감별하기 위한 LA 검사는 간편하고 신속하게 C. dubliniensis를 정확하게 감별할 수 있을 것으로 생각되었다.
Acknowledgements
이 논문은 2015년도 정부(교육부)의 재원으로 한국연구재단의 지원을 받아 수행된 기초연구사업임(NRF-2015R1D1A1A01058906).
Conflict of interest
In relation to this article, I declare that there is no conflict of interest.
References
1. Miceli MH, Diaz JA, Lee SA. Emerging oppor- tunistic yeast infections. Lancet Infect Dis 2011;11: 142-151
Crossref
Google Scholar
2. Guinea J. Global trends in the distribution of Candida species causing candidemia. Clin Microbiol Infect 2014;20 Suppl 6:5-10
Crossref
Google Scholar
3. Sullivan DJ, Westerneng TJ, Haynes KA, Bennett DE, Coleman DC. Candida dubliniensis sp. nov.: pheno- typic and molecular characterization of a novel species associated with oral candidosis in HIV-infected indi- viduals. Microbiology 1995;141:1507-521
Crossref
Google Scholar
4. Falagas ME, Roussos N, Vardakas KZ. Relative fre- quency of albicans and the various non-albicans Can- dida spp among candidemia isolates from inpatients in various parts of the world: a systematic review. Int Infect Dis 2010;14:e954-966
Crossref
Google Scholar
5. Khan Z, Ahmad S, Joseph L, Chandy R. Candida dubliniensis: an appraisal of its clinical significance as a bloodstream pathogen. PloS One 2012;7:e32952
Crossref
Google Scholar
6. Loreto ES, Scheid LA, Nogueira CW, Zeni G, Santurio JM, Alves SH. Candida dubliniensis: epidemiology and phenotypic methods for identification. Myco- pathologia 2010;169:431-443
Crossref
7. Yamahiro A, Lau KH, Peaper DR, Villanueva M. Meningitis caused by Candida dubliniensis in a patient with cirrhosis: A case report and review of the literature. Mycopathologia 2016;181:589-593
Crossref
Google Scholar
8. Petty LA, Gallan AJ, Detrick JA, Ridgway JP, Mueller J, Pisano J. Candida dubliniensis pneumonia: A case report and review of literature. Mycopathologia 2016; 181:765-768
Crossref
Google Scholar
9. Kim TH, Park BR, Kim HR, Lee MK. Candida dubliniensis screening using the germ tube test in clinical yeast isolates and prevalence of C. dubliniensis in Korea. J Clin Lab Anal 2010;24:145-148
Crossref
Google Scholar
10. Kim T-H, Yun SW, Lee M-K, Ro BI. Screening of Candida dubliniensis from respiratory samples in Korea. Korean J Med Mycol 2009;14:171-176
Crossref
Google Scholar
11. Yu N, Kim HR, Lee MK. The first Korean case of candidemia due to Candida dubliniensis. Ann Lab Med 2012;32:225-228
Google Scholar
12. Sahand IH, Moragues MD, Robert R, Quindos G, Ponton J. Evaluation of Bichro-Dubli Fumouze to distinguish Candida dubliniensis from Candida albi- cans. Diagn Microbiol Infect Dis 2006;55:165-167
Crossref
Google Scholar
13. Ahmad S, Khan Z, Asadzadeh M, Theyyathel A, Chandy R. Performance comparison of phenotypic and molecular methods for detection and differen- tiation of Candida albicans and Candida dubliniensis. BMC Infect Ds 2012;12:230.
Crossref
14. Marot-Leblond A, Beucher B, David S, Nail-Billaud S, Robert R. Development and evaluation of a rapid latex agglutination test using a monoclonal antibody to identify Candida dubliniensis colonies. J Clin Microbiol 2006;44:138-142
Crossref
Google Scholar
15. Meis JF, Ruhnke M, De Pauw BE, Odds FC, Siegert W, Verweij PE. Candida dubliniensis candidemia in patients with chemotherapy-induced neutropenia and bone marrow transplantation. Emerg Infect Dis 1999; 5:150-153
Crossref
Google Scholar
16. Nunn MA, Schaefer SM, Petrou MA, Brown JR. Environmental source of Candida dubliniensis. Emerg Infect Dis 2007;13:747-750
Google Scholar
17. Neppelenbroek KH, Seo RS, Urban VM, Silva S, Dovigo LN, Jorge JH, et al. Identification of Candida species in the clinical laboratory: a review of con- ventional, commercial, and molecular techniques. Oral Dis 2014;20:329-344
Google Scholar
18. Roberts AL, Alelew A, Iwen PC. Evaluation of matrix-assisted laser desorption ionization-time-of-flight mass spectrometry to differentiate between Candida albicans and Candida dubliniensis. Diagn Microbiol Infect Dis 2016;85:73-76
Crossref
19. Ells R, Kock JL, Pohl CH. Candida albicans or Candida dubliniensis? Mycoses 2011;54:1-16
Crossref
Google Scholar
20. Chryssanthou E, Fernandez V, Petrini B. Performance of commercial latex agglutination tests for the differ- entiation of Candida dubliniensis and Candida albi- cans in routine diagnostics. APMIS 2007;115:1281 -1284
Google Scholar
