pISSN : 3058-423X eISSN: 3058-4302
Open Access, Peer-reviewed
pISSN : 3058-423X eISSN: 3058-4302
Open Access, Peer-reviewed
Jeong Nan Kang,Do Hyeong Kim,So Hee Park,Jung Eun Seol,Hyojin Kim,Jeong Hwan Shin
http://dx.doi.org/10.17966/KJMM.2016.21.4.122 Epub 2016 December 27
Abstract
A 71-year-old female presented with erythematous ulcerative patches on her right cheek, chest and right upper arm. She admitted to neurosurgery intensive care unit (NSICU) with mental change related to intracerebral hemorrhage. She had no underlying disease. Histopathologic examination of her right upper arm showed multiple non-septated broad hyphae with right-angled branching in dermis. She was diagnosed as primary cutaneous mucormycosis. The fungal culture demonstrated Cunninghamella species. We postulated that mucormycosis occurred after inoculation of fungi following fall down trauma. Mucormycosis, which commonly affects immunocompromised patient, is a rare fungal infection caused by the order Mucorales. Cutaneous mucormycosis is caused either by direct inoculation of fungal spores or by hematologic spread from another primary source. Clinical manifestations are various from indolent ulceration to rapidly progressive necrosis. Mucormycosis can be diagnosed based on the histologic findings and the fungal culture. Mucormycosis by Cunninghamella species have been increasingly reported, but most of them are pulmonary mucormycosis in immunocompromised patients. Herein, we report a rare case of multiple primary cutaneous mucormycosis caused by Cunninghamella species in a patient without underlying disease.
Keywords
서 론
털진균증은 Mucorales 목에 의한 드문 진균 감염증으로, 특히 조절되지 않는 당뇨병, 장기이식자, 혈액암 환자 등 면역저하자에서 호발한다[1]. 혈관침범으로 연부조직 파괴와 급속한 진행을 보이는 것이 특징이며, 이 중 원발성 피부털진균증은 털진균증의 드문 형태로, 일반적인 양상으로는 진균 포자의 접종 이후로 발생하는 단발성의 괴사성 출혈 궤양을 보인다[1].
Cunninghamella 속 진균에 의한 털진균증은 드물게 보고되며, 이 중 대부분은 폐 털진균증으로 원발성 피부털진균증은 매우 드물다. Cunninghamella속 진균에 의한 원발성 피부털진균증은 현재까지 총 4례[2],[3],[4],[5] 보고되어 있으며 이는 모두 면역저하자에서 발생한 증례이다. 저자들은 기저질환이 없는 71세 환자에서 Cunninghamella 속에 의해 우측 볼, 흉부 및 우측 팔에 다발성으로 발생한 원발성 피부털진균증 1예를 경험하고, 이를 드문 증례로 생각하여 문헌고찰과 함께 보고하는 바이다.
증 례
환 자: 전 OO, 71세, 여자
주 소: 우측 볼, 흉부 및 우측 팔에 발생한 홍반 궤양성 반
현병력: 환자는 내원 2주 전 의식을 잃고 쓰러진 상태로 발견되어 본원 응급실 통해 내원하였으며, 두개내 출혈 진단 하에 신경외과적인 응급 수술 시행받고 의식불명 상태로 신경외과 중환자실 입원중이었다. 피부 병변은 입원 10일째에 협진 의뢰되었고 정확한 발병시기는 알지 못하였다.
과거력: 특이사항 없음
가족력: 특이사항 없음
이학적 소견: 피부 소견 외에 우측 허벅지에 찰과상이 관찰되었다.
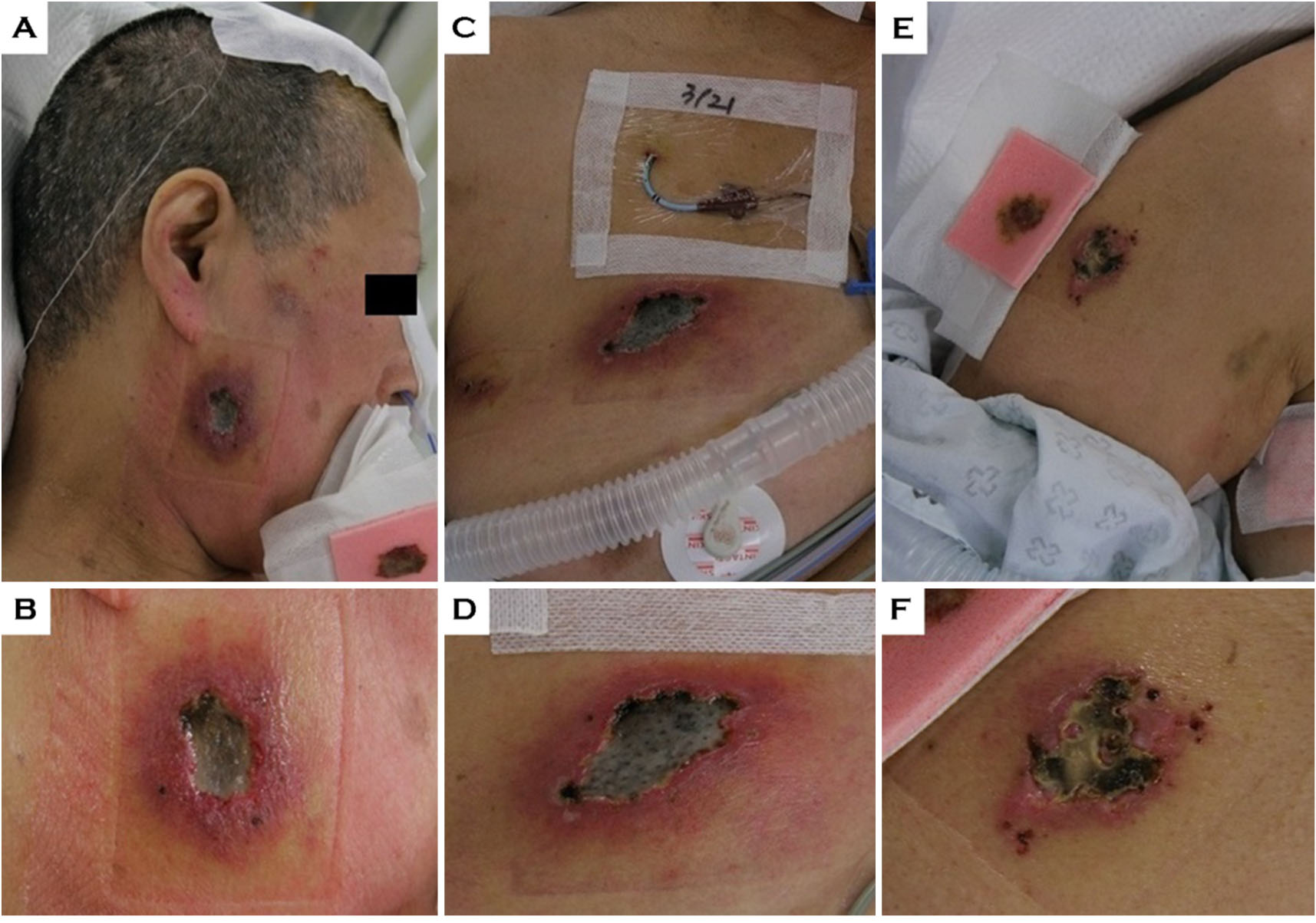
피부 소견: 우측 볼, 흉부 및 우측 팔에 홍반 궤양성 반이 관찰되었고 괴사딱지가 동반되었다(Fig. 1). 동측 엉덩이와 허벅지에 찰과상이 관찰된다는 점에서 낙상이 있었을 것으로 추정할 수 있었다.
검사 소견: 혈액검사 상 호중구(12,591/mm3)의 중등도 증가, C-reactive protein (4.99 mg/dL) 및 erythrocyte sedimentation rate (57 mm/hr)의 증가가 관찰되었고, 간 및 신기능 검사, 혈당검사에서는 정상범위를 보였다. 혈액배양검사에서는 Acinetobacter baumanii가 배양되었고, 경기관흡인 배양검사에서는 Serratia marcescens가 배양되었다. 뇌척수액 성상분석은 정상 소견을 보였고, 뇌척수액 배양검사에서 세균도 관찰되지 않았다. 소변검사에서는 모두 정상 소견을 보였다.
방사선학적 소견: 흉부 X선 검사에서는 특이소견 관찰되지 않았고, 두개 CT 사진에서는 체외뇌실배액술이 시행된 상태로, 좌측 기저핵과 좌측 시상에 뇌내 출혈과 뇌실내 출혈이 관찰되었다. 입원 당시 시행한 고해상도 흉부 CT에서는우상엽 폐에 다수의 중심소엽 결절과 양측 폐의 미만성 기관지벽 비후 소견이 관찰되었다.
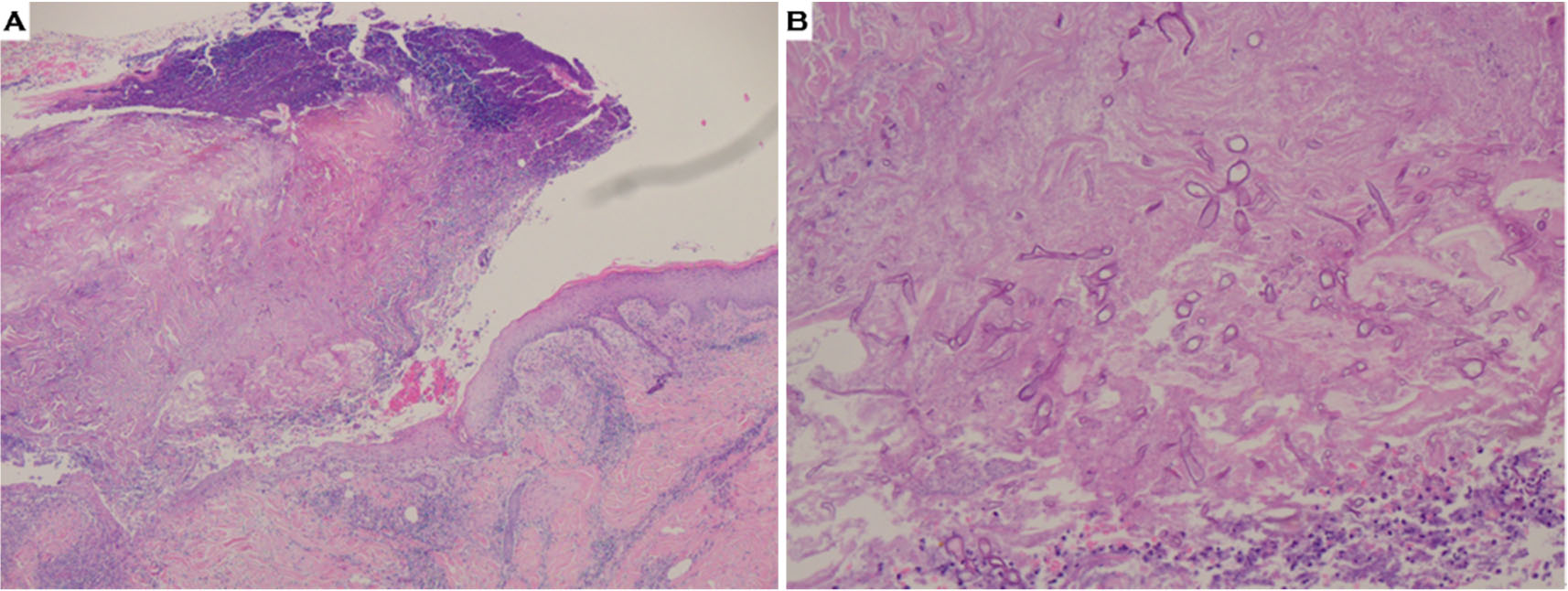
병리조직학적 소견: 우측 팔 병변에서 시행한 조직검사 상 H&E 염색에서 표피로 궤양, 딱지, 표피내 미세농양 및 출혈 소견이 관찰되었다. 진피 내에서는 전층에 걸쳐 광범위하게 침윤된 호중구, 조직구 및 다핵거대세포로 구성된 육아종성 염증반응이 관찰되고, 90도의 분지를 보이며 얇은 벽을 가지는 균사가 다수 관찰되었다(Fig. 2).
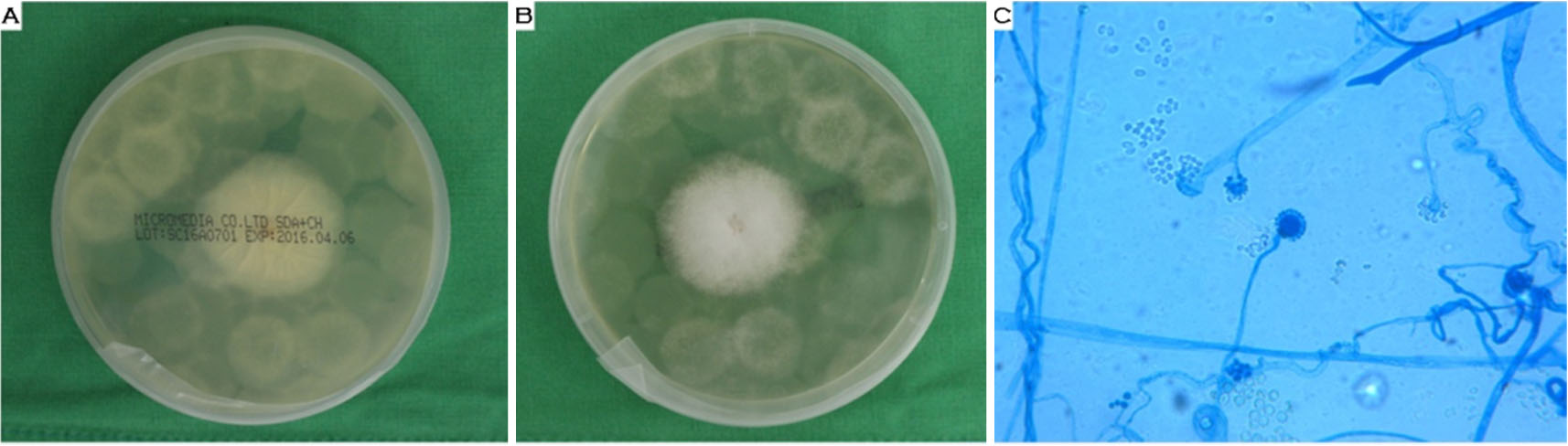
진균학적 소견: 우측 팔 병변 피부 생검조직을 25℃에서 Sabourauds dextrose agar에 배양한 결과 배양 5일 째 빠르게 성장하는 흰색의 솜털 모양 집락이 배지 표면을 뒤덮는 소견을 보였으며, 배지의 뒷면은 황색을 띠었다(Fig. 3A, 3B). 집락 일부를 채취하여 lactophenol cotton blue 염색을 통해 현미경으로 관찰한 결과 곧은 분지형의 포자낭병 (sporangiophore)이 관찰되고 말단부가 부푼 작은 이(denticle) 모양의 잔물집(terminal vesicle)을 보였다. 이 부위에서 난원형의 단세포의 포자낭 포자(sporangiospore)가 다수 발달되어 있었다(Fig. 3C).
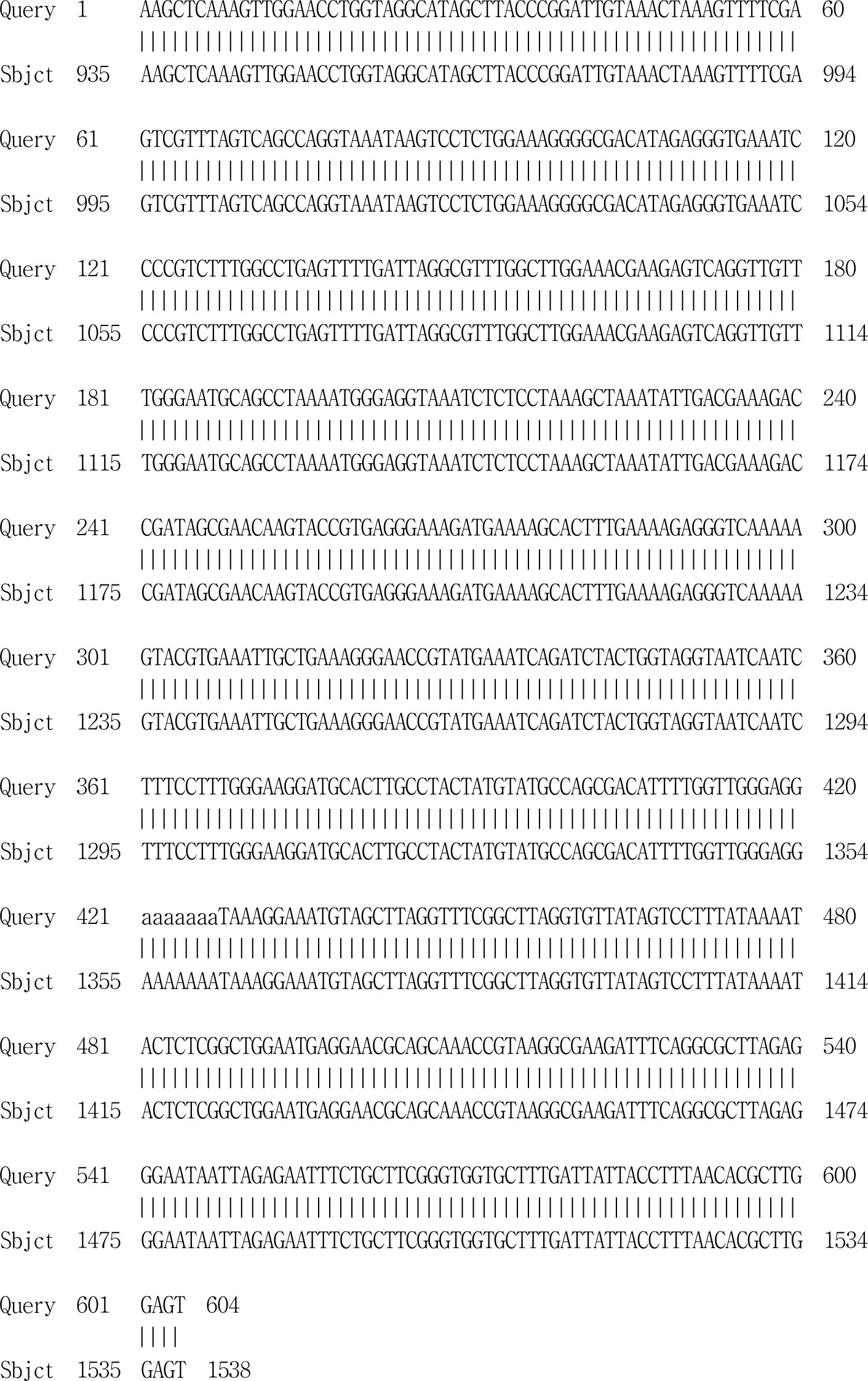
분자생물학적 검사: 배양된 균집락으로부터 DNeasy® Plant Mini Kit (Qiagen)를 이용하여 균 DNA를 분리하였다. 분리된 DNA는 D1 (F) (5'-GCATATCAATAAGCGGAGGAAAAG-3'), D2 (R) (5'-GGTCCGTGTTTCAAGACGG-3') primer를 사용하여 28S rRNA gene을 증폭한 후 ABI PRISM® 3130 Genetic Analyzer (Life Technologies)를 이용하여 얻어진 염기서열을 NCBI BLAST에서 Cunninghamella (C.) bertholletiae, C. elegans의 염기서열과 비교한 결과 두 가지 모두와 100% 일치하여 Cunninghamella 속으로 동정되었다(Fig. 4).
치료 및 경과: 피부털진균증으로 확진된 후 괴사조직제거술과 함께 amphotericin B를 매일 50 mg 정맥 내로 주사하였으며 피부 병변 호전되던 중 신경외과적인 보존적 치료를 위해 타병원으로 전원되었다.
고 찰
털진균증은 Mucorales 목에 속한 진균에 의한 드문 혈관 침습성(angioinvasive) 감염증이다[6]. 임상형에 따라 비뇌형, 호흡기형, 파종형, 피부형, 위장관형으로 구분할 수 있으며, 5가지 모두 면역저하자에게 더 흔하다고 보고되어 있다[7],[8]. 이 중 피부털진균증은 전체의 10% 미만을 차지하는 드문 아형으로, 피부에 직접적으로 진균 포자의 접종으로 발생하거나, 다른 일차병소, 특히 폐로부터 혈행성 전파를 통해 감염이 발생한다[9]. 원발성 피부털진균증은 피부 외상력이 선행하는 경우가 많으며, 그 외에도 화상, 수술, 수술부목, 혈관 및 근육주사, 조직검사, 문신, 곤충물림, 과도한 발한,
부착밴드 등이 모두 유발사건이 될 수 있다[7],[10]. 공통 분모는 피부 보호장벽의 손상이 일어나는 것이며, 잇따라 일어나는 진균 포자의 접종으로 원발성 피부털진균증이 발생하게 된다[7]. 한 문헌에서는 피부털진균증 증례의 선행요인으로 34%에서 관통상이 있었고, 드레싱 15%, 수술 15%, 화상 6%, 자동차 사고와 낙상이 각각 3%였다고 보고하고 있다[11]. 피부털진균증의 전신 위험요인으로는 당뇨병, 악성종양, 백혈구감소증, 면역억제제 복용을 들 수 있으며[12], 일부 문헌에서는 원발성 피부털진균증 환자의 50%가 당뇨병을 가지고 있다고 언급한다[13]. 본 증례는 기저질환이 없는 환자에서 낙상으로 인해 다수의 외상 부위에 피부 병변이 발생한 것으로 추정된다.
원발성 피부털진균증은 표재형 또는 괴사형의 임상양상을 보일 수 있다[14]. 이 중 표재형 감염증은 점진적인 발병과 느린 진행을 보이는 것이 특징으로, 조직검사에서 심부조직 혹은 혈관 침습이 관찰되지 않고 발열 등의 전신증상을 보이지 않는다[7]. 피부 병변은 고름물집(pustules)으로 관찰되며 궤양이나 가피 형성은 드물다[3]. 대부분 무통성이며, 치료는 항진균제의 전신투여 없이 국소적인 괴사조직제거술로 충분한 경우가 많다[7].
괴사형 감염증은 빠른 발병과 급속한 진행이 특징적이다. 유발사건 48~72시간 후 홍반성 반이 나타나며[8], 다수의 홍반성 반이 빠르게 융합하면서 궤양과 가피를 형성하며 통증이 발생한다[7]. 병변은 계속해서 넓어지며, 하부 피부 구조물의 경화를 유발한다[7]. 혈관 침습과 그에 따른 조직 괴사가 산성의 조직환경을 만들고, 이것이 진균의 성장에 도움을 주는 이른바 자기증식(selfpropagating)의 특징을 보이며, 혈관 침습성으로 인해 혈행성 전파가 발생하는 경우도 있다[7]. 괴사형은 초기에 진균 감염증을 의심하지 못하는 경우 진단이 지체되어 사망하는 경우가 많아 조기 진단이 필수적이며, 적극적인 수술적 치료와 전신 항진균 치료가 모든 경우에서 시행되어야 한다[7],[8],[15]. 본 증례는 궤양을 동반한 직경 5 cm 이상의 홍반성 반이 보였으며, 염증세포 침윤이 진피 전층에 걸쳐 있었다는 점에서 괴사형임을 알 수 있었다.
진단을 위해서는 조직검사가 필수적이며, 균종동정을 위해서는 진균 배양이 필요하다[7],[16]. 조직검사에서 폭이 넓고 격막이 없으며, 직각으로 분지하는 특징적인 균사를 볼 수 있다[7],[16]. KOH 젖은 펴바른 표본검사가 진단에 도움이 될 수 있지만, 가피나 궤양 병변에는 적용이 힘들다[7]. 본 증례에서도 KOH 젖은 펴바른 표본검사 시행이 곤란하여 조직검사와 진균 배양을 시행하였으며, 조직검사에서 특징적인 균사체를 관찰할 수 있었고 진균 배양에서 Cunninghamella (C.) 속 진균임을 동정할 수 있었다.
Cunninghamella 속 진균 중에서 현재까지 C.bertholletiae만이 사람에게 감염성을 가진다고 알려져 있다[17]. Cunninghamella 속에 의한 털진균증은 드물게 보고되며, 증례 대부분이 폐 털진균증(pulmonary mucormycosis)으로 면역저하자에서 발생한다. 현재까지 Cunninghamella 속에 의한 원발 성 피부털진균증은 해외문헌에서는 4례[2],[3],[4],[5]가 보고 되었으나 국내문헌에는 보고가 없다. Cunninghamella 속에 의한 이전 보고들은 각각 당뇨병 환자, 후천성면역결핍증후군 환자, 신장이식환자, 당뇨병 및 만성 골수성 백혈병 환자로 모두 면역저하자에게 발생하였으나 본 증례는 면역억제제 등의 복용력이 없고 특이 기저질환이 없다는 점에서 차이점을 보였다. 이에 저자들은 기저질환이 없는환자에서 Cunninghamella 속 진균에 의해 발생한 다발성 원발성 피부털진균증을 경험하고 드문 증례로 생각되어 보고한다.
Conflict of interest
In relation to this article, I declare that there is no conflict of interest.
References
1. Chambers CJ, Reyes Merin M, Fung MA, Huntley A, Sharon VR. Primary cutaneous mucormycosis at sites of insulin injection. J Am Acad Dermatol 2011;64: e79-81
2. Boyce JM, Lawson LA, Lockwood WR, Hughes JL. Cunninghamella bertholletiae wound infection of probable nosocomial origin. South Med J 1981;74: 1132-1135
Google Scholar
3. Mostaza JM, Barbado FJ, Fernandez-Martin J, Pena- Yanez J, Vazquez-Rodriguez JJ. Cutaneoarticular mucormycosis due to Cunninghamella bertholletiae in a patient with AIDS. Rev Infect Dis 1989;11:316 -318
Crossref
Google Scholar
4. Motohashi K, Ito S, Hagihara M, Maruta A, Ishigatsubo Y, Kanamori H. Cutaneous zygomycosis caused by Cunninghamella bertholletiae in a patient with chronic myelogenous leukemia in blast crisis. Am J Hematol 2009;84:447-448
Crossref
Google Scholar
5. Quinio D, Karam A, Leroy JP, Moal MC, Bourbigot B, Masure O, et al. Zygomycosis caused by Cunninghamella bertholletiae in a kidney transplant recipient. Med Mycol 2004;42:177-180
Crossref
Google Scholar
6. Prabhu RM, Patel R. Mucormycosis and entomophthoramycosis: a review of the clinical manifestations, diagnosis and treatment. Clin Microbiol Infect 2004; 10 Suppl 1:31-47
Crossref
Google Scholar
7. Hicks WL, Jr., Nowels K, Troxel J. Primary cutaneous mucormycosis. Am J Otolaryngol 1995;16:265-268
8. Khardori N, Hayat S, Rolston K, Bodey GP. Cutaneous Rhizopus and Aspergillus infections in five patients with cancer. Arch Dermatol 1989;125:952-956
Crossref
Google Scholar
9. Verma R, Nair V, Vasudevan B, Vijendran P, Behera V, Neema S. Rare case of primary cutaneous mucormycosis of the hand caused by Rhizopus microsporus in an immunocompetent patient. Int J Dermatol 2014; 53:66-69
Crossref
Google Scholar
10. Kaur R, Bala K, Ahuja RB, Srivastav P, Bansal U. Primary cutaneous mucormycosis in a patient with burn wounds due to Lichtheimia ramosa. Mycopathologia 2014;178:291-295
Crossref
Google Scholar
11. Roden MM, Zaoutis TE, Buchanan WL, Knudsen TA, Sarkisova TA, Schaufele RL, et al. Epidemiology and outcome of zygomycosis: a review of 929 reported cases. Clin Infect Dis 2005;41:634-653
Crossref
Google Scholar
12. Almaslamani M, Taj-Aldeen SJ, Garcia-Hermoso D, Dannaoui E, Alsoub H, Alkhal A. An increasing trend of cutaneous zygomycosis caused by Mycocladus corymbifer (formerly Absidia corymbifera): report of two cases and review of primary cutaneous Mycocladus infections. Med Mycol 2009;47:532-538
Google Scholar
13. Adam RD, Hunter G, Ditomasso J, Comerci G, Jr. Mucormycosis: emerging prominence of cutaneous infections. Clin Infect Dis 1994;19:67-76
Crossref
Google Scholar
14. Ryan ME, Ochs D, Ochs J. Primary cutaneous mucormycosis: superficial and gangrenous infections. Pediatr Infect Dis 1982;1:110-114
15. Aziz S, Merrell RC, Edwards MF. Mucormycosis in patients with multiple-organ failure. Arch Surg 1984; 119:1189-1191
Crossref
Google Scholar
16. Flagothier C, Arrese JE, Quatresooz P, Pierard GE. Cutaneous mucormycosis. J Mycol Med 2006;16:77 -81
Crossref
Google Scholar
17. Ribes JA, Vanover-Sams CL, Baker DJ. Zygomycetes in human disease. Clin Microbiol Rev 2000;13:236 -301
Crossref
Google Scholar
