pISSN : 3058-423X eISSN: 3058-4302
Open Access, Peer-reviewed
pISSN : 3058-423X eISSN: 3058-4302
Open Access, Peer-reviewed
Sang Youl Yun,Min Woo Park,Moo Kyu Suh,Gyoung Yim Ha,Jong Im Lee,Jong Soo Choi
http://dx.doi.org/10.17966/KJMM.2016.21.3.92 Epub 2016 October 03
Abstract
Kerion celsi is a severe inflammatory type of tinea capitis that presents as a boggy mass studded with broken hairs, oozing purulent material from follicular orifices. This infection is caused most commonly by zoophilic or geophilic pathogens. Trichophyton(T.) rubrum is an anthropophilic dermatophyte that is found all over the world. It has become one of the most important causative agents in tinea unguium and tinea pedis. But, kerion celsi caused by T. rubrum is rare. Kerion celsi is uncommon in adult. We report a case of kerion celsi caused by T. rubrum in a 72-year-old woman. She presented with localized tender erythematous plaques with pustules with oozing purulent material on the frontal scalp. A fungal culture from tissue of the lesions was grown on Sabouraud's dextrose agar and showed typical whitish cottony colonies of T. rubrum. The nucleotide sequence of internal transcribed spacer region for clinical isolate was identical to that of T. rubrum strain UZ1588_14 (GenBank accession number KP326579.1). She was treated with 200 mg of oral itraconazole daily for 3 months. The skin lesions improved 1 month after treatment, and recurrence has not been observed.
Keywords
Elderly Kerion celsi Trichophyton rubrum
서 론
백선종창(kerion celsi)은 피부사상균이 모발을 침범하여 발생되는 머리백선(tinea capitis)의 심한 형태로 염증을 유발하여 두피에 동통을 동반한 농종을 형성하는 질환이며, 주로 소아에서 흔히 발생하며 성인에서는 비교적 드물게 발생한다. 원인균은 주로 동물친화성 및 토양친화성 피부사상균으로 Microsporum(M.) canis, M. gypseum, Trichophyton(T.) verrucosum 등이 있다[1]. T. rubrum은 머리를 제외한 백선 중에서 가장 많은 원인균중의 하나이나 머리백선을 일으키는 예는 비교적드문 것으로 보고되고 있다[2],[3],[4],[5].
저자들은 백선종창이 72세 된 노인에서 T. rubrum에 의해 발생한 예를 경험하고 드문 예라 생각되어 문헌고찰과 함께 보고한다.

증 례
환 자: 조 OO, 72세, 여자
주 소: 전두부 두피의 압통을 동반한 농포와 홍반성 판
현병력: 내원 6개월 전부터 전두부에 압통을 동반한 홍반성 판과 염증성 농포가 발생한 후 점차 크기가 증가하여 본원 피부과 내원하였음
과거력 및 가족력: 특기사항 없음
이학적 소견: 피부 소견 외 특기사항 없음
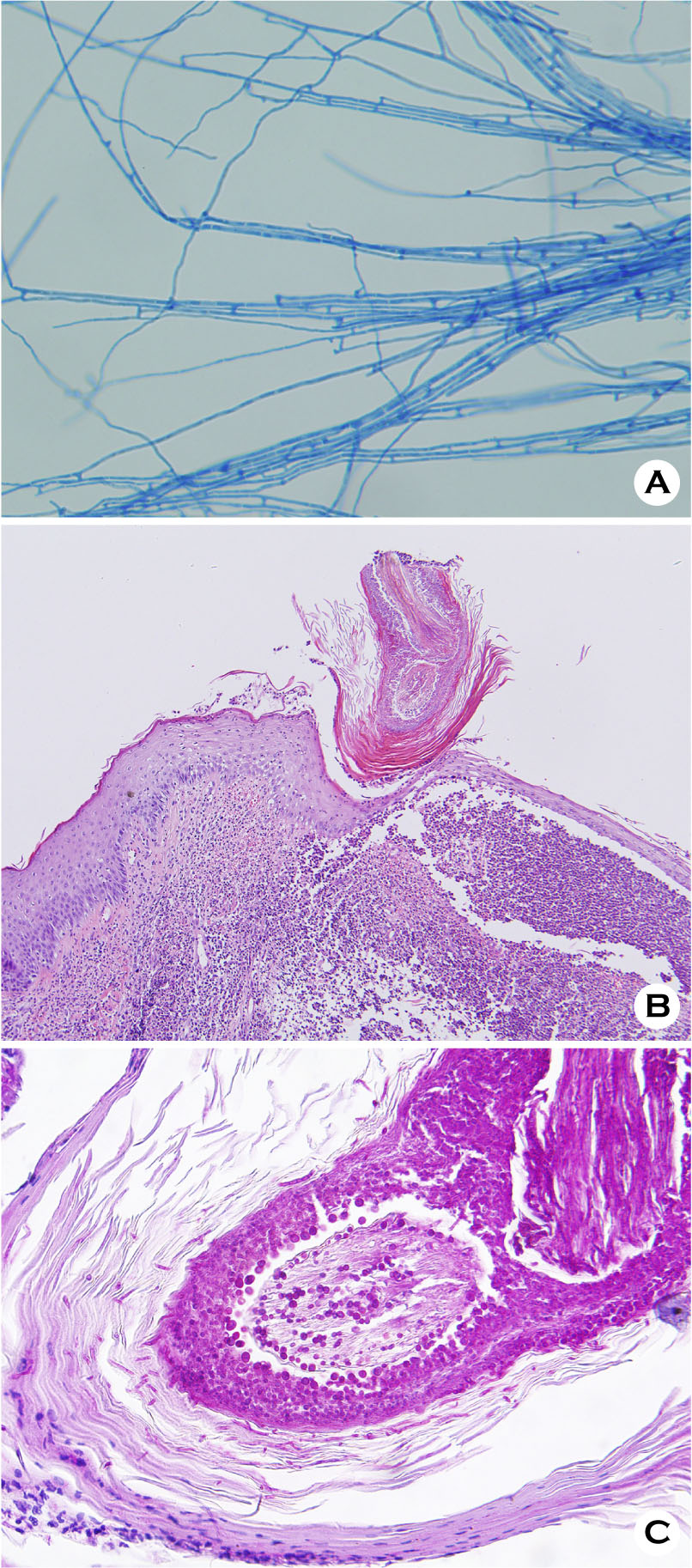
피부 소견: 전두부에 압통을 동반한 홍반성 판과 염증성 농포가 관찰되었고 병변 내의 모발은 쉽게 탈락되었음(Fig. 1A, 1B).
진균학적 소견: 전두부 두피의 병모 및 인설의 KOH 검사상 균사가 관찰되었으나 Wood 등 검사는 음성이었다. 두피 병소 부위의 인설 및 병모를 Sabouraud's dextrose agar에 접종하여 25℃에서 2주간 배양한 결과 융기된 솜털 모양의 균집락을 관찰할 수 있었으며 배지의 뒷면은 검붉은 색을 나타내었다(Fig. 2). 또한 이 집락을 슬라이드 배양표본으로 만들어 lactophenol-cotton blue로 염색하여 현미경으로 관찰한 결과 눈물방울 모양의 소생분자가 관찰되어 T. rubrum으로 동정하였다(Fig. 3A).
검사 소견: 일반혈액검사, 소변검사, 간기능 및 신기능 검사와 매독혈청반응 검사, 흉부 X-선 검사, 심전도 검사는 모두 정상 범위 내지 음성이었다.
병리조직학적 소견: 전두부의 병변부에서 시행한 피부생검의 H & E 염색 상 모낭 주위 및 진피층으로 림프구, 조직구 등으로 구성된 염증세포의 침윤이 관찰되었다(Fig. 3B). Periodic acid-Schiff 염색 상 모낭 주위에서 붉은 균사와 분생자가 관찰되었다(Fig. 3C).
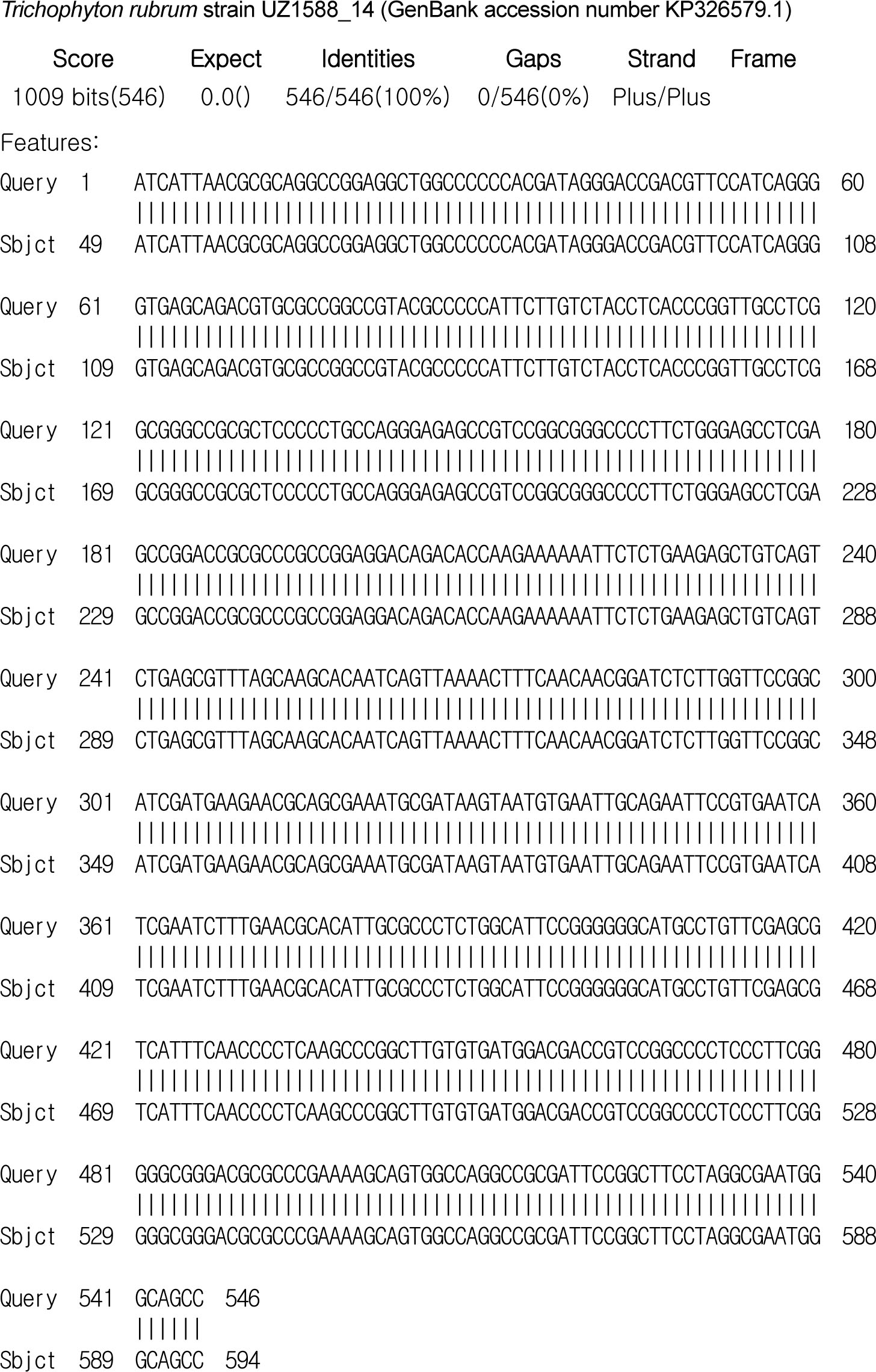
분자생물학적 검사: 환자의 배양된 균집락으로부터 DNA를 분리하여 진균핵 내의 internal tran-scribed spacer (ITS) 부위의 염기서열을 얻은 후 BLAST를 이용하여 GenBank에 있는 T. rubrum strain UZ1588_14 (GenBank accession number KP-326579.1)의 ITS 부위의 염기서열과 비교한 결과 100% 일치하여 T. rubrum으로 동정하였다(Fig. 4).
치료 및 경과: 1일 itraconazole 200 mg을 경구 투여하고 sertaconazole의 국소도포로 치료를 시작하였다. 치료 시작 1개월 째 병변부 염증의 현저한 호전을 보였다. 이후 2개월간 치료를 지속하여 탈모를 포함한 모든 증상이 호전되었으며 이후 6개월 동안 외래 추적관찰 하였으나 재발 소견은 없었다.

고 찰
백선종창은 M. canis, M. gypseum, T. verrucosum등 동물친화성 및 토양친화성 진균에 의해 발생하는 염증성 머리백선으로 지역에 따라 주 원인균의 차이가 있다[1]. 국내에서는 최근 M. canis가 주 원인균으로 알려져 있으나[2],[3],[4],[6], 1986년 Kim 등[7] 이 T. verrucosum에 의한 백선종창을 처음으로 보고한 이후에 점차 그 보고가 증가하고 있다. 이외에도 T. violaceum, T. tonsurans, T. mentagrophytes가 국내에서도 보고되었다[2],[3],[4],[8]. T. rubrum은 사람 친화성 진균으로 세계적으로 광범위하게 분포하고 있으며, 머리백선 이외의 몸백선, 샅백선, 손백선, 발백선, 손발톱백선과 같은 다른 표재성 진균감염의 가장 흔한 원인균 중 하나이다. 그러나 T.rubrum이 머리백선의 원인으로 보고되는 경우는 전 세계적으로 일부 지역을 제외하면 매우 드물며[5],[9],[10], T. rubrum에 의한 백선종창도 국내 피부과 문헌에서는 Kim 등[11]이 처음 1예를 처음 보고한 이후 드물게 보고되고 있다[2],[3],[4],[12],[13],[14],[15]. 이처럼 신체의 한정된 부위와 지리적인 편재를 보이는 이유는 유전학적, 환경적 요인이 작용할 것으로 추측되지만 확실히 밝혀져 있지 않다[16].
백선종창은 사춘기 이후 연령에서는 잘 발생하지 않는 것으로 알려져 있다. 사춘기 이후에는 피지 분비의 양적인 증가 및 질적인 변화에 의해 항진균 효과를 갖는 두부 지방산의 정균 작용이 활성화되는 것이 주요한 요인으로 생각되며, 또한 사춘기 이전에는 미숙했던 면역학적 체계가 사춘기를 지나면서 완성되는 것도 원인이 될 수 있다고 한다 [17]. 최근에는 스테로이드 제제의 오남용, 당뇨, 면역억제제의 투여 등으로 성인에서 백선종창의 발생빈도가 증가추세에 있다고는 하나 여전히 사춘기 이전의 소아에서 발생빈도가 높게 보고된다[2],[3],[4]. 성인에서는 면역기능이 억제되어 있거나 피지 분비가 감소하는 폐경기 이후의 여성들이 주로 보고되어 왔다[17],[18],[19]. 본 증례에서도 72세 여성으로 스테로이드 제제 장기복용이나 면역억제제 투여 등의 과거력은 없었으나 폐경기에 따른 체내 호르몬 대사 영향으로 머리 지방산의 분비 저하가 유발 요인일 것으로 생각된다.
진단은 병변부의 KOH 검사와 진균 배양으로 이루어지며 조직생검상 모발 주머니 주위의 심한 염증세포 침윤과 모발줄기 주위의 균사를 관찰할 수 있다. T. rubrum은 배양 배지의 자홍색 또는 포도주 빛의 착색을 보일 수 있으며, 현미경 검사상 균사가 풍부하며 작은 눈물방울 모양 내지는 쐐기 모양의 소생분자가 균사의 양 옆으로 배열되는 특징을 보인다[1]. 본 증례에서는 병변부에서 시행한 KOH 검사에서 균사가 관찰되었으며 사부로배지에서 2주간 실온 배양했을 때 융기된 솜털모양의 균집락이 보였고, 이 집락을 슬라이드 배양표본으로 만들어 현미경으로 관찰하면 눈물방울 모양의 소생분자가 관찰되었다. 본 증례에서는 병리조직 검사상 H&E 및 PAS 염색으로 모간 주위에서 균사와 포자를 잘 볼 수 있었다. 전통적으로 원인균의 동정은 형태학적 특성을 기반으로하여 이루어졌으나 이는 많은 시간이 소요되며 정확한 동정은 형태학적 특성을 기반으로 하여 이루어졌으나 이는 많은 시간이 소요되며 정확한 동정을 위해서 숙련된 전문가가 필요하다. 이에 비해 분자생물학적 동정은 소요시간이 적으며 정확도가 높아 진균 동정에 도움을 주고 있다[20]. 본증례에서는 환자의 배양된 균집락으로부터 DNA를 분리하여 진균핵 내의 internal transcribed spacer (ITS) 부위의 염기서열을 얻은 후 BLAST를 이용하여 GenBank에 있는 T. rubrum stain UZ1588_14 (GenBank accession number KP326579.1)의 ITS 부위의 염기서열과 비교한 결과 100% 일치하여 T. rubrum으로 최종 동정하였다.
본 증이 발생하였을 경우 감별해야 할 질환으로는 절종증, 농가진, 탈모성모낭염증이 있으며, 반흔을 남긴 뒤에는 원판상홍반성루푸스, 모공성 편평태선, 가성원형탈모증, 방사선피부염 등과도 감별이 필요하다[1]. 본 증은 임상적으로 모발이 쉽게 탈락되는 점과 KOH 검사와 진균 배양으로 상기질환들과 감별할 수 있었다.
치료로는 항진균제의 경구복용과 함께 염증반응에 의한 반흔이나 영구 탈모를 줄이기 위해 코르티코스테로이드호르몬과 항생제를 같이 투여하기도 한다[1]. 항진균제로 griseofulvin이 주로 사용 되었으나 최근에는 부작용이 적고 저항균주의 발생을 줄일 수 있는 itraconazole과 terbinafine 등이 이용되고 있다[1]. 본 증례는 itraconazole 200 mg을 3개월 투여하였다. 치료시작 1달 째 병변부의 염증과 통증의 현저한 호전을 보였다. 이후 2개월간 치료를 지속하여 탈모를 포함한 모든 증상이 호전되었으며 이후 6개월 동안 외래 추적관찰 하였으나 재발 소견은 없었다.
Conflict of interest
In relation to this article, I declare that there is no conflict of interest.
References
1. Stefan MS, Amit G. Superficial fungal infection. In: Goldsmith LA, Katz SI, Gilchrest BA, Paller AS, Leffell DJ, Dallas NA, editors. Fitzpatrick's Dermatology in General Medicine. 8th ed. New York: McGraw-Hill, 2012:2277-2297
2. Oh SH, Kim SH, Suh SB. Tinea capitis of adults in Daegu city for 11 years (1978-1988). Korean J Dermatol 1989;27:666-679
Google Scholar
3. Chun IK, Lim MH, Lee SC, Won YH. Clinical and mycological studies of tinea capitis in Chonnam area (1986-1995). Korean J Med Mycol 1996;1:83-89
Google Scholar
4. Shin DH, Kim KS, Kim KH. Clinical and mycologic studies of tinea capitis in Taegu. Korean J Med Mycol 1988;3:132-138
Google Scholar
5. Anstey A, Lucke TW, Philpot C. Tinea capitis caused by Trichophyton rubrum. Br J Dermatol 1996;135: 113-115
Crossref
Google Scholar
6. Kim SH, Suh MK, Kim JH, Ha KY, Kim JR. A case of kerion celsi caused by Microsporum canis probably transmitted from hamster. Korean J Med Mycol 2009; 14:23-27
Google Scholar
7. Kim YP, Chun IK, Kim SH. A case of kerion celsi caused by Trichophyton verrucosum and its epidemiologic study. Korean J Dermatol 1986;24:687-691
Google Scholar
8. Jang BS, Jo JH, Oh CK, Jang HS, Kwon KS. A case of kerion celsi caused by Trichophyton mentagrophytes. Korean J Med Mycol 2002;7:86-91
Google Scholar
9. Schwinn A, Ebert J, Brocker EB. Frequency of Trichophyton rubrum in tinea capitis. Mycoses 1995;38: 1-7
Crossref
Google Scholar
10. Elewski BE. Tinea capitis: a current perspective. J Am Acad Dermatol 2000;42:1-20
Crossref
Google Scholar
11. Kim KH, Lee WJ, Jun JB, Suh KB, Park JK. A case of kerion celsi in an adult caused by Trichophyton rubrum. Korean J Dermatol 1995;33:1114-1118
Google Scholar
12. Kim YJ, Choi JH, Bang JS, Suh MK, Lee JW, Kim TH, et al. A case of tinea capitis caused by Trichophyton rubrum in a 67-year-old woman. Korean J Med Mycol 2000;5:66-69
Google Scholar
13. Kim KS, Kim JW, Kye YC, Kim SN. A case of tinea capitis in an adult due to Trichophyton rubrum. Ann Dermatol 2000;12:189-192
Crossref
Google Scholar
14. Shin SJ, Lee JY, Yoo CS, Kim CW, Kim SS, Kim KH. Tinea capitis caused by Trichophyton rubrum in and adult woman judoist. Korean J Med Mycol 2012; 17:236-239
Google Scholar
15. Song JG, Yun SY, Suh MK, Ha GY, Jang TJ. Tinea capitis caused by Trichophytom rubrum in a 81-yearold woman. Korean J Med Mycol 2015;20:114-118
Crossref
Google Scholar
16. Bargman H, Kane J, Baxter ML, Summerbell RC. Tinea capitis due to Trichophyton rubrum in adult women. Mycoses 1995;38:231-234
Crossref
Google Scholar
17. Aste N, Pau M, Biggio P. Tinea capitis in adults. Mycoses 1996;39:299-301
Crossref
Google Scholar
18. Stiller MJ, Rowenthal SA, Weinstein AS. Tinea capitis caused by Trichophyton rubrum in a 67-year-old woman with systemic lupus erythematosus. J Am Acad Dermatol 1993;29:257-258
19. Mansur AT, Artunkal S, Ener B. Tinea capitis in an adult patient under treatment with trastuzumab. Mycoses 2010;54:609-610
Crossref
Google Scholar
20. Ko JH, Hwang YJ, Kim JY, Lee YW, Choe YB, Ahn KJ. A case of concomitant tinea infection diagnosed with molecular biologic technique. Korean J Med Mycol 2010;15:150-155
Google Scholar
