pISSN : 3058-423X eISSN: 3058-4302
Open Access, Peer-reviewed
pISSN : 3058-423X eISSN: 3058-4302
Open Access, Peer-reviewed
Jaeryuk Kim,Duckhee Kim,Jeonghyun Jang,Heungsup Sung,Mi-Na Kim
http://dx.doi.org/10.17966/KJMM.2016.21.3.84 Epub 2016 October 03
Abstract
Purpureocillium(P) lilacinum is a ubiquitous, saprophytic filamentous fungus that is infrequently reported in keratitis and cutaneous infections. However, the microbiological characterization of the culture isolates is limited in Korea. A 56-year-old male who suffered a pine needlestick to his right eye 10 days previously presented with ocular opacity and pain. A microscopic examination of a corneal scraping by Gram staining and calcofluor white staining was negative for bacteria and fungi. Fungal culture yielded pure white cottony molds on Sabouraud's dextrose agar after a 3-day incubation. Microscopic examination further revealed a mixture of a verticillate arrangement of phialides resembling the Penicillium structure and sparsely branched conidiophores bearing single to small clusters of conidia. This was initially presumed to be a species of Penicillium but the colonies never turned green with further incubation. It was subsequently identified as P. lilacinum by 28S rDNA sequencing and MALDI-TOF mass spectrometry. Antifungal susceptibility test revealed that this organism was resistant to flucytosine, amphotericin B, fluconazole, itraconazole, voriconazole, and caspofungin. After treatment with topical 5% voriconazole and oral itrazonazole combined with multiple debridements for 2 weeks, the patient was discharged with improved visual acuity. We thus report the first case of P. lilacinum infection that required molecular identification due to mixed conidiogenesis features and that showed laboratory-confirmed antifungal resistance in Korea.
Keywords
Drug resistance DNA sequencing Fungi Keratitis Matrix-assisted laser desorptionionization mass spectrometry Purpureocillium lilacinum
서 론
Purpureocillium lilacinum은 hyphomycetes에 속 하는 진균으로 토양, 곤충, 부패식물 등에 서식하며 임상 검체에서는 대개 오염균으로 분리된다. P.lilacinum은 드물게 각막염, 내안구염 등의 안감염과 국소 피부감염을 일으키며 면역저하자에게서 카테터 관련 진균혈증도 일으키는 것으로 보고되어 있다[1]. 국내에는 현재까지 P. lilacinum에 의한 감염은 각막염 2예[2],[3], 국소 피부감염 4예[4],[5],[6],[7] 등 총 6예가 보고되었다. P. lilacinum은 처음에 Penicillium lilacinum으로 명명된 이후 1974년 Paecilomyces lilacinus로 변경되었으며, 2011년 계통발생학적 분석을 통해 Paecilomyces 속에서 분리되어 Purpureocillium이라는 새로운 속으로 분류되었다[8]. 따라서 검사실에서 형태학적 감별을 시도할 경우 Paecilomyces 속의 특징과 함께 Penicillium 속의 특징을 보이기 때문에 동정에 오류가 발생할 수 있다[9],[10],[11]. P. lilacinum은 Paecilomyces 속이나 Penicillium 속과 달리 일반적으로 amphotericin B에 내성을 보이기 때문에 정확한 균종 동정이 임상적으로 중요하다[1]. 저자들은 진균성 각막염이 의심되는 환자의 각막도찰 배양에서 분리된 진균을 관찰했을 때 현미경적으로 두 가지 형태의 분생자형성 (conidiogenesis)이 혼재되어 있어 종 동정을 할 수 없었다. 이에 28S ribosomal DNA (28S rDNA)의 D1-D2 부위의 염기서열 분석과 matrix-assisted laser desorption ionization-time of flight (MALDI-TOF) mass spectrometry (MS)를 이용하여 P. lilacinum으로 동정하였기에 그 미생물학적 특성을 국내 문헌고찰과 함께 보고하고자 한다.
증 례
당뇨병으로 약물치료중인 56세 남자가 솔잎에 우안을 찔린 후 우안의 각막혼탁이 발생하여 개인의원에서 9일간 항바이러스제 및 항생제 점안과 항생제 경구 투여하였으나 증상 호전 없어 본원 안과에 내원하였다. 안과검사에서 나안시력은 우안 0.63, 좌안 0.8이었으며 세극등 검사상 우안에서 익상편과 결막충혈이 관찰되었으며 각막상피 결손과 결손주위로 깃털 모양의 각막기질 침윤 소견을 보였다. 이외 다른 신체적 특이 사항은 관찰되지 않았다. 혈당수치가 입원기간 중 정상보다 높았으나 이외 일반혈액검사, 소변검사, 간기능 및 신기능 검사와, 흉부 X-선 검사, 심전도 검사는 모두 정상 범위 내지 음성이었다.
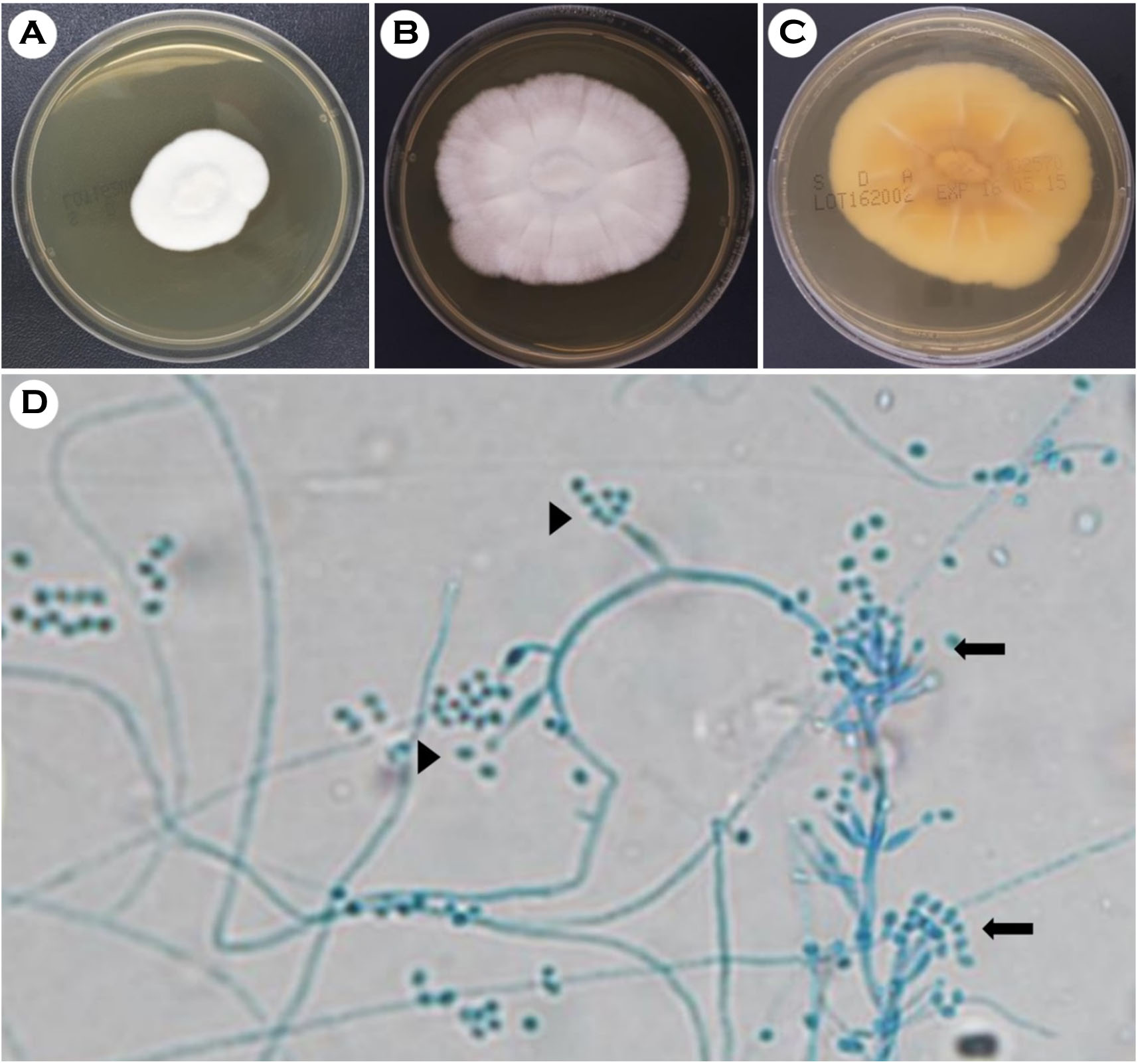
미생물학적 소견: 우안에서 채취한 각막도찰의 calcoflour white-KOH 염색 표본에서 진균이 관찰되지 않았다. Sabouraud dextrose agar (Shinyang Chemical, Seoul, Korea)에 접종하여 배양했을 때 37℃에는 자라지 않지만 25℃에서 3일만에 흰색의 보풀이 있는 집락이 자랐으며, 집락의 뒷면의 색깔은 담황색이었다(Fig. 1A, 1B, 1C). 이 집락으로 슬라이드 배양 표본을 만들어 lactophenol cotton blue로 염색하여 현미경 관찰을 하였다. 격막이 있는 균사(hyphae)로부터 분생자병(conidiophore)이 불규칙하게 분지하고 그 위로 경자(phialide)의 윤생(verticillate)구조가 관찰되었다. 경자 끝에는 타원형의 분생자가 사슬 모양으로 분포하여 Penicillium속과 유사한 구조를 보였다. 경자는 대체로 길쭉하고 끝으로 갈수록 가늘어지는 형태를보였다. 종종 균사로부터 바로 분지하는 한 가닥의 분생자병 끝에 분생자가 소수 달려있거나 군집을 이루는 형태가 함께 관찰되었다(Fig. 1D). 집락의 형태는 단일하였고 2주간 배양에서도 계속 흰색으로 남아있어 집락이 청록색으로 변하는 Penicillium 속과는 구분되었다. 3주째부터는 변연부가 라벤더 색깔로 변하였다. 이상의 집락과 현미경 소견으로는 정확하게 종 동정을 할 수 없었다.
배양된 집락으로부터 핵산을 추출하여 28SrDNA 내의 D1-D2 부위를 PCR법으로 증폭하여 염기서열 분석을 시행하였다. 분석된 542 bp의 염기서열을 GenBank에서 BLAST (The Basic Local Alignment Search Tool)로 검색한 결과 Paecilomyces lilacinus strain ATCC 10114 (GenBank accession number AY213717.1)와 Isaria takamizusanensis strain NHJ 3497 (GenBank accession number EU369033.1) 와 100% 일치하였다. 다음 순위로 Tolypocladiumsp. RG-2013a와 97% 일치하여 염기서열 분석에서는 Paecilomyces lilacinus / Isaria takamizusanensis로 동정할 수 있었다.
배양된 균을 BACTECTM Plus Aerobic/F 배지(BD Diagnostics, Sparks, MD, USA)에 접종하여 하룻밤 증균한 다음 70% formic와 acetonitrile로 전처리 후 MALDI biotyper (Bruker Daltonics, Bremen, Germany)의 진균 동정모드로 분석하였다. MALDI biotyper의 스코어값(score value)은 Paecilomyces lilacinus가 2.035로 1순위, Aspergillus terreus가 1.205로 차순위여서 Paecilomyces lilacinus로 종 동정되었다. 최종적으로 이 균종의 형태학적 특성과 분자생물학적 동정결과를 종합하여 P. lilacinum으로 동정하였다.
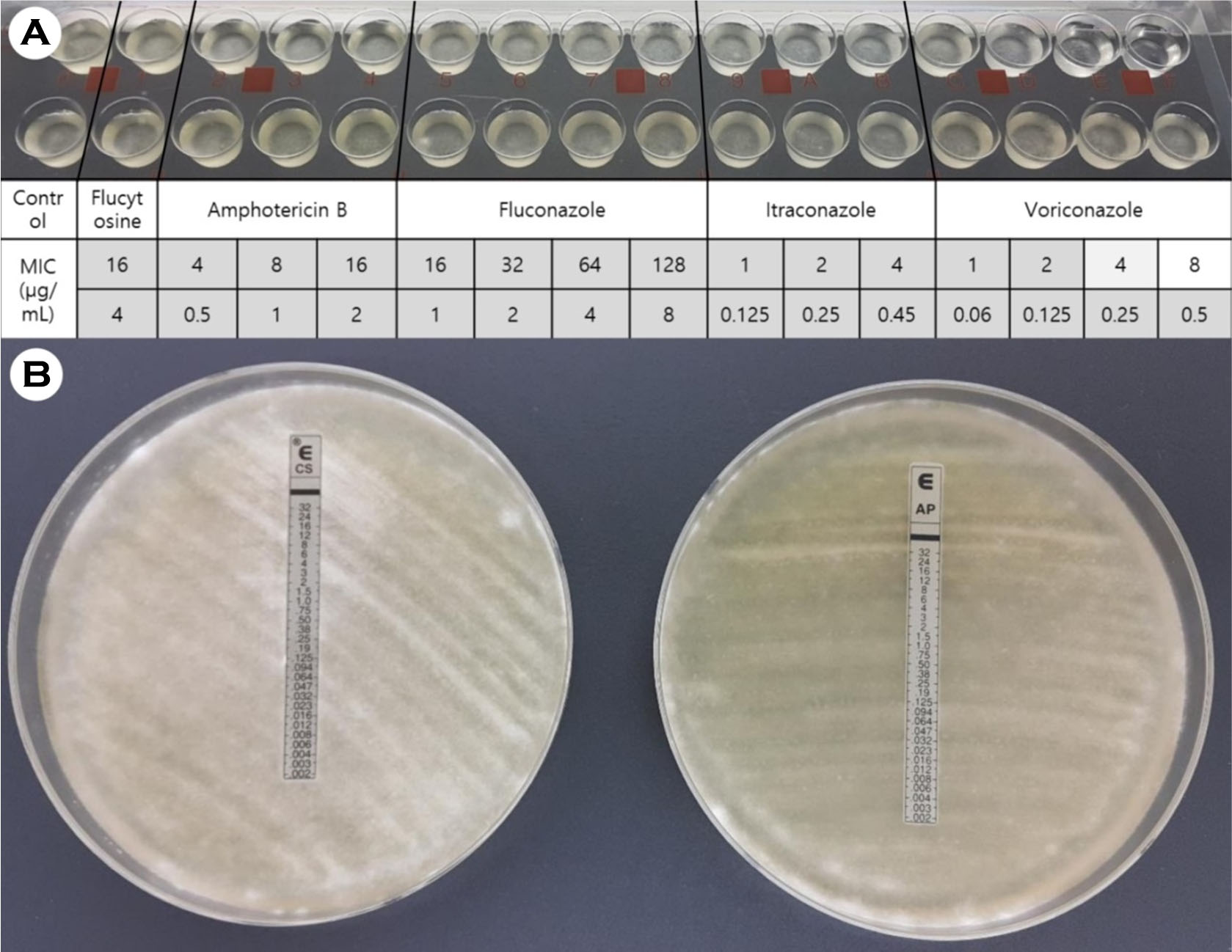
ATB FUNGUS 3 (bioMérieux, Marcy-l'Etoile, France)와 Epsilometer test (bioMérieux, Marcy-l'Etoile, France)를 사용하여 항진균제 감수성 검사를 시행하였다. MIC는 각각 flucytosine은 >16 μg/mL, amphotericin B는 >16 μg/mL, fluconazole은 >128 μg/mL, itraconazole은 >4 μg/mL, voriconazole은 4 μg/mL를 보였다. Epsilometer test에서 amphotericin B와 caspofungin에 대해 억제대가 관찰되지 않았다(Fig. 2).
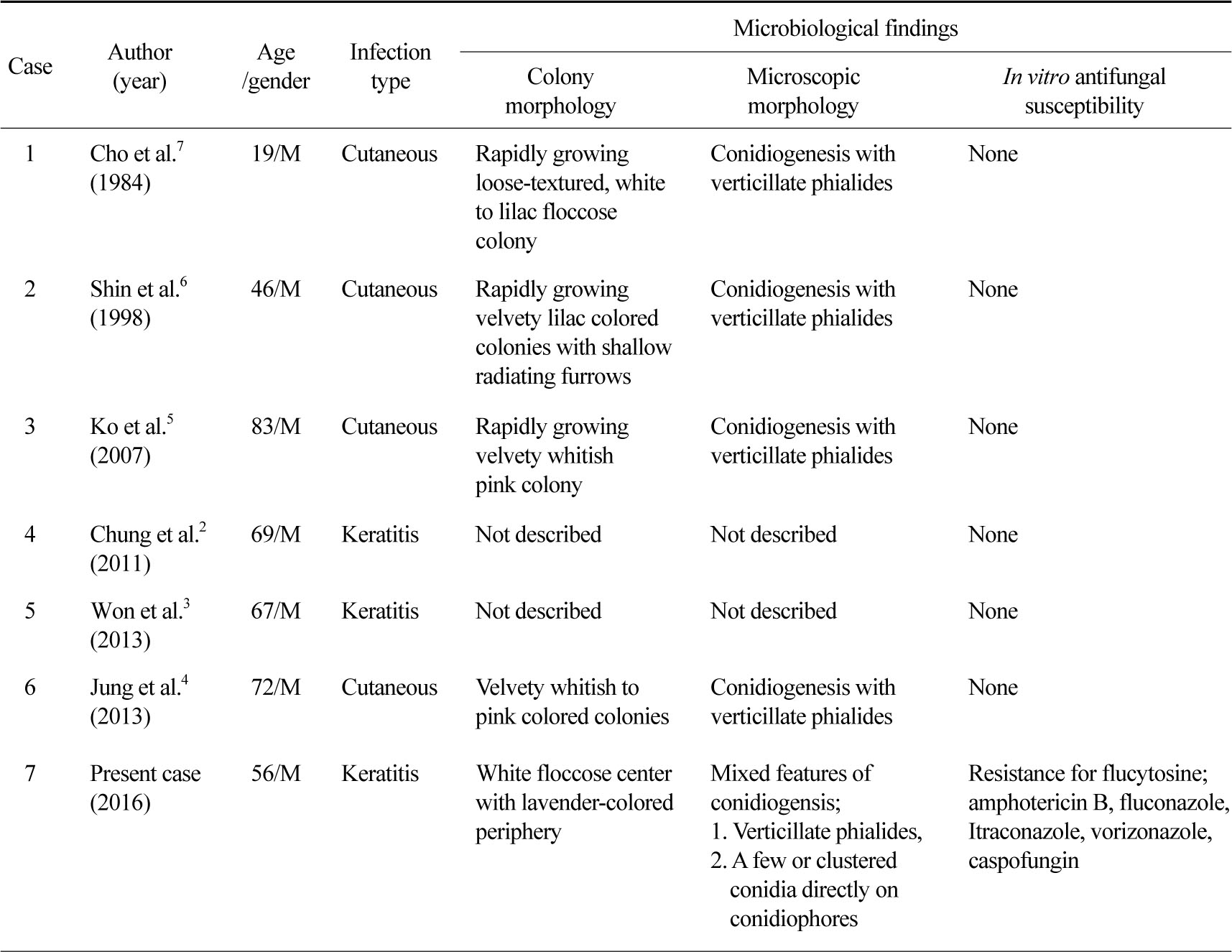
국내에 현재까지 P. lilacinum 감염사례는 각막염 2예와 국소 피부감염 4예가 있었다. 이들 보고와 이번 증례의 미생물학적 소견을 찾아서 비교하였다. 각막염 2예는 P. lilacinum의 미생물학적 소견에 대한 기술이 없었고 국소 피부감염 4예는 형태학적 소견에 대해 기술하고 있으나 두 가지 형태의 분생자형성 중 윤생구조만 기술하여 Paecilomyces속에 합당한 형태만 강조하고 있었다. 6예 모두 항진균제 감수성 검사는 실시하지 않았다(Table 1).
치료 및 경과: 입원 중 우안의 병변에 대해 수 차례 변연절제술을 시행하였으며 5% voriconazole을 30분 간격으로 점안하고 1일 2회 itrazonazole 100 mg 경구 투여를 하였다. 2주 후 안통증이 호전되어 퇴원하였고 외래에서 5% voriconazole을 2시간 간격으로 점안하고 1일 2회 itrazonazole 100 mg 경구 투여하도록 처방 후 추적 관찰하였다. 4주 후 시력과 각막상피 결손이 호전되었다.
고 찰
이 증례는 우안의 각막염 병변에서 분리된 진균을 형태학적, 분자생물학적 검사로 P. lilacinum으로 동정하여 P. lilacinum에 의한 각막염으로 진단할 수 있었다. P. lilacinum에 의한 감염은 주로 면역 기능이 저하된 환자에서 발생하나 면역 기능이 정상인 환자에서도 발생할 수 있으며 각막염, 내안구염 등의 안감염이 가장 흔하며 피부감염이 두 번째로 흔하다[1]. P. lilacinum에 의한 각막염의 위험인자는 만성 각막병증 또는 안과적 수술력, 각막외상, 콘택트 렌즈 착용 순으로 알려져있다[12]. 이 증례의 환자는 당뇨병을 앓고 있어 면역저하 상태였으며 솔잎에 우안을 찔린 이후 각막염이 발병하여 각막이 손상될 위험인자를 가지고 있었다. 국내에는 P. lilacinum 각막염 2예가 보고되어 있으며 2예 모두 안과적 수술력이 있어 각막손상에 의해 P. lilacinum 감염이 초래되었다.
P. lilacinum은 Paecilomyces 속의 P. variotii나 Penicillium 속과 현미경적으로 유사하지만 집락의 성상 및 현미경적 특징적 소견으로 감별할 수 있다. P. lilacinum의 집락은 라벤더색을 띠는 반면에 P. variotii의 집락은 올리브 갈색을 띠며 현미경적 으로 유사한 형태의 경자의 윤생구조를 보이지만 P. lilacinum이 P. variotii에 비해 경자 사이의 공간이 더 좁아 밀집된 구조를 보인다[13]. Penicillium 속은 초기에는 P. lilacinum과 마찬가지로 흰색을 띠지만 성숙해지면 청록색으로 색깔이 변하여 감별 할 수 있다[13]. 현미경적으로 P. lilacinum은 경자의 윤생구조가 밀집되어 마치 Penicillium 속의 구조처럼 보일 수 있다. 그러나 P. lilacinum은 경자가 날씬하고 끝으로 갈수록 가늘어지며 분생자가 타원형이어서 좀더 짧고 뭉툭한 모양의 경자와 원형의 분생자를 가진 Penicillium 속과 감별할 수 있다[13],[14]. 또한 P. lilacinum은 경자의 윤생구조와 함께 Fusarium 속 또는 Acremonium 속과 유사하게 균사로부터 바로 분지하는 한 개의 분생자 끝에 분생자가 소수 또는 다수가 군집을 이루는 형태가 혼재되어 보일 수 있다[8],[15]. 따라서 형태학적 동정만을 시도할 경우 한 가지 형태의 분생자형성만 관찰하여 오동정을 할 수 있다.
이 증례에서는 분리된 균주를 25℃에서 배양했을 때 빠르게 자라 3일만에 평편하고 흰색의 보풀이 있는 집락이 관찰되었으며 현미경적으로 Penicillium 속과 유사한 구조가 관찰되어 처음에는 Penicillium 속으로 판단하였다. 그러나 집락의 색깔이 2주간 배양에서도 청록색으로 변하지 않고 현미경적으로 Fusarium 속 또는 Acremonium 속과 유사한 형태의 분생자형성이 혼재된 양상을 보여 형태학적으로는 동정을 할 수 없었다. 이에 28S rDNA 내의 D1-D2 부위의 염기서열 분석을 시행하였고 Paecilomyces lilacinus와 Isaria takamizusanensis에 100% 일치하여 두 균종을 감별할 수 없었다. I. takamizusanensis는 곤충에 기생하는 진균으로 인체감염이 보고된 예는 없으며 2015년 EF-1α (elongation factor 1-α) 유전자에 기반한 계통발생학적 분석으로 Purpureocillium 속임을 확인하여 Purpureocillium takamizusanense로 새로이 명명되었다[16]. 따라서 이 증례에서 실시한 D1-D2 부위의 염기서열 분석으로는 P. lilacinum과 P. takamizusanensis를 구분할 수 없었다. 이에 비해 MALDI Biotyper의 진균 동정모드로 분석을 시행했을 때는 2.0 이상의 높은 스코어값으로 Paecilomyces lilacinus를 종수준까지 동정할 수 있었다. 이전 연구에서 분자생물학적으로 확인된 9주의 Paecilomyces lilacinus에 대하여 MALDI Biotyper로 동정이 된 6주는 모두 2.0 이상의 스코어값으로 Paecilomyces lilacinus로 종수준까지 동정이 되었고 나머지 3주는 동정에 실패하였다(No identification)[17]. P. lilacinum의 종수준 동정에는 MALDI-TOF MS 등의 분자생물학적 동정법을 이용하는 것이 효과적일 것이다.
P. lilacinum에 의한 각막염의 표준 치료법은 아직 확립되어 있지 않으며 항진균제 치료로 완치된 경우가 31%에 불과하고 전층각막이식 등의 수술을 받은 경우가 69%에 이른다[12]. 따라서 P. lilacinum의 항진균제 감수성을 고려하여 적절한 항진균제를 선택하는 것이 예후에 중요하다. P. lilacinum은 amphotericin B, flucytosin, fluconazole에 생체 외에서 고도의 MIC (minimum inhibitory concentration)를 보이는 것으로 알려져 있다[1]. Itraconazole, posazonazole, voricozole은 다양한 범위의 MIC를 보이며, 특히 voriconazole은 0.12~4 μg/mL의 넓은 범위의 MIC를 보이는 것으로 알려져 있다[1]. Caspofungin과 micafungin은 일반적으로 고도의 MIC를 보이지만 낮은 MIC를 보이는 균주도 보고된 바 있다[18]. 국내에서 P. lilacinum에 대한 항진균제 감수성 검사는 보고된 적이 없으며 이 증례에서는 amphotericin B, flucytosine, fluconazole, itraconazole, voriconazole에 내성을 보였다. P. lilacinum 과 현미경적으로 유사하여 오인될 수 있는 P. variotii와 Penicillium 속은 amphotericin B에 감수성인 반면에, P. lilacinum은 amphotericin B에 고도의 내성을 보이기 때문에[8],[10] 종 감별에 유용하다. 이처럼 P. lilacinum은 다제내성을 보일 수 있기때문에 적절한 항진균제 선택을 위해서 정확한 균종 동정이 임상적으로 중요하다.
이 증례는 국내에서 최초로 염기서열 분석과 MALDI-TOF MS로 P. lilacinum을 동정하고 항진균제 감수성 검사를 실시한 P. lilacinum에 의한 감염 예이다. P. lilacinum은 형태학적으로 동정할경우 오류가 발생할 수 있기 때문에 분자생물학적 방법을 이용하여 정확히 종 동정하는 것이 유용하며, 특히 MALDI-TOF MS를 이용하여 신속하게 종수준의 동정을 할 수 있다.
Conflict of interest
In relation to this article, I declare that there is no conflict of interest.
References
1. Pastor FJ, Guarro J. Clinical manifestations, treatment and outcome of Paecilomyces lilacinus infections. Clin Microbiol Infect 2006;12:948-960
Crossref
Google Scholar
2. Chung SR, You IC, Cho NC, Ahn M. Paecilomyces keratitis: cases in Korea and literature review. J Korean Ophthalmol Soc 2016;57:390
Crossref
Google Scholar
3. Won JY, Shin JY, Hwang JH, Joo CK. A case of fungal keratitis caused by Paecilomyces lilacinus after penetrating keratoplasty. J Korean Ophthalmol Soc 2014;55:1384-1387
Crossref
Google Scholar
4. Jung MY, Park JH, Lee JH, Lee JH, Yang JM, Lee DY. A localized cutaneous Paecilomyces lilacinus infection treated with voriconazole. Korean J Dermatol 2013;51:833-836
Google Scholar
5. Ko WT, Kim SH, Suh MK, Ha GY, Kim JR. A case of localized skin infection due to Paecilomyces lilacinus. Korean J Dermatol 2007:930-933
Google Scholar
6. Shin SB, Lee HN, Kim SW, Park GS, Cho BK, Kim HJ. Cutaneous abscess caused by Paecilomyces lilacinus in a renal transplant patient. Korean J Med Mycol 1998;3:185-189
Google Scholar
7. Cho GY, Cho EH, Choi GJ, Hong NS, Houh W. Facial cutaneous mycosis by Paecilomyces lilacinus. Korean J Dermatol 1984;22:89-93
Google Scholar
8. Luangsa-Ard J, Houbraken J, van Doorn T, Hong SB, Borman AM, Hywel-Jones NL, et al. Purpureocillium, a new genus for the medically important Paecilomyces lilacinus. FEMS Microbiol Lett 2011;321:141-149
Crossref
Google Scholar
9. Saberhagen C, Klotz SA, Bartholomew W, Drews D, Dixon A. Infection due to Paecilomyces lilacinus: a challenging clinical identification. Clin Infect Dis 1997;25:1411-1413
Crossref
Google Scholar
10. Sheybani A, Nguyen AT, Harocopos G, Lubniewski AJ, Huang AJ. A masquerader? Paecilomyces must be distinguished from Penicillium in fungal keratitis: a report of two contrasting cases. BMJ Case Rep 2015: 2015
Crossref
Google Scholar
11. Van Schooneveld T, Freifeld A, Lesiak B, Kalil A, Sutton DA, Iwen PC. Paecilomyces lilacinus infection in a liver transplant patient: case report and review of the literature. Transpl Infect Dis 2008;10:117-122
Crossref
Google Scholar
12. Yuan X, Wilhelmus KR, Matoba AY, Alexandrakis G, Miller D, Huang AJ. Pathogenesis and outcome of Paecilomyces keratitis. Am J Ophthalmol 2009;147: 691-696 e693
Crossref
Google Scholar
13. Larone DH. Medically important fungi: a guide to identification. 5th ed. New York: Am Soc Microbiol, 2011:294-6,299
14. Campbell CK, Johnson EM, Warnock DW. Moulds with enteroblastic conidia adhering in chains. In: Identification of pathogenic fungi 2nd ed.: Wiley- Blackwell, 2013:129-159
Crossref
Google Scholar
15. Okada G, Sakai N, Yamagishi M. Acremonium-like submerged conidiation in Paecilomyces nostocoides and P. lilacinus. Mycoscience 1995;36:345-351
Crossref
Google Scholar
16. Ban S, Azuma Y, Sato H, Suzuki K, Nakagiri A. Isaria takamizusanensis is the anamorph of Cordyceps ryogamimontana, warranting a new combination, Purpureocillium takamizusanense comb. nov. Int J Syst Evol Microbiol 2015;65:2459-2465
Crossref
Google Scholar
17. Schulthess B, Ledermann R, Mouttet F, Zbinden A, Bloemberg GV, Böttger EC, et al. Use of the Bruker MALDI Biotyper for identification of molds in the clinical mycology laboratory. J Clin Microbiol 2014; 52:2797-2803
Crossref
Google Scholar
18. Castelli MV, Alastruey-Izquierdo A, Cuesta I, Monzon A, Mellado E, Rodriguez-Tudela JL, et al. Susceptibility testing and molecular classification of Paecilomyces spp. Antimicrob Agents Chemother 2008;52: 2926-2928
Crossref
Google Scholar
