pISSN : 3058-423X eISSN: 3058-4302
Open Access, Peer-reviewed
pISSN : 3058-423X eISSN: 3058-4302
Open Access, Peer-reviewed

Eun Hye Hong,Ye Ji Jang,Eun Byul Cho,Eun Joo Park,Kwang Joong Kim,Kwang Ho Kim
10.17966/JMI.2019.24.2.58 Epub 2019 July 03
Abstract
Onychomycosis is a fungal nail infection caused mainly by dermatophytes. Non-dermatophytes such as yeasts, Acremonium, Aspergillus, and Fusarium species account for only 10% of onychomycosis, and Fusarium species are relatively common amongst these pathogens. However, the main Fusarium species pathogens are Fusarium solani and Fusarium oxysporum. Fusarium proliferatum is a rare pathogen in onychomycosis, and only a few cases have been reported worldwide. We report a case of a 68-year-old woman presenting with a white- to yellow-colored patch on her left third fingernail plate, which was diagnosed by fungus culture and sequencing as onychomycosis caused by Fusarium proliferatum.
Keywords
Fusarium proliferatum Fungus Onychomycosis Sequencing
Onychomycosis, fungal infection of the nail, is common but difficult to treat. Non-dermatophyte molds account for approximately 10% of onychomycosis worldwide1, and it is hard to clinically differentiate non-dermatophyte from dermatophyte infection. Therefore, evaluations such as fungus culture, biopsy and sequencing should be performed to identify the exact strain of the fungus. One of the non-dermatophyte molds is Fusarium species, a saprophyte abundant in soil and involved mainly in decaying crops. Human infection caused by Fusarium species is distinct from local infections such as keratitis, skin infection and onychomycosis, and systemic infections2. In onychomycosis, Fusarium species commonly affects toenails which have existing trauma or nail dystrophy. Fusarium solani and Fusarium oxysporum are relatively common pathogens3,4, but Fusarium proliferatum is a rare pathogen. We report a case of a 68-year-old woman with fingernail onychomycosis caused by Fusarium proliferatum, which was diagnosed by fungus culture and sequencing.
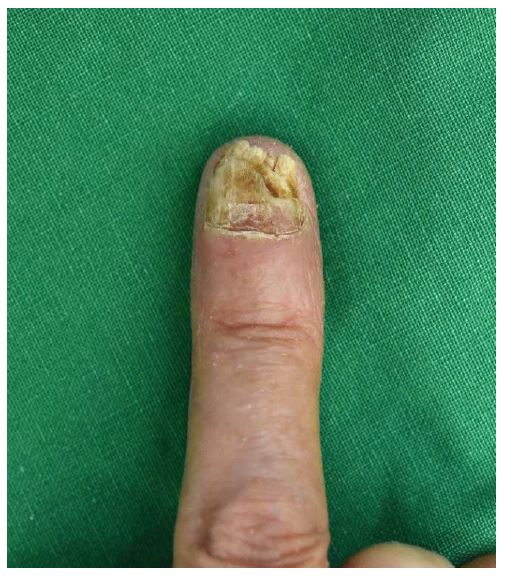
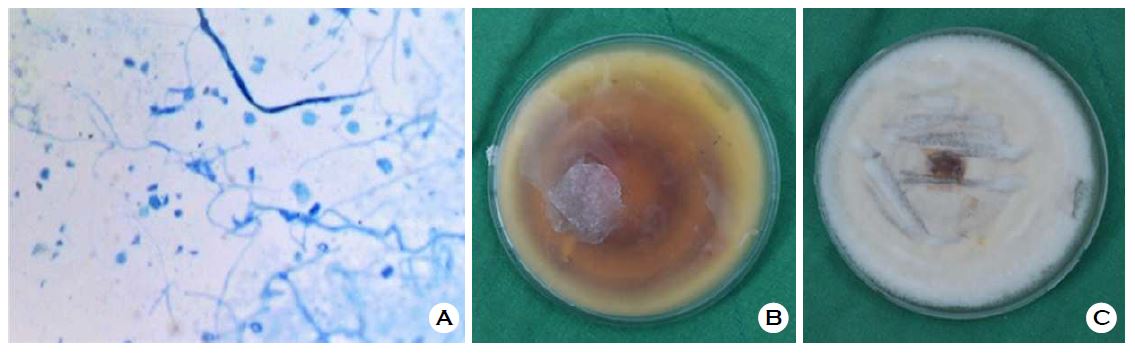
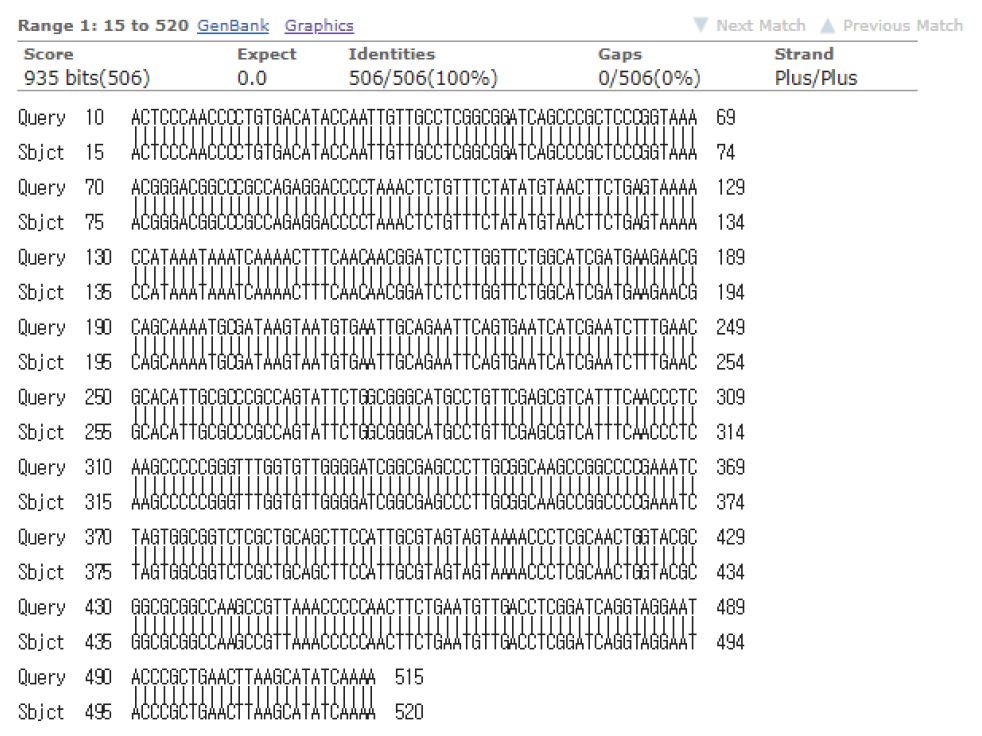
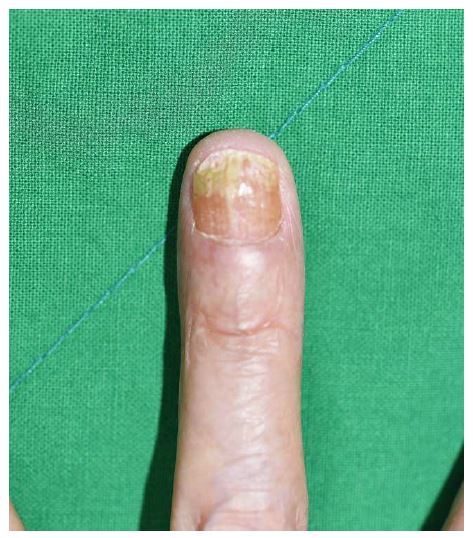
A 68-year-old woman presented with an onychodystrophic nail lesion on the left third fingernail, which occurred after chemotherapy for advanced gastric cancer. Upon initial examination, it manifested as white- to yellow-colored patches on the left third fingernail plate, with a rough surface and subungual hyperkeratosis (Figure 1). It was accompanied by nail brittleness and whitish horizontal lines on the proximal part of the nail. A smear with 10% potassium hydroxide (KOH) and fungal culture were performed. The KOH smear showed a number of hyphae, and non-dermatophyte type mold was cultured on Sabouraud's dextrose agar plates, suggesting fungal infection. The patient started four cycles of oral itraconazole pulse therapy (200 mg bid × 7 days) and 5% topical amorolfine treatment, but the condition did not improve. A KOH smear and fungal cultures were conducted again to identify the reason for this failure. The KOH smear showed multiple long hyphae with vertical branches (Figure 2A). After incubation in Sabouraud's dextrose agar plate at 25℃ for four days, colonies started to grow. White-colored villous colonies with central brownish discoloration were formed, suggesting infection by Fusarium species (Figure 2B, C). To identify the exact strain of fungus, sequencing was performed with an internal transcribed spacer (ITS) region isolated from the colonies. This sequence was 100% identical with Fusarium proliferatum (GenBank accession number EF534188.1, Figure 3). A BLAST search showed that the most similar strain was Fusarium proliferatum. The patient was finally diagnosed as suffering from onychomycosis caused by Fusarium proliferatum. She was treated with oral fluconazole 150 mg per week, topical amorolfine 5%, and laser therapies simultaneously. Topical amorolfine 5% was applied after CO2 laser holing. The lesion had improved a year after her first visit (Figure 4), but follow-up was lost due to the patient discontinuing visits to our clinic.
Onychomycosis is a fungal infection of nails caused by dermatophytes, non-dermatophytes, and yeasts. The causative agents of 90% of onychomycosis are dermatophytes such as Trichophyton rubrum and Trichophyton interdigitale, and the remaining 10% is caused by non-dermatophyte fungus such as yeast, Acremonium, Aspergillus, and Fusarium species5. Fusarium species accounts for about 3% of all onychomycosis6. Fusarium species is a harmless saprotroph and is widely distributed throughout the world. It causes a wide range of infections, from local opportunistic infections such as keratitis and onychomycosis to systemic infections in immunosuppressed patients3. Onychomycosis caused by Fusarium species mainly occurs in toenails with previous dysplasia or traumas, and infections involving the fingernail are not common. In previous case reports, onychomycosis caused by Fusarium species showed clinical features of distal and lateral subungual onychomycosis7. The most common pathogens among Fusarium species are Fusarium oxysporum and Fusarium solani. In a KOH smear, the hyphae vary in thickness, with branches at 45 degrees or 90 degrees, and multiseptated fusiform macroconidias are observed8. Fusarium species grows rapidly in Sabouraud's dextrose agar plate at room temperature and forms colonies covered with white fluffy hyphae within four to five days. Various colors such as purple, orange and green appear at the later stages, according to the species9.
In the case reported here, onychomycosis developed in an immunocompromised patient after chemotherapy for advanced gastric cancer. There was no evidence of any other systemic infection or local infection such as keratitis. The clinical features of the nail lesion were similar to those of distal and lateral subungual onychomycosis. However, it is noteworthy that our case occurred in the fingernail, as toenails are the main site of onychomycosis caused by Fusarium species.
As Fusarium species is ubiquitous in soil, onychomycosis cannot be diagnosed only because it is observed in nails. Diagnosis is possible if Fusarium species is cultured over time, and if dermatophyte infection is excluded10. Recently, the nucleotide sequence analysis of the ITS region of the fungus strain has been used to confirm the pathogen causing onychomycosis11.
In this case, a Fusarium species were cultured in two fungus cultures. To identify the exact fungus strain, we performed nucleotide sequencing of the ITS region isolated from the fungus DNA and BLAST was performed using the DNA sequence. Fusarium proliferatum was the highest-scoring result, and the patient was finally diagnosed as having onychomycosis caused by Fusarium proliferatum.
Some previous case reports of Fusarium onychomycosis showed successful treatment with itraconazole or terbinafine7. However, in this case, the patient was resistant to itraconazole and the treatment was changed to fluconazole. She also received topical antifungal therapy and laser therapy, including topical amorolfine 5% applied after CO2 laser holing. After the combination therapy, her nail lesion improved. Some research has been undertaken into the effectiveness of laser therapy in treating onychomycosis, but there is no clear consensus. Further studies regarding effective antifungal therapy for Fusarium onychomycosis and the use of laser therapy in treating onychomycosis are needed.
A few cases of onychomycosis caused by Fusarium have been previously reported, of which Fusarium proliferatum accounts for a small percentage. In Korea, cases of Fusarium solani, Fusarium oxyporum and Fusarium verticilloides infections have been reported9,12,13. There are a few cases of onychomycosis due to Fusarium proliferatum but, as far as we know, it has not yet been reported in Korea. Therefore, we report a rare case of onychomycosis occurred in the left third fingernail, caused by Fusarium proliferatum.
The patient provided written informed consent for the publication and the use of his or her images.
References
1. Welsh O, Vera-Cabrera L, Welsh E. Onychomycosis. Clin Dermatol 2010;28:151-159
2. Bodey GP, Boktour M, Mays S, Duvic M, Kontoyiannis D, Hachem R, et al. Skin lesion associated with Fusarium infection. J Am Acad Dermatol 2002;47:659-666
Google Scholar
3. Gupta AK, Baran R, Summerbell RC. Fusarium infections of the skin. Curr Opin Infect Dis 2000;13:121-128
4. Baran R, Tosti A, Piraccini BM. Unknown clinical patterns of Fusarium nail infection: report of three cases. Br J Dermatol 1997;136:424-427
Google Scholar
5. Schieke SM, Garg A. Superficial fungal infection. In: Goldsmith LA, Katz SI, Gilchrest BA, Paller AS, Leffell DJ, Wolff K, editors. Fitzpatrick's dermatology in general medicine. 8th ed. New York: McGraw-Hill, 2012:2278-2297
6. Ninet B, Jan I, Bontems O, Léchenne B, Jousson O, Lew D, et al. Molecular identification of Fusarium species in onychomycoses. Dermatology 2005;210:21-25
Google Scholar
7. Hattori N, Shirai A, Sugiura Y, Li W, Yokoyama K, Misawa Y, et al. Onychomycosis caused by Fusarium proliferatum. Br J Dermatol 2005;153:647-649
Google Scholar
8. Liu K, Howell DN, Perfect JR, Schell WA. Morphologic criteria for the preliminary identification of Fusarium, Paecilomyces, and Acremonium species by histopathology. Am J Clin Pathol 1998;109:45-54
Google Scholar
9. Hyun DN, Won JH, Park JS, Chung H, Jun JB. A case of onychomycosis caused by Fusarium verticillioides. Korean J Med Mycol 2008;13:26-30
Google Scholar
10. Brasch J, Shimanovich I. Persistent fingernail onychomycosis caused by Fusarium proliferatum in a healthy woman. Mycoses 2012;55:86-89
Google Scholar
11. Takahata Y, Hiruma M, Sugita T, Muto M. A case of onychomycosis due to Aspergillus sydowii diagnosed using DNA sequence analysis. Mycoses 2008;51:170-173
Google Scholar
12. Lim SW, Kwon SW, Suh MK, Lee HC, Choi JH, Lee JW, et al. A case of onychomycosis caused by Fusarium solani. Korean J Med Mycol 2003;8:21-25
Google Scholar
13. Kim JE, Park HJ, Lee JY, Cho BK, Kim SO. A case of onychomycosis with acute paronychia caused by Fusarium oxysporum. Korean J Med Mycol 2002;7:170-174
Google Scholar
Congratulatory MessageClick here!
