pISSN : 3058-423X eISSN: 3058-4302
Open Access, Peer-reviewed
pISSN : 3058-423X eISSN: 3058-4302
Open Access, Peer-reviewed

Hyojin Kim,Gyeong Je Cho,Jong Uk Kim,Woo Jung Jin,So Hee Park,Seung Hyun Moon,Jung Eun Seol,Jeong Hwan Shin
10.17966/JMI.2019.24.2.52 Epub 2019 July 03
Abstract
Purpureocillium is a genus of saprophytic fungi that is commonly found in soil or rotting material. Although rarely a pathogen in humans, it can cause serious infections in immunocompromized patients. An 85-year-old woman presented with a 2-week history of pruritic erythematous plaques with yellowish crusts on her right forearm and dorsal hand. Histopathological analysis identified fungal hyphae and spores in the dermis, and Purpureocillium lilacinum was identified through tissue culture, polymerase chain reaction, and DNA sequencing. The skin lesion barely responded to 4 weeks of itraconazole treatment but improved upon the addition of terbinafine. The skin lesion was completely cured after 12 weeks, with no recurrence to date. Here, we report a rare deep cutaneous fungal infection caused by P. lilacinum in an immunocompetent patient and postulate that, in this case, the patient's agricultural lifestyle increased the possibility of P. lilacinum infection.
Keywords
Deep fungal infection Immunocompetent host Purpureocillium lilacinum
Purpureocillium species are ubiquitous saprophytic fungi1,2. Purpureocillium lilacinum was once named Paecilomyces lilacinus, but a phylogenetic analysis in 2011 led to its reclassification in the new genus Purpureocillium3. Paecilomyces lilacinum is a rare pathogen in humans1-6. Ocular involvement is the most common human manifestation followed fby cutaneous infection7. Although cutaneous infection by Purpureocillium is mostly seen in immunocompromized patients, immunocompetent hosts can be infected1. There is no standard treatment, and several systemic antifungal agents, and surgical excision are used8,9.
We encountered a rare case of cutaneous infection by P. lilacinum in an otherwise healthy immunocompetent patient who lived in a rural area. Since greater awareness of cutaneous P. lilacinum infection in immunocompetent patients is needed, we report this case with a literature review.
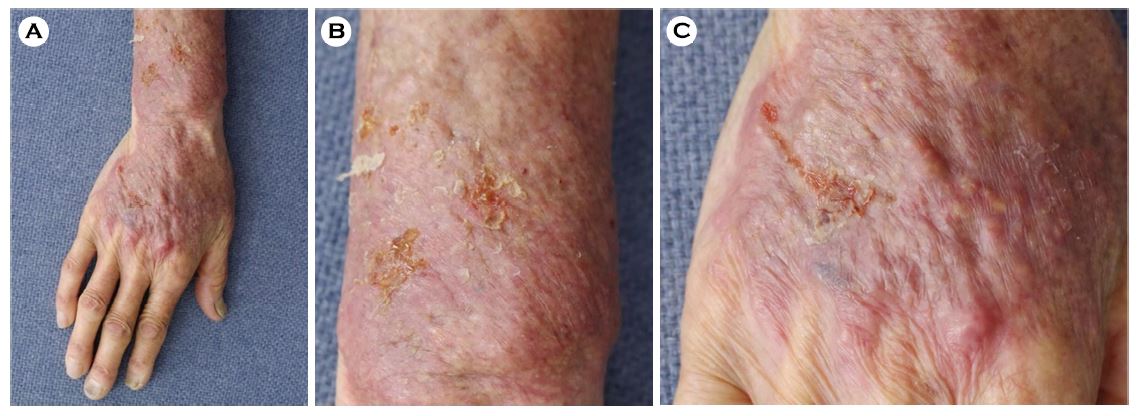
An 85-year-old woman presented with a 2-week history of erythematous plaques with surface nodularity and eczematoid yellowish crusts on her right forearm and dorsal hand (Figure 1). She lived alone and farmed in a rural area, and reported no noteworthy medical or family history. There was also no trauma or contact history.
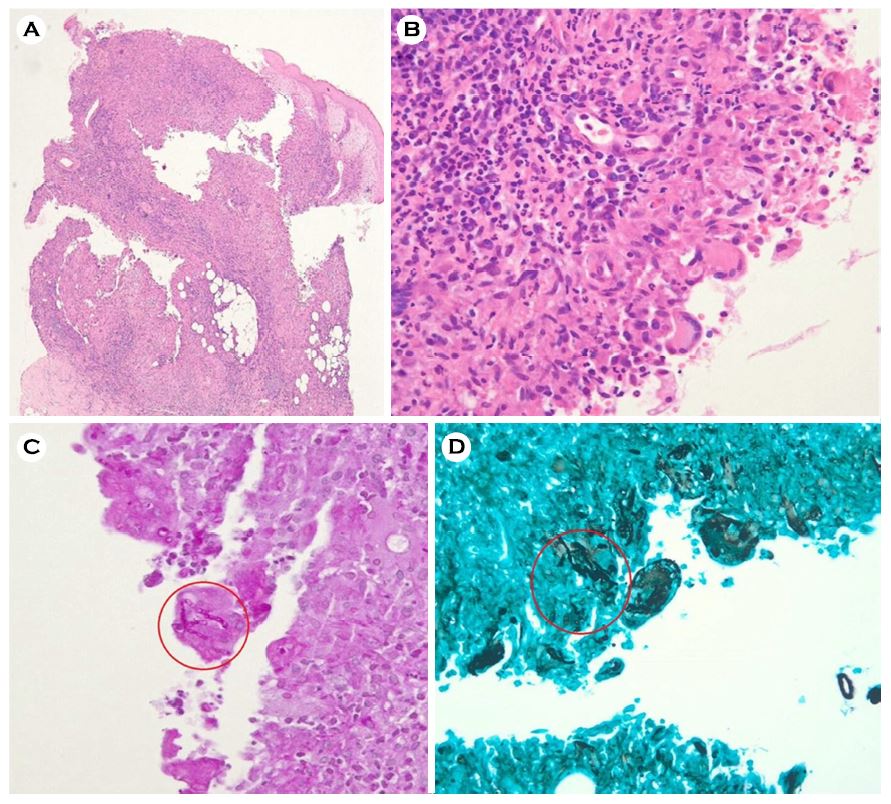
Cutaneous scraping for a 10% potassium hydroxide smear identified no fungal elements and histopathological examination of a right forearm biopsy revealed dense inflammatory infiltration in the dermis at low magnification (Figure 2A) and granulomatous changes with neutrophils, histiocytes, plasma cells, and giant cells in the dermis (Figure 2B). Purplish branching fungal hyphae were observed among the inflammatory cells after staining with Periodic acid-Schiff (Figure 2C), and black hyphae and spores were also observed upon Gomorimethenamine silver staining (Figure 2D).
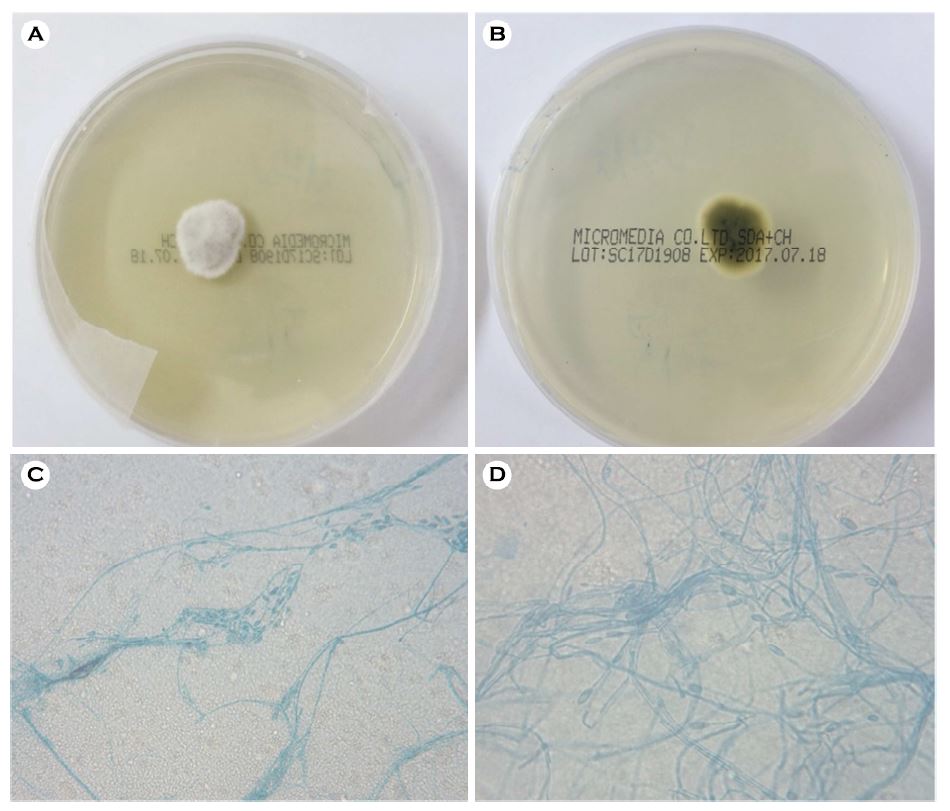
Culture of a small segment of the biopsied specimen on Sabouraud dextrose agar produced a whitish dome-shaped floccose colony with shallow radiating furrows after 5 days at 25℃ (Figure 3A). The reverse side was dark green (Figure 3B). The cultured organism exhibited long thin-walled entangled hyphae with single oval conidia after colonies were stained with lactophenol cotton blue and examined microscopically (Figure 3C, 3D).
The identity of the organism was confirmed by sequencing the D1-D1 region of its 28S rRNA and the internal transcribed spacer.* Purified DNA from the polymerase chain reaction was sequenced with a BigDye Terminator Cycle sequencing kit (Applied BioSystems, Foster City, CA, USA) and ABI PRISM 3130 genetic analyzer (Applied Biosystems). All sequences were compared with those of similar strains using BLAST analysis. The sequence analysis indicated 100.0% homology with P. lilacinum ACTT 10114 (GenBank accession no. AY213717.1 and GenBank accession no. AY213665.1). We, therefore, identified our isolate as P. lilacinum.
The skin lesion barely responded to 4 weeks of systemic treatment with itraconazole, so terbinafine was added to the therapy, after which improvement was evident. The skin lesion was completely cured after 12 weeks of combination therapy, and there has been no recurrence to date.
Purpureocillium is a genus of saprophytic molds that is commonly found in soil or decaying organic material but is a relatively uncommon pathogen of humans1,2. It was first described as Penicillium lilacinum by Bainer in 190710 and then renamed Paecilomyces lilacinus by Samson in 19743. Finally, Luangsa-Ard et al. reclassified it in the new genus Purpureocillium after a phylogenetic analysis in 201111.
Fenech and Mallia first isolated P. lilacinum in a human in 1972 from a patient with a pleural effusion12, and Takayasu et al.3 reported a cutaneous infection in 1977. Ocular involvement, such as iatrogenic keratitis and endophthalmitis after artificial lens implantation, comprises 51.3% of all reported human infections, followed by cutaneous infection at 35.3%1. Other reported sites of infection include the sinuses, endocardium, and lungs7. Cutaneous P. lilacinum infection occurs primarily in immunocompromized patients with a history of organ transplantation, long-term steroid use, malignancy, or acquired immunodeficiency syndrome, and it is considered rare in immunocompetent patients1,9,13. Moreover, 18.6% of the infections seen in immunocompetent patients have no identified trigger factor1.
Since the first immunocompetent host was described in 1977, there have been 14 cases of cutaneous P. lilacinum infection in immunocompetent patients reported worldwide (Table 1)1,11,14-18. The patient age distribution was from 7 to 86 (mean 48.2) years with no gender preference was evident. Of note, all of the infection sites were exposed areas such as the face, arm, or leg, and a preceding trauma was clearly identified in only two cases. Recent cases of immunocompetent farmers developing P. lilacinum infection with no specific antecedent event have also been reported14,15. It can be inferred that an agricultural lifestyle involving minor trauma and routine contact with soil may be the source of infection in immunocompetent patients. Our patient also lived in a rural area and was in frequent contact with soil, which may have increased the risk of deep cutaneous fungal infection by P. lilacinum. Considering the infection site and the patient's rural lifestyle, we postulate that our patient experienced recurrent minor trauma that she did not remember, and was infected by P. lilacinum from the soil.
Diagnosis of P. lilacinum infection is based on the identification of the fungal organism. Histopathological examination, tissue culture in Sabouraud dextrose agar with lactophenol cotton blue staining, and molecular analysis can help to diagnose deep cutaneous fungal infection by P. lilacinum 9,14,15. Diagnosing P. lilacinum accurately is important because each species in the genus Purpureocillium exhibits resistance to different antifungal agents19. P. lilacinum is resistant to conventional antifungal agents, including amphotericin B, fluconazole, and flucytosine, and its in vitro susceptibility to itraconazole varies1,13. Voriconazole is a promising therapeutic agent14,20, although there is no established dosage for this antifungal medication and no widely accepted treatment period or protocol for debridement or surgical excision has been established.
In conclusion, a rural or agricultural lifestyle may contribute to an increased risk of P. lilacinum infection in immunocompetent individuals. Here we reported a rare case of such an infection and provided a literature review of deep cutaneous fungal infection by P. lilacinum in immunocompetent patients.
The patient provided written informed consent for the publication and the use of his or her images.
References
1. Pastor FJ, Guarro J. Clinical manifestations, treatment and outcome of Paecilomyces lilacinus infections. Clin Microbiol Infect 2006;12:948-960
Google Scholar
2. Castro LG, Salebian A, Sotto MN. Hyalohyphomycosis by Paecilomyces lilacinus in a renal transplant patient and a review of human Paecilomyces species infections. J Med Vet Mycol 1990;28:15-26
Google Scholar
3. Samson RA. Paecilomyces and some allied hyphomycetes. Stud Mycol 1974;6:58
Google Scholar
4. Polat M, Kara SS, Tapisiz A, Demirtas Z, Sari S, Kalkanci A, et al. Successful treatment of Paecilomyces variotii peritonitis in a liver transplant patient. Mycopathologia 2015; 179:317-320
Google Scholar
5. Steiner B, Aquino VR, Paz AA, Silla LM, Szvascki A, Goldani LZ. Paecilomyces variotii as an emergent pathogenic agent of pneumonia. Case Rep Infect Dis 2013;2013:273848
Google Scholar
6. Vasudevan B, Hazra N, Verma R, Srinivas V, Vijendran P, Badad A. First reported case of subcutaneous hyalohyphomycosis caused by Paecilomyces variotii. Int J Dermatol 2013;52:711-713
Google Scholar
7. Marchese SM, Smoller BR. Cutaneous Paecilomyces lilacinus infection in a hospitalized patient taking corticosteroids. Int J Dermatol 1998;37:438-441
Google Scholar
8. Hall VC, Goyal S, Davis MD, Walsh JS. Cutaneous hyalohyphomycosis caused by Paecilomyces lilacinus: report of three cases and review of the literature. Int J Dermatol 2004;43:648-653
Google Scholar
9. Itin PH, Frei R, Lautenschlaqer S, Buechner SA, Surber C, Gratwohl A, et al. Cutaneous manifestations of Paecilomyces lilacinus infection induced by a contaminated skin lotion in patients who are severely immunosuppressed. J Am Acad Dermatol 1998;39:401-409
Google Scholar
10. Bainer G. Mycotheque de l'edole de pharmacie IX. Paecilomyces, genre nouveau de mucedinees. Bull Soc Mycol Fr 1907;23:26-27, Cited from Kwon-Chung KJ, Bennett JE. Medical mycology. Philadelphia: Lea & Febiger, 1992: 747-750
11. Luangsa-Ard J, Houbraken J, van Doorn T, Hong SB, Borman AM, Hywel-Jones NL, et al. Purpureocillium, a new genus for the medically important Paecilomyces lilacinus. FEMS Microbiol Lett 2011;321:141-149
Google Scholar
12. Fenech FF, Millia CP. Pleural effusion caused by Penicillium lilacinus. Br J Dis Chest 1972;66:284-290
Google Scholar
13. Blackwell V, Ahmed K, O'Docherty C, Hay RJ. Cutaneous hyalohyphomycosis caused by Paecilomyces lilacinus in a renal transplant patient. Br J Dermatol 2000;143:873-875
Google Scholar
14. Jung MY, Park HJ, Lee JH, Lee JH, Yang JM, Lee DY. A localized cutaneous Paecilomyces lilacinus infection treated with voriconazole. Korean J Dermatol 2013;51:833-836
Google Scholar
15. Kwak H, Park SK, Yun SK, Kim HU, Park J. A case of localized skin infection due to Purpureocillium lilacinum. Korean J Med Mycol 2017;22:42-49
Google Scholar
16. Saghrouni F, Saidi W, Ben Said Z, Gheith S, Ben Said M, Ranque S, et al. Cutaneous hyalohyphomycosis caused by Purpureocillium lilacinum in an immunocompetent patient: case report and review. Med Mycol 2013;51:664-668
Google Scholar
17. Ko WT, Kim SH, Suh MK, Ha GY, Kim JR. A case of localized skin infection due to Paecilomyces lilacinus. Korean J dermatol 2007;45:930-933
Google Scholar
18. Nagamoto E, Fujisawa A, Yoshino Y, Yoshitsugu K, Odo M, Watanabe H, et al. Case of Paecilomyces lilacinus infection occurring in necrotizing fasciitis-associated skin ulcers on the face and surrounding a tracheotomy stoma. Med Mycol J 2014;55:E21-27
Google Scholar
19. Aguilar C, Pujol I, Sala J, Guarro J. Antifungal susceptibilities of Paecilomyces species. Antimicrob Agents Chemother 1998;42:1601-1604
Google Scholar
20. Castelli MV, Alastruey-Izquierdo A, Cuesta I, Monzon A, Mellado E, Rodriguez-Tudela JL, et al. Susceptibility testing and molecular classification of Paecilomyces spp. Antimicrob Agents Chemother 2008;52:2926-2928
Google Scholar
Congratulatory MessageClick here!
