pISSN : 3058-423X eISSN: 3058-4302
Open Access, Peer-reviewed
pISSN : 3058-423X eISSN: 3058-4302
Open Access, Peer-reviewed

Jun Suk Hong,Dong Won Lee,Moo Kyu Suh,Gyoung Yim Ha,Tae Jung Jang,Jong Soo Choi
10.17966/JMI.2019.24.1.32 Epub 2019 March 28
Abstract
Keywords
Nummular dermatitis Tinea corporis Trichophyton verrucosum
Many skin conditions present as cutaneous annular lesions, thereby complicating the diagnosis based on the physical appearance alone1. As a typical example of annular lesions, nummular dermatitis presents as well-demarcated coin-shaped annular plaques formed from coalescing papules and papulovesicles. Another example of annular lesions is seen in tinea corporis, which is a superficial dermatophyte infection that can occur on any cutaneous surface, except the hands, feet, scalp, or groin; it presents as an erythematous annular plaque with a scaly, centrifugally advancing border1,2. The presentations of nummular dermatitis and tinea corporis are so similar that tinea corporis is often mistaken for nummular dermatitis, and a potassium hydroxide (KOH) preparation of the skin scrapings may help distinguish between the two conditions1. However, in atypical manifestations of tinea corporis, such as vesiculopustular lesion, the accurate diagnosis can be missed because the clinical signs and symptoms of tinea corporis are neither sensitive nor specific for dermatophytosis2,3. In particular, cutaneous lesions caused by Trichophyton verrucosum, which is the most common causative pathogen of dermatophytosis in cattle, are usually characterized clinically by intense inflammation because of which these lesions are often misdiagnosed as eczema4,5. Besides, in atypical cases of tinea corporis, the diagnosis can be even missed by false negative results from KOH analysis or culture. In such cases, definitive diagnosis can easily be confirmed histologically on the basis of the presence of PAS-positive fungi in the stratum corneum or hair follicle2.
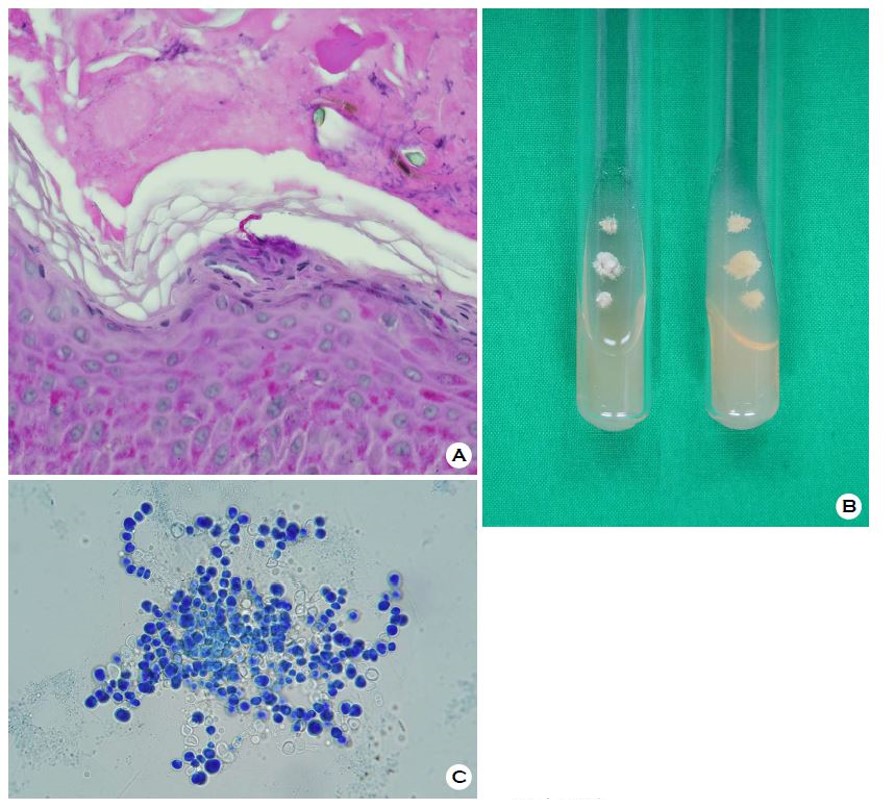
A 58-year-old female cattle keeper presented with a solitary, pruritic, 3.0 × 3.0-cm sized erythematous annular plaque with central clearing and a vesicular border on the left upper arm at one month after its emergence (Figure 1). The results of KOH examination on the left upper arm lesion were negative. Therefore, we cultured and performed a biopsy for a definitive diagnosis. Histopathological analysis revealed short septate hyphae in the stratum corneum (Figure 2A). Cultures from skin biopsy specimens on Sabouraud's dextrose agar yielded slow-growing, folded, heaped, glabrous, and white colonies, which lacked pigments in the reverse side after 6 weeks (Figure 2B). Chains of chlamydoconidia were observed in the slide culture on microscopic examination (Figure 2C). The nucleotide sequence of the internal transcribed spacer of the clinical isolate was identical to that of T. verrucosum strain CBS 562.50 (GenBank accession number MH856755). The patient was treated with 100 mg of oral itraconazole daily for 1 month, and the skin lesion improved completely.

We diagnosed tinea corporis caused by T. verrucosum mimicking nummular dermatitis on the basis of clinical findings, pathological findings, fungal culture, and molecular biological analysis. We have reported this case to emphasize the importance of fungal culture and histopathological examination for accurate diagnosis in atypical and difficult cases.
References
1. Trayes KP, Savage K, Studdiford JS. Annular lesions: diag nosis and treatment. Am Fam Physician 2018;98:283-291
Crossref
Google Scholar
PubMed
2. Ziemer M, Seyfarth F, Elsner P, Hipler UC. Atypical manifestations of tinea corporis. Mycoses 2007;50 Suppl 2: 31-35
Crossref
Google Scholar
3. Kelly BP. Superficial fungal infections. Pediatr Rev 2012; 33:e22-37
Crossref
PubMed
4. Roman C, Massai L, Gianni C, Crosti C. Case reports. six cases of infection due to Trichophyton verrucosum. Mycoses 2001;44:334-337
Crossref
Google Scholar
PubMed
5. Hong JS, Lee DW, Suh MK, Ha GY. Macroscopic and microscopic findings of Trichophyton verrucosum isolated from cattle. J Mycol Infect 2018;23:118-119
Crossref
Google Scholar
Congratulatory MessageClick here!
