pISSN : 3058-423X eISSN: 3058-4302
Open Access, Peer-reviewed
pISSN : 3058-423X eISSN: 3058-4302
Open Access, Peer-reviewed

Adil Maleb,Aziza Hami,Yassine Ben Lahlou, Somiya Lamrabat,Safaa Rifai,Nawal Rahmani,Mohammed Bensalah,Mohammed Frikh,Abdelhay Lemnouer,Mostafa Elouennass
10.17966/JMI.2019.24.1.28 Epub 2019 March 28
Abstract
Disseminated cryptococcosis is a rare fungal infection, which mainly occurs in immunocompromised patients, and the diagnosis is difficult. Therefore, it is less likely to be considered in immunocompetent patients. Here, we present a case of fatal cryptococcal infection of the pleural fluid and ascites in a patient seronegative for HIV. The patient was a 45-year old man who was followed for Crohn's disease and treated with steroids and an immunosuppressant (azathioprine). The culture of pleural and ascites fluids showed the presence of yeasts colonies identified as Cryptococcus neoformans. Bacteriological examination of the blood culture or cerebrospinal fluid (CSF) was not prescribed. The HIV serology was negative. At the fourth day of treatment, the patient died because of the deterioration of neurological and hepatocellular functions. The main diagnostic problems that led to this fatal outcome were non-suspicion of an at-risk patient, lack of microbiological analysis of the blood or CSF, and inadequate antifungal therapy.
Keywords
Ascites Cryptococcus neoformans Pleura
Disseminated cryptococcosis is a rare fungal infection caused by a capsulated yeast of the Cryptococcus genus, which mainly occurs in immunocompromised patients, and is fatal1. Thus, it is easily considered, and the diagnosis is relatively easy in these patients. However, in immunocompetent patients, the diagnosis is more difficult. Therefore, it is less likely to be considered, which can lead to delays in therapy initiation, directly influencing the prognosis2. We present a case of fatal cryptococcal infection of the pleural fluid and ascites in a patient seronegative for HIV, followed for Crohn's disease. The objective of this case study is to demonstrate the main pitfalls of clinical and microbiological diagnosis that darken the prognosis of this infection.
A 45-year old man was followed for Crohn's disease, with the complications of splenic thrombosis and duodeno-jejunal stenosis. The patient was treated with steroids and then with an immunosuppressant (azathioprine). The patient was hospitalized for shock and diagnosed with hypovolemic shock state on diarrhea, with the abundance of ascites. The clinical examination revealed a conscious patient of 55 kg, feverish (38℃), having an arterial tension of 75/35 mm Hg, heart rate of 112/min, and respiratory rate of 25 breaths/min. The abdominal examination showed a distended abdomen with collateral venous circulation. The patient had dehydration folds and cold extremities with oliguria, but no meningeal or cutaneous signs.
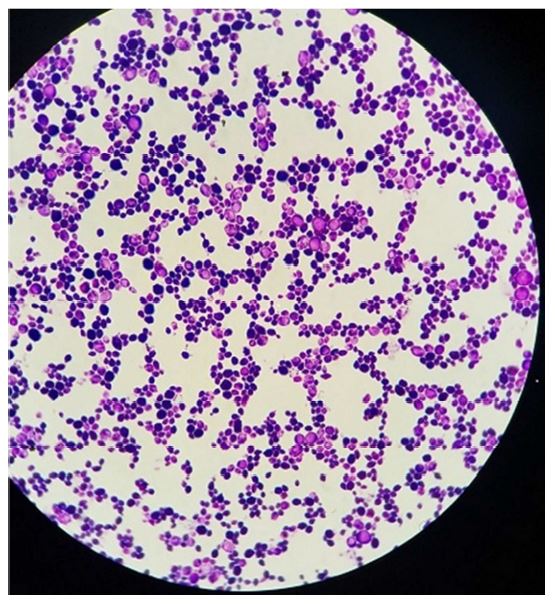
Biological examinations on day 1 revealed CRP levels of 161 mg/L, leukocytes at 5,400 elements/mm3 with 95% of neutrophils and 2% of lymphocytes, and hemoglobin at 9.2 g/dL. On day 2, the ascites examination revealed 243 leucocytes/ mm3, predominantly lymphocytes (93%). Direct examination after Gram staining of ascites fluid revealed the presence of budding yeasts. On day 4, the culture of ascites fluid after two days of incubation on Sabouraud's media showed the presence of yeasts colonies (Figure 1), identified using BD Phoenix100 yeast ID panel (Becton Dickinson Diagnostics, USA) as Cryptococcus neoformans at 99.99% confidence. Immunohistochemical stains, such as Grocott-Gomori's methenamine silver stain, periodic acid-Schiff stain, or mucicarmine stain, were not used. Fever associated with diffuse interstitial lung disease and bilateral pleural effusion on computed tomography indicated a cytobacteriological examination of the pleural fluid. On day 5, the cytology of the pleural fluid revealed leukocytes at 2,420 elements/mm3 with lymphocyte predominance (65%). On day 7, the pleural fluid was cultured on chocolate agar media in the presence of CO2 and anaerobic atmosphere. The culture was positive, allowing for the isolation of Cryptococcus neoformans. Sabouraud's media supplemented with actidione was used for this culture as well for the liquid of ascites and the pleural fluid. It remained sterile after 5 days of incubation for both liquids. Lumbar puncture was contraindicated because of the bleeding risk (prothrombin time at 29%). Bacteriological examination of the blood culture or cerebrospinal fluid (CSF) was not prescribed for the patient, and the HIV serology was negative. On day 4, fluconazole was immediately administered intravenously at the dose of 800 mg/day. At the fourth day of treatment (day 8), the patient died because of the deterioration of neurological and hepatocellular functions. No autopsy was performed to clarify the cause of death. The deceased patient's dependents gave consent to our use of the anonymized patient data.
Cryptococcosis is a serious infection caused by the encapsulated yeast Cryptococcus neoformans. It is a ubiquitous fungus isolated from the soil and pigeon droppings3. The direct relationship between pigeon droppings and Cryptococcus infection in the present case has not been established. Indeed, the multiplicity of possible sources, especially in an urban environment, makes the accurate determination of the source nearly impossible4. The portal of entry of this fungus is pulmonary, and the dissemination of the infection is via the blood4-7, which is likely the case in our patient. The prevalence of exposure to Cryptococcus neoformans is high worldwide because 80% of subjects have anti-C. neoformans antibodies. However, the disease is relatively rare8. The most common manifestation of this fungal infection is the involvement of the central nervous system in the form of sub-acute or chronic meningitis or cerebral cryptococcomas in rarer cases7. However, cryptococcosis is a severe opportunistic infection, which could affect several organs9. Ascites of cryptococcal origin is rare. Only 62 cases have been described in the literature10,11. Pulmonary involvement usually consists of granulomatous and infiltrated reactions, similar to that in the present case12. Cryptococcal pleural effusions are rare13. Cryptococcosis mainly develops in subjects with a deficiency in the cell-mediated immunity9. Therefore, patients with AIDS are at a higher risk of infection, but other conditions might predispose the patients to cryptococcosis, such as immunosuppression, corticosteroids, diabetes, cirrhosis, chronic leukemia and lymphoma7,10,14,15. As for our propositus, in the cases described in Crohn's disease, immunosuppressants and corticosteroids are thought to be the contributing factors to the infection and not Crohn's disease itself15.
The diagnosis of cryptococcosis is based on the demonstration and direct examination of a specific encapsulated yeast of genus Cryptococcus. The culture on Sabouraud's medium without actidione is essential for the identification of the species16,17. As is the case in our patient, the diagnosis based on the detection of Cryptococcus on the culture of ascites fluid is delayed (average, 6 days). Therefore, 50% of cases are diagnosed post mortem17. Extra meningeal localizations of C. neoformans are rarely isolated, and systematic search must be encouraged for the spread of this yeast, especially at the meninges, even in the absence of neurological signs (systematic prescription of a cytobacteriological examination of the CSF in front of any form extrameningeal cryptococcosis)18. The blood cultures are of great interest in the diagnosis of disseminated cryptococcosis because they are positive in 30% cases11. The diagnosis would have been made earlier if our patient had been prescribed blood cultures in adapted culture media.
Disseminated cryptococcosis is an emergency situation that requires aggressive antifungal treatment19. The treatment conventionally uses amphotericin B (0.7 mg/kg/day) with or without 5-fluorocytosine (100 mg/kg/day) for 15 days. The relay is fluconazole 400 mg/day for 6~10 weeks and 200 mg/ day for maintenance17,20. The treatment provided to our patient was insufficient (fluconazole alone). Despite well-managed medical treatment, the treatment failure rate for disseminated cryptococcal disease is 20%8,21.
Disseminated cryptococcosis is a rare and serious fungal infection, which can be fatal because of the vital organs it affects, delayed diagnosis, and possibility of therapeutic failure. To improve its prognosis, the triad "clinical suspicion in subjects at-risk, early and correct diagnosis, early and well-guided antifungal treatment" must be followed.
References
1. Singh N, Husain S, De Vera M, Gayowski T, Cacciarelli TV. Cryptococcus neoformans infection in patients with cirrhosis, including liver transplant candidates. Medicine (Baltimore) 2004;83:188-192
Crossref
Google Scholar
2. El Ouazzani H, Achachi L, Belkhiri S, El Ftouh M, El Fassy Fihry MT. Cryptococcose disséminée chez un sujet apparemment immunocompétent. Rev Mal Respir 2009;26: 788-793
Crossref
Google Scholar
PubMed
3. Ward C. Prejudice against women: Who, when, and why? Sex Roles 1981;7:163-171
Crossref
Google Scholar
4. Charra B, Hachimi A, Nejmi H, Sodqi M, Benslama A, Motaouakkil S. Cryptococcose neuroméningée chez un sujet immunocompétent. Med Mal Infect 2005;35:549 -551
Crossref
Google Scholar
PubMed
5. Yoo SS, Tran M, Anhalt G, Barrett T, Vonderheid EC. Disseminated cellulitic cryptococcosis in the setting of prednisone monotherapy for pemphigus vulgaris. J Dermatol 2003;30:405-410
Crossref
Google Scholar
PubMed
6. Revest M, Decaux O, Frouget T, Cazalets C, Albert JD, Chevrier S, et al. Infections à cryptocoque chez des patients non VIH. À propos de quatre cas et revue de la littérature. Rev Med Interne 2006;27:203-208
Crossref
Google Scholar
PubMed
7. Albert-Braun S, Venema F, Bausch J, Hunfeld KP, Schäfer V. Cryptococcus neoformans peritonitis in a patient with alcoholic cirrhosis: Case report and review of the literature. Infection 2005;33:282-288
Crossref
Google Scholar
8. Aubry P. Mycoses profondes. Med Trop 2014;1-17
Crossref
9. Minta DK, Traoré AM, Coulibaly I, Diallo K, Soukho-Kaya A, Dolo A, et al. Cryptococcose extra-neuroméningée au cours du sida à Bamako, Mali (à propos de 2observations). J Mycol Med 2014;24:e65-e71
Crossref
Google Scholar
PubMed
10. Prieux-Klotz C, Larréché S, Delaune D, Sinayoko L, Corberand D, Ficko C. Cryptococcose disséminée révélée par une infection du liquide d'ascite. Vol. 46, Med Mal Infect 2016;46:456-457
Crossref
Google Scholar
PubMed
11. El-Kersh K, Rawasia WF, Chaddha U, Guardiola J. Rarity revisited: Cryptococcal peritonitis. BMJ Case Rep 2013
Crossref
Google Scholar
PubMed
12. Huston SM, Mody CH. Cryptococcosis: An emerging respiratory mycosis. Clin Chest Med 2009;30:253-264
Crossref
Google Scholar
PubMed
13. Kamiya H, Ishikawa R, Moriya A, Arai A, Morimoto K, Ando T, et al. Disseminated cryptococcosis complicated with bilateral pleural effusion and ascites during corticosteroid therapy for organizing pneumonia with myelodysplastic syndrome. Intern Med 2008;47:1981-1986
Crossref
Google Scholar
14. Diamond RD, Bennett JE. Disseminated cryptococcosis in man: Decreased lymphocyte transformation in response to Cryptococcus neoformans. J Infect Dis 1973;127:694 -697
Crossref
Google Scholar
15. Osawa R, Singh N. Colitis as a manifestation of infliximab-associated disseminated cryptococcosis. Int J Infect Dis 2010;14:e436-440
Crossref
Google Scholar
16. Ehui E, Eholie SP, Kakou A, Gbery I, Diomande IM, Adou¬Bryn KD, et al. Cryptococcose disséminée révélée par une atteinte cutanée au cours du SIDA (French). Disseminated cryptococcosis reveal by cutaneous manifestations course AIDS. J Mycol Med 2010;10:97-109
Crossref
17. Jarvis JN, Harrison TS. Pulmonary cryptococcosis. Semin Respir Crit Care Med 2008;29:141-150
Crossref
PubMed
18. Carter EA, Henderson DW, McBride J, Sage MR. Case report: Complete lung collapse - An unusual presentation of cryptococcosis. Clin Radiol 1992;46:292-294
Crossref
Google Scholar
PubMed
19. Ammouri W, Harmouche H, Afifi Y, Tazi Mezalek Z, Adnaoui M, Aouni M, et al. A case of disseminated cryptococcosis complicating treatment of pemphigus vulgaris with prednisone and azathioprime. Pan Afr Med J 2011;10:35
Crossref
20. Brouwer AE, Rajanuwong A, Chierakul W, Griffin GE, Larsen RA, White NJ, et al. Combination antifungal therapies for HIV-associated cryptococcal meningitis: A randomised trial. Lancet 2004;363:1764-1767
Crossref
Google Scholar
21. Elavsky CM, Mislan C, Elavsky S. When talking less is more: Exploring outcomes of Twitter usage in the large-lecture hall. Learn Media Technol 2011;36:215-233
Crossref
Google Scholar
Congratulatory MessageClick here!
