pISSN : 3058-423X eISSN: 3058-4302
Open Access, Peer-reviewed
pISSN : 3058-423X eISSN: 3058-4302
Open Access, Peer-reviewed

Min Kyun An,Ji Ha Yoon,Eun Byul Cho,Eun Joo Park,Kwang Ho Kim
10.17966/JMI.2018.23.4.111 Epub 2019 January 02
Abstract
A 19-year-old woman presented with an asymptomatic cutaneous discoloration on her nape. Dermatological examination revealed localized dark brown to dark pigmented velvety macules and patches. She denied a past medical history, except for a 7-kg weight gain over a 6-months period. Histopathologically, the specimen showed hyperkeratosis, epidermal hyperplasia, mild acanthosis, and papillomatosis. In addition, keratin material and fungal spore were noted between the papilloma ridges. Periodic acid-Schiff special stain showed a positive result for the fungal spore in the horny layer. She was treated with a daily oral dose of terbinafine and topical flutrimazole. After 12 weeks of treatment, she is currently under observation without pigmentation and adverse effect. We considered the initial diagnosis as acanthosis nigricans because of weight gain, similar clinical features, and histological findings. However, the final diagnosis was hyperkeratotic head and neck Malassezia dermatosis considering the presence of yeast and the dramatic improvement after antifungal treatment. To the best of our knowledge, hyperkeratotic head and neck Malassezia dermatosis is not well characterized in the literature. It is an unusual variant of pityriasis versicolor. The skin lesion appears brown to dark, scaly, and hyperkeratotic macules and patches located on the face and neck. Here, we reported an unusual case of hyperkeratotic head and neck Malassezia dermatosis.
Keywords
Acanthosis nigricans Fungal spore Hyperkeratotic head and neck Malassezia dermatosis Malassezia species
Hyperkeratotic head and neck Malassezia dermatosis (HHNMD) was the first disease condition reported by Boralevi et al.1 Clinical features of HHNMD include scaly hyperkeratotic dermatosis involving the face and neck. Examination of the skin lesion revealed Malassezia colonization. Clinical manifestations of acanthosis nigricans (AN) are systemic hyperpigmented, hyperkeratotic, and verrucous velvet-like patches and plaques. It mainly occurs in the intertriginous areas, such as the axilla, posterior neck, and genital area. AN develops because of several different causes, and it can be classified into eight subtypes, namely malignant-associated, benign, acral, obesity-associated, syndromic, drug-induced, unilateral, and mixed2. AN is more commonly associated with insulin resistance or obesity. To the best of our knowledge, no cases of AN-associated fungal infection have yet been reported. Here we reported a case of HHNMD caused by yeast infection presenting with AN.
A 19-year-old woman presented with asymptomatic cutaneous discoloration. A dermatological examination revealed localized dark brown to dark pigmented velvety macules and patches on the nape (Figure 1A). No pruritus or pain was detected in the skin lesions. She denied any medical history except for a 7-kg weight gain over the past 6 months. Her grandfather has diabetes, but there is no familial history of AN. Laboratory results were positive with fluorescent antinuclear antibody¬speckled pattern, and all findings, including blood sugar test and HbA1c levels, were normal.

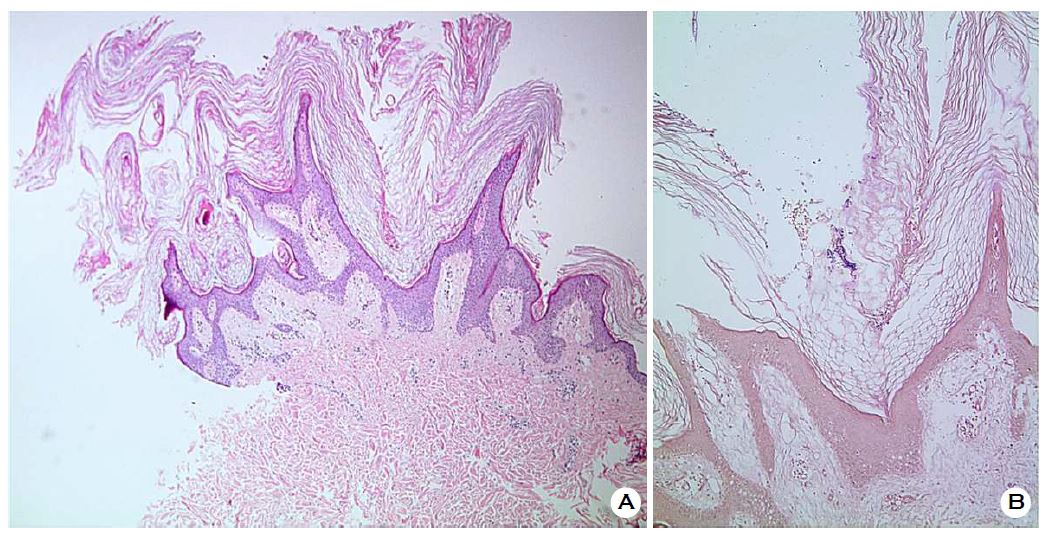
A skin punch biopsy was performed to differentiate among HHNMD, confluent and reticulated papillomatosis, and AN. Histopathologically, the specimen revealed hyperkeratosis, a thinned epidermis above papillomatous projection, mild acanthosis, and an upward finger-like projection of dermal papillae (Figure 2A). Keratin material and fungal spores were detected between the papilloma ridges. The upper dermis revealed mild perivascular lymphocytic infiltration. No other specific findings were observed in the dermis. Periodic acid-Schiff (PAS) staining revealed a positive result for fungal spores in the horny layer (Figure 2B).
AN and HHNMD were not excluded based on clinical and histological findings. The initial treatment was performed with 250 mg terbinafine and 1% topical flutrimazole cream daily. After 3 weeks, the velvety pigmented patches improved. After 12 weeks of continuous treatment, the symptoms disappeared, leaving no residual pigmentation and without any adverse effect (Figure 1B). Considering the dramatically improved skin lesions after antifungal treatment, HHNMD was considered as the final diagnosis. She is currently undergoing observation without any special treatment.
HHNMD is a rare cutaneous infection caused by Malassezia. Until date, there have been only two reports on HHNMD1,3. Boralevi et al.1 confirmed Malassezia species in the fungal culture and considered it an unusual variant of pityriasis versicolor (PV) based on clinical features in adolescents and young adults. Pham-Ledard et al.3 inferred it to be a facial presentation of confluent and reticulated papillomatosis (CRP) based on clinical features of brown, scaly, hyperkeratotic macules, and patches.
Histological features of PV are characterized by slight hyperkeratosis, slight spongiosis, and minimal perivascular lymphocytic infiltration4. CRP is characterized by mild hyperkeratosis, papillomatosis, and focal acanthosis5. Histological findings of this case showed significant hyperkeratosis, thinned epidermis at the tips and sides of protruding dermal papillae, and upward projection of the dermal papillae. Therefore, PV and CRP were excluded.
This case showed weight gain, typical skin appearance of AN, and histological findings. However, fungal spores were observed with the keratin material between the hyperkeratotic ridges. No cases of cutaneous fungal infection have yet been reported. The response to treatment of AN is extremely poor. However, this case was treated, and dramatically hyperkeratotic scaly hyperpigmentation of the skin was observed after anti- fungal treatment. Although we did not conduct any evaluation, such as fungal culture or genomic sequencing, the cutaneous infection of Malassezia yeast was the most suspected based on the observed fungal spores. The epidermal stripping or scrapping, performed before the skin punch biopsy, could exclude terra firma forme dermatosis but not the skin lesion. The stable psychological status and willingness for therapy excluded the possibility of dermatitis neglecta. These clinical features and histological findings suggest that the final diagnosis was more appropriate for HHNMD than for AN.
Cutaneous changes in AN are caused by growth factor stimulation of keratinocytes and dermal fibrosis of the skin, and hyperpigmentation is caused by epidermal hyperkeratosis2. Tamraz et al.6 reviewed 10 cases of CRP and observed Malassezia yeast in six, which demonstrated clinicopathological hyperpigmentation and hyperkeratosis similar to that in HHNMD. In CRP, an abnormal keratinizing response to Malassezia has been hypothesized to underlying pathological keratinization6. We believe that hyperkeratosis in HHNMD is similar to that in CRP, considering the improper response of keratinocytes to fungal spores. Histological findings of this case also demonstrated a significant increase in hyperkeratosis but not in melanin pigmentation. Histological findings of the two cases reported by Boralevi et al.1 showed no increase in melanin pigmentation. Thus, hyperpigmentation of HHNMD is believed to occur due to hyperkeratosis rather than due to an increase in melanin pigmentation.
In this case, additional evaluations, such as fungus culture, were not performed to identify the pathogen, which is a limitation. Boralevi et al.1, who first reported HHNMD, reported HHNMD as a variant form of PV. Pham-Ledard et al.3 considered HHNMD as a facial presentation of CRP with contingent yeast colonization. Considering the lack of reports on HHNMD, it remains controversial to consider HHNMD as an independent disease entity.
Antifungal agents should be considered as the first-line treatment for HHNMD. Boralevi et al.1 confirmed Malassezia globosa and M. sympodialis as causative agents in two cases. A 26-year-old man, treated with oral ketoconazole and imidazole cream, improved after 6 months of treatment. A 42-year-old woman was treated with oral and topical ketoconazole as well as 1% salicylic acid topical ointment, and the skin lesion improved after 1 month of treatment. In this case, the patient was also treated with oral terbinafine and topical flutrimazole for approximately 12 weeks.
These antifungal agents may be helpful not only for the direct treatment of Malassezia yeast but also for hyperkeratosis —the cause of hyperpigmentation. Ketoconazole exerts an anti-inflammatory effect through the inhibition of the arachidonic acid cascade7 and directly acts on a somatomedin C/insulin-like growth factor I receptor to reduce keratinocyte replication8. Until date, no studies have reported that terbinafine and flutrimazole reduce human keratinocyte proliferation; however, terbinafine is commonly used for the treatment of seborrheic dermatitis in Malassezia infection9. The effect of terbinafine can be attributed to the combination of its antifungal activity against Malassezia yeasts and its anti-inflammatory activity9. Topical flutrimazole has demonstrated an anti-inflammatory effect in animal studies, which reduces edema by targeting arachidonic acid10.
In the present case, we demonstrated that HHNMD presenting with AN can be effectively and safely treated with antifungals. The improvement in pigmentation can be explained by the elimination of Malassezia yeast. The authors believe that antifungal agents are effective for the treatment of hyperkeratosis. Therefore, we hypothesized that cutaneous fungal infection is associated with hyperkeratosis and hyperpigmentation. Therefore, the antifungal agents could be considered as keratolytics in patient.
In relation to this article, We declare that there is no conflict of interest.
References
1. Boralevi F, Marco-Bonnet J, Lepreux S, Buzenet C, Couprie B, Taïeb A. Hyperkeratotic head and neck Malassezia dermatosis. Dermatology 2006;212:36-40
Crossref
Google Scholar
PubMed
2. Sinha S, Schwartz RA. Juvenile acanthosis nigricans. J Am Acad Dermatol 2007;57:502-508
Crossref
Google Scholar
PubMed
3. Pham-Ledard A, Ezzedine K, Couprie B, Begueret H, Boralevi F, Taieb A. Facial confluent and reticulate papillomatosis (Gougerot-Carteaud syndrome) or hyperkeratotic head and neck Malassezia dermatitis? Ann Dermatol Venereol 2010;137:451-454
Crossref
Google Scholar
PubMed
4. Elder DE. Lever's histopathology of the skin. Lippincott Williams & Wilkins, 2014:732
Crossref
5. Park YJ, Kang HY, Lee ES, Kim YC. Differentiating confluent and reticulated papillomatosis from acanthosis nigricans. J Cutan Pathol 2015;42:944-952
Crossref
Google Scholar
6. Tamraz H, Raffoul M, Kurban M, Kibbi AG, Abbas O. Confluent and reticulated papillomatosis: clinical and histopathological study of 10 cases from Lebanon. J Eur Dermatol Venereol 2013;27:e119-123
Crossref
7. Cutsem JV, van Gerven F, Cauwenbergh G, Odds F, Janssen PAJ. The antiiflammatory effects of ketoconazole. J Am Acad Dermatol 1991;25:257-261
Crossref
PubMed
8. Nickoloff BJ, Misra P, Morhenn VB, Hintz RL, Rosenfeld RG. Further characterization of the keratinocyte somatomedin-C/insulin-like growth factor I (SM-C/IGF-I) receptor and the biological responsiveness of cultured keratinocytes to SM-C/IGF-I. Dermatologica 1988;177:265-273
Crossref
Google Scholar
9. Faergemann J. Treatment of seborrhoeic dermatitis with oral terbinafine? Lancet 2001;358:170
Crossref
Google Scholar
PubMed
10. Merlos M, Vericat ML, Garcia-Rafanell J, Forn J. Topical anti-inflammatory properties of flutrimazole, a new imidazole antifungal agent. Infalmm Res 1996;45:20-25
Crossref
Google Scholar
Congratulatory MessageClick here!
