pISSN : 3058-423X eISSN: 3058-4302
Open Access, Peer-reviewed
pISSN : 3058-423X eISSN: 3058-4302
Open Access, Peer-reviewed

Yee-Hyuk Kim
10.17966/JMI.2018.23.4.105 Epub 2019 January 02
Abstract
Background: Otomycosis is a fungal infection that comprises 7~10% of outer ear infections. Although the occurrence is higher in humid climates, relatively few studies have investigated otomycosis occurrences in humid environments. While recurrent chronic otitis media discharge in the ear creates a milieu in which otomycosis is likely to occur, investigations of otomycosis co-occurring with chronic otitis media have been rare.
Objective: To examine the characteristics of patients with otomycosis co-occurring with chronic otitis media and identify causative fungi.
Methods: The study included 60 patients with chronic otitis media who presented typical otomycosis findings in the outer ear canal and the presence of fungi. Patients were treated in the department of otolaryngology, Daegu Catholic University Medical Center, between July 2011 and June 2018.
Results: The mean patient age was 57.77 years, and our study included 20 men and 40 women (p=0.010). The lesion was on the right in 39 patients and on the left in 21 (p=0.020). Ear discharge was the most common chief complaint at diagnosis. Of the 54 patients over age 19, 10 had diabetes (18.5%). Aspergillus was causative in 29 patients and Candida in 31. Aspergillus niger was identified in 15 patients, Aspergillus sp. in 14, Candida parapsilosis in 12, Candida sp. in six, and Candida albicans in five.
Conclusion: Otomycosis and chronic otitis media co-occurrences increase with age. The Aspergillus and Candida genera were similar in proportion. A. niger was the most common Aspergillus species, while C. parapsilosis was the most common Candida.
Keywords
Aspergillus Candida Fungi Otitis media Otomycosis
Otomycosis is a fungal infection in the outer ear1,2, comprising 7~10% of all outer ear infections1,3,4. However, the occurrence has been reported to be as high as 30~47% in tropical areas with high humidity5,6. Otomycosis is frequently encountered in outpatient clinics, but relatively little research has been conducted on this disease. Although recurrent dis- charge in the ear due to chronic otitis media creates an environment that is favorable for otomycosis, little is known about the co-occurrence of this disease with chronic conditions. The present study examined the characteristics of patients with otomycosis co-occurring with chronic otitis media and identifies causative fungi.
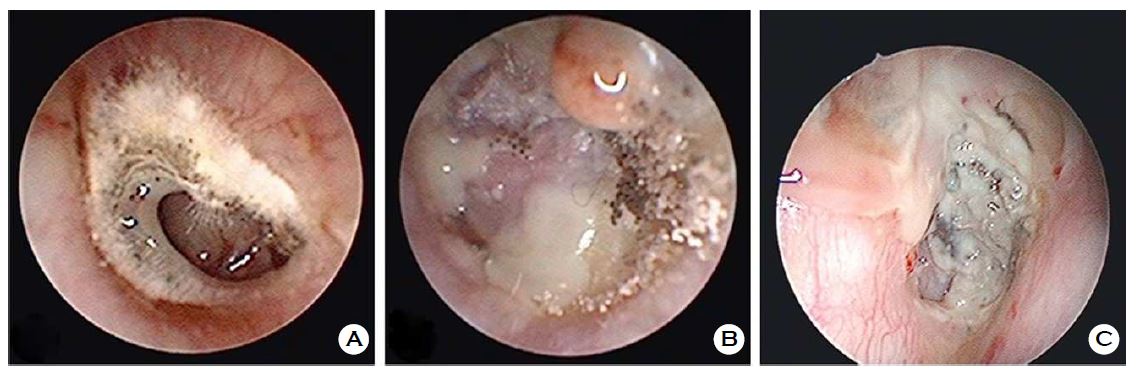
The study included patients in whom typical endoscopic otomycosis findings were observed in the outer ear canal of ears with chronic otitis media, and the presence of fungi was confirmed on a fungal culture test. Typical otomycosis findings in the outer ear canal include white fluff or cotton-like appearance7-10 (Figure 1A), pepper-like appearance7,8,11 (Figure 1B), and wet newspaper appearance9,11 (Figure 1C). The fungus was cultured by injecting the specimen from the outer ear canal onto Sabouraud's dextrose agar and cultivating the sample at 37℃ for one day followed by 30℃ for seven days. Fungal identification was conducted on the fungal colonies by a visual inspection of the colony pattern, microscopic findings, and analyzing the biochemical characteristics of the fungi. The medical records of 60 patients with chronic otitis media (among those treated in the department of otolaryngology, Daegu Catholic University Medical Center between July 2011 and June 2018) who met the conditions mentioned above (the findings in the outer ear canal and the fungal culture test results) were retrospectively examined for age, sex, lesion side, chief complaint at diagnosis, history of diabetes, outer ear canal and eardrum findings, and fungal culture test results. The number of patients per age group was analyzed using a linear regression analysis, and the comparisons of sex, lesion side, and frequency of causative fungi were analyzed with the chi-square test. The statistical analysis was conducted using IBM SPSS Statistics 25.0, and significance level was set at 0.05. A retrospective review was conducted with the approval of the Institutional Review Board of Daegu Catholic University Medical Center (IRB No. CR-18-120).
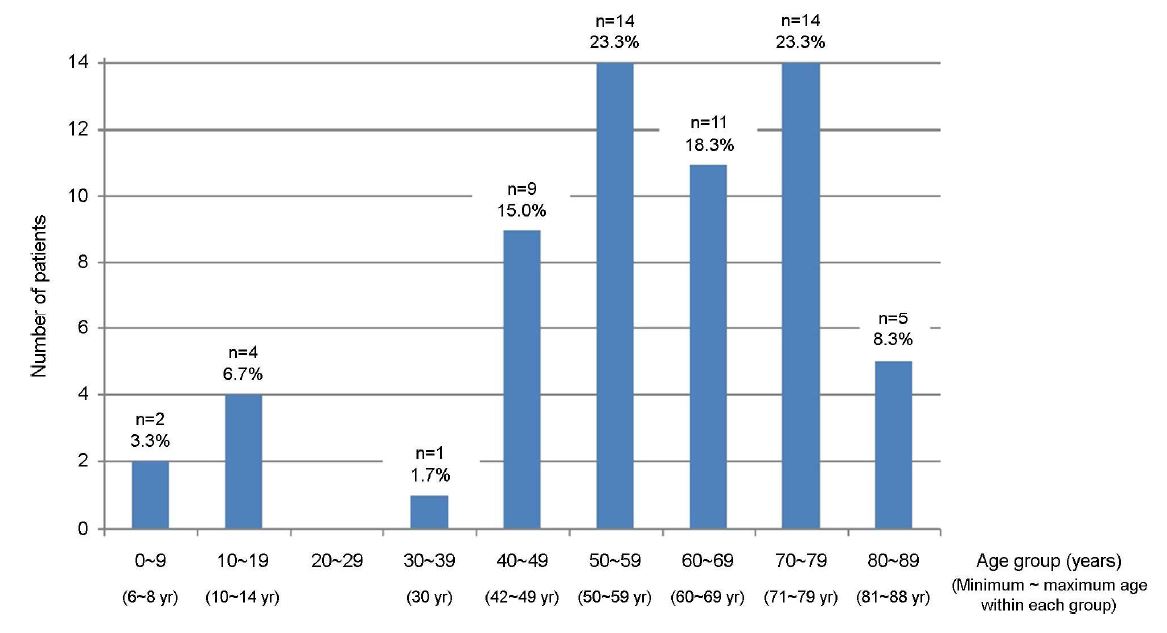
The mean age of the 60 patients who were diagnosed with otomycosis co-occurring with chronic otitis media was 57.77 years (minimum=6, median=59.5, maximum=88, and standard deviation=19.87). The number of patients per age group showed a statistically significant linear increasing trend (p=0.000, R2=0.801) (Figure 2). There were 20 men and 40 women, and the number of women was statistically significantly higher than the number of men (p=0.010). The lesion was on the right in 39 patients and on the left in 21, and the right ear was significantly more commonly affected than the left ear (p=0.020). The analysis of lesion side by sex showed that men did not show a statistically significant difference, though the lesion was on the right ear in 12 and on the left in eight (p=0.371); whereas in women, laterality was statistically significant (27 on the right and 13 on the left; p=0.027) (Table 1). Regarding chief complaints at diagnosis, 38 complained of discharge in the ear, 10 of pain in the ear, 8 of itchiness, and 4 of ear fullness. Of the 54 patients over age 19, 10 had diabetes (18.5%). Regarding causative fungi, the Aspergillus species was found in 29 patients and Candida in 31. Based on the culture test results, Aspergillus niger was identified in 15 patients, Aspergillus sp. in 14, Candida parapsilosis in 12, Candida sp. in 6, Candida albicans in 5, Candida famata and Candida haemulonii in 3 each, and Candida tropicalis in 2 (Table 2).
|
Sex |
Lesion side |
n |
p |
|
Total
(n=60) |
Right |
39 |
0.020* |
|
Left |
21 |
||
|
Men
(n=20) |
Right |
12 |
0.371 |
|
Left |
8 |
||
|
Women
(n=40) |
Right |
27 |
0.027* |
|
Left |
13 |
|
Causative fungus |
n |
p |
|
|
Aspergillus sp. |
14 (23.3%) |
29 |
0.796 |
|
Aspergillus niger |
15 (25.0%) |
||
|
Candida sp. |
6 (10.0%) |
31 |
|
|
Candida albicans |
5 (8.3%) |
||
|
Candida famata |
3 (5.0%) |
||
|
Candida haemulonii |
3 (5.0%) |
||
|
Candida parapsilosis |
12 (20.0%) |
||
|
Candida tropicalis |
2 (3.3%) |
||
|
Total |
60 |
|
|
Several studies have reported that otomycosis is most commonly observed in people in their 20's~40's9,11-14. In contrast, according to a chronic otitis media study conducted in South Korea, the prevalence of the chronic condition shows an increasing trend with age; and specifically, the prevalence rapidly increases in patients in their 40's, compared to earlier ages15. In the present study, which investigated otomycosis co-occurring with chronic otitis media, the number of patients increased with age; and in particular increased rapidly in patients in their 40's. These findings reflect the prevalence of chronic otitis media rather than otomycosis.
Varying results have been reported with respect to the sex prevalence of patients with otomycosis. Statistical results are inconsistent, as some studies have reported a significantly higher proportion of men4,11,12,16,17, others have reported a significantly higher proportion of women18,19, and many have not observed a sex difference1,2,7,8,20-27. In contrast, the chronic otitis media study that was conducted in South Korea found that the prevalence of the condition was 2.77% in men and 3.49% in women, with a statistically higher prevalence in women15. In the present study, which was conducted in patients with otomycosis co-occurring with chronic otitis media, there were twice more women than men. This finding agrees with the results of chronic otitis media prevalence study and does not reflect otomycosis characteristics.
According to a study that was conducted in South Korea, the prevalence of diabetes among adults who are 30 years of age or older 9.9%28. In contrast, the prevalence of diabetes among adults (over age 19) with chronic otitis media has been reported to be 18.19. In present study, no patients were between 15 and 29 years of age, and 18.5% of the participants who were over the age of 19 had diabetes, which is similar to the overall rate among patients with chronic otitis media.
The age distribution, sex ratio, and diabetes prevalence that were observed in the present study did not reflect the characteristics of otomycosis. Rather, they were similar to the chronic otitis media findings. We speculate that the characteristics of the chronic condition were reflected in our findings because the premise of our study was the presence of chronic otitis media.
The Aspergillus and Candida species were the most common fungi that were found in otomycosis without chronic otitis media. Of the Candida species, Candida albicans has been reported by a large number of studies as the most common species2,9,11,18,19,21,29-35. However, in the present study, which focused on otomycosis co-occurring with chronic otitis media, Candida parapsilosis was the most common variety of Candida species. Patients with chronic otitis media experience recurrent discharge in the ear that induces symptoms like a feeling of strange fullness. Patients typically touch the outer ear canal with their finger or wipe the discharge away to get rid of the discomfort. It can be reasoned that by such repetitive behavior, the frequency with which the hand touches the outer ear canal increases, and the fungi on the surface of the finger are transmitted to the outer ear canal, which increases the likelihood of otomycosis. It has been reported that of the Candida species, C. parapsilosis is most commonly colonized on a healthy person's hand36-38. The present study found that C. parapsilosis was more frequently observed than C. albicans in patients with otomycosis co-occurring with chronic otitis media, unlike otomycosis without the chronic condition. We speculate that this is due to repetitive contacts between the finger and outer ear canal, among several causative factors.
Previous studies have reported inconsistencies with respect the laterality of otomycosis2,11,12,18,39. The study of the prevalence of chronic otitis media in South Korea did not find a difference in prevalence between right and left ears15. The statistical analysis that was conducted on the total sample of the present study showed that the number of patients in whom the right ear was affected was significantly higher than the number in whom the left ear was affected. When men and women were examined separately, the number of patients with a right ear lesion was higher in both men and women; and particularly in women, the difference was statistically significant. This finding is similar to the result presented by Prasad et al.12. Thus, the increased frequency of contact between the hand and outer ear canal in patients with chronic otitis media likely increases the occurrence of otomycosis. We speculate that the higher frequency right ear lesions is associated with the higher prevalence of right-handed, than left-handed, individuals.
In summary, the number of patients with otomycosis co-occurring with chronic otitis media increases with age. The prevalence was twice as high in women than in men, and the most common chief complaint at diagnosis was discharge in the right ear. Regarding causative fungi, the genus Aspergillus and genus Candida were similar in proportion. A. niger was identified as the most common variety of the Aspergillus species, and C. parapsilosis was identified as the most common among the Candida species.
In relation to this article, I declare that there is no conflict of interest.
References
1. Ho T, Vrabec JT, Yoo D, Coker NJ. Otomycosis: clinical features and treatment implications. Otolaryngol Head Neck Surg 2006;135:787-791
Crossref
Google Scholar
2. Kaur R, Mittal N, Kakkar M, Aggarwal AK, Mathur MD. Otomycosis: a clinicomycologic study. Ear Nose Throat J 2000;79:606-609
Crossref
Google Scholar
PubMed
3. Mugliston T, O'Donoghue G. Otomycosis--a continuing problem. J Laryngol Otol 1985;99:327-333
Crossref
Google Scholar
PubMed
4. Anwar K, Gohar MS. Otomycosis; clinical features, predisposing factors and treatment implications. Pak J Med Sci 2014;30:564-567
Crossref
5. Zaror L, Fischman O, Suzuki FA, Felipe RG. Otomycosis in São Paulo. Rev Inst Med Trop Sao Paulo 1991;33:169-173
Crossref
PubMed
6. Al-Husban H, Al-Serhan M, Al-Gudah A. Clinical presentation and treatment of otitis externa in Sierra Leone. JRMS 2004;11:65-67
Crossref
7. Jackman A, Ward R, April M, Bent J. Topical antibiotic induced otomycosis. Int J Pediatr Otorhinolaryngol 2005; 69:857-860
Crossref
Google Scholar
8. Swain SK, Behera IC, Sahu MC, Das A. Povidone iodine soaked gelfoam for the treatment of recalcitrant otomycosis - Our experiences at a tertiary care teaching hospital of eastern India. J Mycol Med 2018;28:122-127
Crossref
Google Scholar
9. Gharaghani M, Seifi Z, Zarei Mahmoudabadi A. Otomycosis in iran: a review. Mycopathologia 2015;179:415 -424
Crossref
PubMed
10. Vennewald I, Schönlebe J, Klemm E. Mycological and histological investigations in humans with middle ear infections. Mycoses 2003;46:12-18
Crossref
Google Scholar
PubMed
11. Paulose KO, Al Khalifa S, Shenoy P, Sharma RK. Mycotic infection of the ear (otomycosis): a prospective study. J Laryngol Otol 1989;103:30-35
Crossref
Google Scholar
PubMed
12. Prasad SC, Kotigadde S, Shekhar M, Thada ND, Prabhu P, D'Souza T, et al. Primary otomycosis in the Indian subcontinent: Predisposing factors, microbiology, and classification. Int J Med Microbiol 2014;2014:636493
Crossref
Google Scholar
13. Moharram A, Ahmed H, Nasr SA. Otomycosis in Assiut, Egypt. J Basic Appl Mycol Egypt 2013;4:1-11
Crossref
Google Scholar
14. Aneja KR, Sharma C, Joshi R. Fungal infection of the ear: a common problem in the north eastern part of Haryana. Int J Pediatr Otorhinolaryngol 2010;74:604-607
Crossref
Google Scholar
PubMed
15. Chung JH, Lee SH, Woo SY, Kim SW, Cho YS. Prevalence and associated factors of chronic suppurative otitis media: Data from the Korea National Health and Nutrition Examination Survey, 2009-2012. Laryngoscope 2016;126:2351 -2357
Crossref
Google Scholar
16. Agarwal P, Devi LS. Otomycosis in a rural community attending a tertiary care hospital: Assessment of risk factors and identification of fungal and bacterial agents. J Clin Diagn Res 2017;11:DC14-DC18
Crossref
Google Scholar
PubMed
17. Abdelazeem M, Gamea A, Mubarak H, Elzawawy N. Epidemiology, causative agents, and risk factors affecting human otomycosis infections. Turk J Med Sci 2015;45: 820-826
Crossref
Google Scholar
18. Jia X, Liang Q, Chi F, Cao W. Otomycosis in Shanghai: aetiology, clinical features and therapy. Mycoses 2012;55: 404-409
Crossref
Google Scholar
19. Nemati S, Hassanzadeh R, Khajeh Jahromi S, Delkhosh Nasrollah Abadi A. Otomycosis in the north of Iran: common pathogens and resistance to antifungal agents. Eur Arch Otorhinolaryngol 2014;271:953-957
Crossref
Google Scholar
20. Saunders JE, Raju RP, Boone JL, Hales NW, Berryhill WE. Antibiotic resistance and otomycosis in the draining ear: culture results by diagnosis. Am J Otolaryngol 2011;32: 470-476
Crossref
Google Scholar
PubMed
21. Ismail MT, Al-Kafri A, Ismail M. Otomycosis in Damascus, Syria: Etiology and clinical features. Curr Med Mycol 2017; 3:27-30
Crossref
Google Scholar
PubMed
22. Suh MK, Ha GY. A clinical and mycological study of otomycosis. Korean J Med Mycol 1999;4:15-20
Crossref
Google Scholar
23. Afshari MA, Kachoui R, Ajalloveyan M. Assessment of prevalence of otomycosis in ENT clinic in Baqiyatallah (a.s.) Hospital. J Mil Med 2005;7:121-124
Crossref
Google Scholar
24. García-Agudo L, Aznar-Marín P, Galán-Sánchez F, García-Martos P, Marín-Casanova P, Rodríguez-Iglesias M. Otomycosis due to filamentous fungi. Mycopathologia 2011; 172:307-310
Crossref
PubMed
25. Barati B, Okhovvat SAR, Goljanian A, Omrani MR. Otomycosis in Central Iran: A clinical and mycological study. Iran Red Crescent Med J 2011;13:873-876
Crossref
Google Scholar
PubMed
26. Mahmoudabadi AZ, Masoomi SA, Mohammadi H. Clinical and mycological studies of otomycosis. Pak J Med Sci 2010;26:187-190
Crossref
Google Scholar
27. Shokoohi T, Ahanjan M, Kasiri A. Bacteriological and mycological study of external otitis in patients referred to ENT clinic of Boo Ali Sina Hospital in Sari in summer 1999. J Mazandaran Univ Med Sci 2001;32:1-11
Crossref
Google Scholar
28. Kim DJ. The epidemiology of diabetes in Korea. Diabetes Metab J 2011;35:303-308
Crossref
Google Scholar
PubMed
29. Munguia R, Daniel SJ. Ototopical antifungals and otomycosis: a review. Int J Pediatr Otorhinolaryngol 2008;72: 453-459
Crossref
Google Scholar
30. Fayemiwo SA, Ogunleye VO, Adeosun AA, Bakare RA. Prevalence of otomycosis in Ibadan: a review of laboratory reports. Afr J Med Med Sci 2010;39 Suppl:219-222
Crossref
Google Scholar
PubMed
31. Pontes ZBVS, Silva ADF, Lima EO, Guerra MH, Oliveira NMC, Carvalho MFFP, et al. Otomycosis: a retrospective study. Braz J Otorhinolaryngol 2009;75:367-370
Crossref
PubMed
32. Pradhan B, Tuladhar NR, Amatya RM. Prevalence of otomycosis in outpatient department of otolaryngology in Tribhuvan University Teaching Hospital, Kathmandu, Nepal. Ann Otol Rhinol Laryngol 2003;112:384-387
Crossref
Google Scholar
33. Viswanatha B, Sumatha D, Vijayashree MS. Otomycosis in immunocompetent and immunocompromised patients: comparative study and literature review. Ear Nose Throat J 2012;91:114-121
Crossref
Google Scholar
34. Yassin A, Maher A, Moawad MK. Otomycosis: a survey in the eastern province of Saudi Arabia. J Laryngol Otol 1978;92:869-876
Crossref
Google Scholar
PubMed
35. Raper KB, Fennell DI. The genus Aspergillus. 1st ed. Baltimore: Williams & Wilkins Co., 1965
Crossref
36. Bonassoli LA, Bertoli M, Svidzinski TI. High frequency of Candida parapsilosis on the hands of healthy hosts. J Hosp Infect 2005;59:159-162
Crossref
Google Scholar
PubMed
37. Saiman L, Ludington E, Dawson JD, Patterson JE, Rangel¬Frausto S, Wiblin RT, et al. Risk factors for Candida species colonization of neonatal intensive care unit patients. Pediatr Infect Dis J 2001;20:1119-1124
Crossref
Google Scholar
38. Huang YC, Lin TY, Leu HS, Wu JL, Wu JH. Yeast carriage on hands of hospital personnel working in intensive care units. J Hosp Infect 1998;39:47-51
Crossref
Google Scholar
PubMed
39. Kurnatowski P, Filipiak A. Otomycosis: prevalence, clinical symptoms, therapeutic procedure. Mycoses 2001;44:472 -479
Crossref
Google Scholar
Congratulatory MessageClick here!
