pISSN : 3058-423X eISSN: 3058-4302
Open Access, Peer-reviewed
pISSN : 3058-423X eISSN: 3058-4302
Open Access, Peer-reviewed

Mingyu Kim,Kyung Hyun Min,Dong Soo Yu,Young Bok Lee
10.17966/JMI.2026.31.2.90 Epub 2026 June 30
Abstract
Keywords
Alopecia Antifungal agents Kerion Microsporum Tinea Capitis
A 21-month-old girl presented with multiple small, skin-colored, circular alopecic scalp patches accompanied by pruritus without scaling, erythema, or tenderness. Before presentation to our institution, she had received an unspecified topical corticosteroid from a local clinic for presumed alopecia areata. At presentation, the clinical findings were equivocal and not entirely consistent with active alopecia areata. The presence of vellus hairs suggested possible regrowth; there- fore, hydroxyzine and ciclopirox olamine shampoo were prescribed while further corticosteroid treatment was deferred. Two months later, the lesions had progressed to a boggy, suppurative plaque with broken hairs and exudate (Fig. 1A). The patient cried upon gentle palpation, indicating marked tenderness consistent with kerion celsi. Although she had a history of exposure to stray cats, no family members or household pets had obvious skin lesions. A Wood's lamp examination demonstrated faint yellow-green fluorescence (Fig. 1B), and potassium hydroxide (KOH) preparation revealed ectothrix invasion. Fungal culture subsequently identified Microsporum canis.
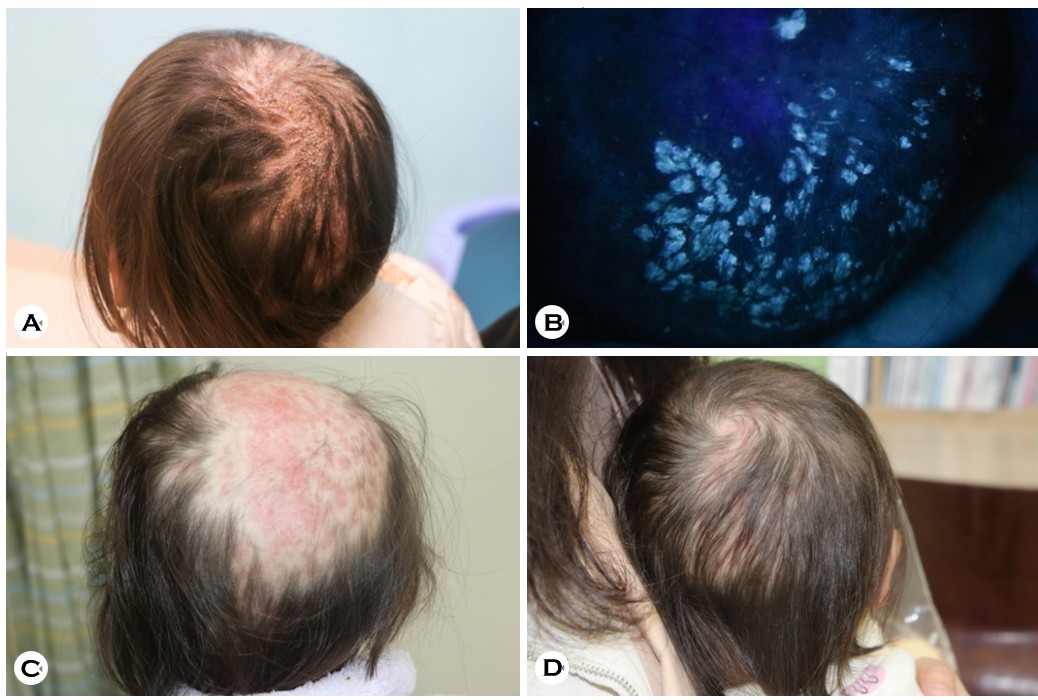
Although griseofulvin is the preferred treatment for pedi- atric Microsporum tinea capitis1, it is no longer available in Korea, and pediatric formulations of itraconazole have been discontinued. Given the severity of the inflammatory lesion and the restricted availability of pediatric antifungal therapies, oral fluconazole (100 mg/day; 10 mg/kg/day) was admin- istered for 3 months in combination with amorolfine 0.25% cream once daily, without adverse events2,3. Diffuse alopecia developed during the kerion phase (Fig. 1C). However, partial hair regrowth was observed 4 months after treatment initiation (Fig. 1D). No follow-up mycological testing was performed. This case highlights that early non-inflammatory tinea capitis may closely mimic alopecia areata in infants, potentially delaying diagnosis. Wood's lamp and KOH exam- inations should be considered early in the evaluation of infants presenting with focal alopecic patches.
References
1. Kakourou T, Uksal U, European Society for Pediatric Dermatology. Guidelines for the management of tinea capitis in children. Pediatr Dermatol 2010;27:226-228
Google Scholar
2. Valari M, Iordanidou A, Raftopoulou A, Pangalis A. Fluconazole in the treatment of pediatric tinea capitis caused by Microsporum canis. Drugs Exp Clin Res 2002; 28:161-164
Google Scholar
3. Foster KW, Friedlander SF, Panzer H, Ghannoum MA, Elewski BE. A randomized controlled trial assessing the efficacy of fluconazole in the treatment of pediatric tinea capitis. J Am Acad Dermatol 2005;53:798-809
Google Scholar
Congratulatory MessageClick here!
