pISSN : 3058-423X eISSN: 3058-4302
Open Access, Peer-reviewed
pISSN : 3058-423X eISSN: 3058-4302
Open Access, Peer-reviewed

Yashpal Manchanda,Abeer AlBazali,Khaled Obaid,Mohammad Asadzadeh,Hawraa Taqi
10.17966/JMI.2026.31.2.80 Epub 2026 June 30
Abstract
Mycetoma is a type of chronic granulomatous infection that affects the skin and subcutaneous tissue, typically resulting from the traumatic inoculation of the causative organism. Typically, this disease is limited to the countries located in the subtropical zone. It is conventionally diagnosed based on certain typical direct microscopic features of grains and culture properties. However, the sensitivity and specificity of these tests are highly variable, apart from being time-consuming, invasive, and subjective. The rapid establishment of the identity of the causative organism, along with its drug susceptibility, plays an important role in the management of mycetoma to avoid complications and side effects associated with the long-term use of currently available drugs. Notably, cases of mycetoma have not been reported in Kuwait. This study investigated the first confirmed case of eumycetoma, and a brief comparative analysis of various molecular diagnostic tests currently used for diagnostic confirmation was performed.
Keywords
Black grains Granulomatous dermatitis Madurella mycetomatis Mycetoma
Mycetoma is a chronic granulomatous disease affecting the skin and subcutaneous tissues, typically resulting from the traumatic inoculation of the causative organism1. Cases of this disease are geographically restricted to the "mycetoma belt" formed by countries from tropical and subtropical regions lying within 30°N and 15°S latitude of the equator line2. No cases of mycetoma have been reported in Kuwait. The pre- sent study reported the first case of Madurella mycetomatis infection in Kuwait, which was confirmed by molecular and microbiological diagnostic tests. Various molecular diagnostic techniques currently used for diagnostic confirmation were also compared.
A 32-year-old Sudanese male farmer presented with a 4-month history of swelling on the right sole, along with pus discharge and the presence of sporadic black-colored granules. No systemic complaints, such as weight loss, night sweats, chronic cough, or a low-grade persistent fever, were reported. The patient denied any definitive history of a penetrating injury at the site preceding the lesion. He also did not report any known comorbid conditions such as diabetes. Dermato- logical examination revealed a brownish lobulated, firm, nontender mass on the sole of the right foot in the medial plantar arch area, including areas of the discharging sinuses (Fig. 1). Underneath the skin around the sinuses, black-colored grains were also observed. Regional lymph nodes were not palpable.

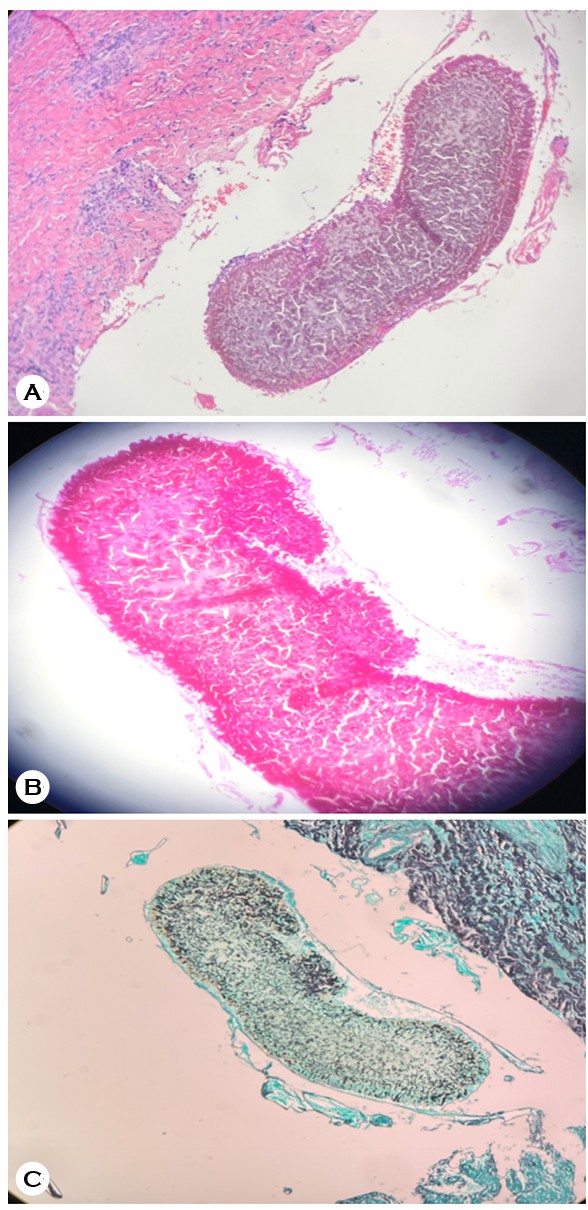
A 10% potassium hydroxide preparation was made from the granules collected after 24 hours of wet saline dressing. It showed multiple branched filamentous structures suggestive of a fungus. An incisional biopsy was performed under local anesthesia via an elliptical incision around a discharging sinus (Fig. 2). The excised tissue was sent for histopathology, acid-fast bacilli culture, fungal culture, and molecular diag- nostic tests. Histopathology, supplemented by periodic acid-Schiff (PAS) and Gomori's methenamine silver (GMS) staining, showed a dense infiltration of the neutrophils, eosinophils, lymphocytes, and histiocytes in the dermis and subcutaneous tissue as well as the presence of a grain in the deeper dermis, which stained positively after PAS and GMS staining (Fig. 3A, B, C). The samples were sent to the mycology laboratory in sterile saline for the culture isolation of the causative agent. The fungal culture yielded a filamentous mold with a yellow diffusible pigment indicative of M. mycetomatis. It was further confirmed via polymerase chain reaction (PCR) sequencing of the beta-tubulin gene and D1/D2 domains of rDNA. Other routine laboratory investigations, including complete blood count, liver function test, renal function test, chest X-ray, Mantoux test, and T-SPOT.TB, were all within normal limits. Moreover, a foot X-ray showed no bony involvement.

The patient was initially administered 200 mg of itraconazole (tablet) twice daily after meals. After 4 weeks of initiating the treatment, he was referred to surgery for complete surgical excision and advised to follow up with us after surgery for the continuation of antifungal therapy.
Cases of eumycetoma have never been reported in Kuwait, wherein its climate is generally hot and dry throughout the year, with minimal rainy days. Majority of the residents are immigrants from various parts of the world, who are by and large in their prime age (age group of 20-50 years: working class) and have been screened for any medical condition prior to their arrival as immigrants. In the present case, the duration of onset was very short, and no definitive history of penetrating injuries to the site was noted. However, it is highly possible that the organism was introduced into the skin in the patient's country of origin (Sudan), considering the prolonged incubation period associated with this condition. Nonetheless, this is the first confirmed case in this region.
Conventionally, the identification of the causative organism was based on the direct microscopic examination of grains and culture properties. However, these tests have widely varying sensitivity and specificity rates3. Besides, they are invasive, require a prolonged time, and are subject to wide inter- operator variations. More often than not, these happen to be inconclusive if done in isolation4. Moreover, they have to be performed together to reach a specific diagnosis. Direct grain microscopy may exclude the possibility of actinomycetoma. Fine needle aspiration cytology indicated two types of M. mycetomatis, namely, granular and vesicular types. However, it cannot differentiate between various causative eumycotic organisms, for example, M. mycetomatis from Trematos- phaeria grisea, due to lack of information about the different phenotypes and identification patterns of eumycetoma causing fungi.
Even the prolonged use of currently available systemic antifungal agents for the treatment of eumycetoma does not guarantee a clinical cure in at least half of the cases5. Furthermore, these drugs, when used in higher doses and/or for longer durations, are often toxic and associated with severe adverse effects. Thus, establishing the exact identity of the causative microorganism along with its drug susceptibility is important to avoid complications and side effects.
The identification of the genetic variability of causative organisms is considered to be a more stable and specific mode compared with using methods based on phenotypic criteria. Recently, various DNA-based molecular diagnostic techniques have been developed to complement and/or replace conven- tional methods (Table 1). A new system, the API 20C AUX kit, was recently introduced and was able to identify Madurella fahalii, Madurella pseudomycetomatis, and Madurella tro- picana6. Whole genome sequencing is another useful tool that can provide many genetic markers, which in turn can be probed for the development of molecular diagnostic methods and identification of potential drug markers7.
|
Technique |
Main use in |
Advantages |
Limitations |
Refs |
|
ITS and D1/D2
rDNA sequencing Fungal ribosomal DNA barcoding |
Species-level identification |
Broadly applicable Useful for rare or novel fungi Allows comparison with |
Requires good-quality DNA and May require culture or
adequate Higher cost and longer
turnaround |
6 |
|
Species-specific
PCR-RFLP Amplification followed |
Identification of Madurella mycetomatis and related |
Faster than conventional
phenotypic identification Relatively specific for |
Limited to organisms covered Requires molecular laboratory Not ideal for unexpected or |
9 |
|
AFLP genotyping Genome-wide restriction |
Strain typing, epidemiology, |
High discriminatory power Useful for geographic and
epidemiologic comparisons |
Technically demanding Requires expertise and Not suitable for routine |
8 |
|
Rolling circle
amplification Probe-based isothermal amplification |
Rapid identification of selected
black-grain eumycetoma |
Simple amplification format Species-specific Potentially faster than |
Requires species-specific
probes Limited panel coverage Not field-friendly in many |
10 |
|
Loop-mediated
isothermal Isothermal amplification |
Rapid detection of Madurella mycetomatis, especially |
Rapid Does not require a conventional
PCR thermocycler Conceptually suitable for |
Narrow assay range False positives may occur
with contamination Requires validation, DNA |
11 |
|
MALDI-TOF MS Protein mass |
Rapid identification after |
Fast once culture is
available Low running cost after
establishment Helpful for non-sporulating or
slowly sporulating isolates if database coverage is adequate |
Requires culture and an High initial equipment cost Performance depends heavily |
12 |
|
Whole-genome Whole-genome analysis |
Reference genome |
Highest-resolution Useful for novel species and
research questions beyond |
Expensive Requires bioinformatics expertise Slow for routine diagnosis and Often requires a cultured isolate |
7 |
For M. mycetomatis, various methods have been used, including restriction endonuclease analyses (REA), random amplified polymorphic DNA (RAPD), and amplified fragment length polymorphism (AFLP)8. One of the molecular diag- nostic techniques being extensively used is PCR coupled with REA of PCR products, PCR-based randomly amplified polymorphic DNA fingerprinting, and Curie-point pyrolysis mass spectrometry. Of these, RAPD has shown highly variable results. Conversely, REA and AFLP were able to differentiate the isolates of M. mycetomatis obtained from different coun- tries and sometimes even from within the same country9.
Ahmed et al. (2014), while studying a sample of 62 isol- ates, applied the rolling circle amplification (RCA) technique, which is a relatively simple and cheaper technique with very high specificity for the identification of Falciformispora senegalensis, F. tompkinsii, M. fahalii, M. mycetomatis, M. pseudomycetomatis, M. tropicana, Medicopsis romeroi, and T. grisea. This technique was shown to produce results with 100% specificity and have no single case of cross-reactivity or false results10. RCA applies species-specific padlock probes and an isothermal DNA amplification technique. They concluded that the RCA technique can potentially be implemented in endemic areas and can even be expanded to detect fungal DNA from environmental samples. Unfortunately, even RCA is based on the amplification of the ITS gene, and the local nonavailability of thermocyclers required to perform PCR can be an issue in some regions.
The loop-mediated isothermal amplification method has been developed to forego the need for using PCR, which is one of the main limiting factors in resource-poor settings. It basically relies on the four primers used to identify six specific regions in the target DNA, followed by amplification via autocycling and strand displacement with a specialized DNA polymerase11.
Another method developed is matrix-assisted laser desor- ption/ionization-time-of-flight mass spectrometry (MALDI-TOF MS). It has been proven to be a robust, cheaper, simpler, and relatively faster mode for identifying various pathogenic microorganisms from pure culture. It requires the cocrystalli- zation of the sample with a matrix that absorbs laser light and converts it into the gas phase. Thus, the ions formed reach the detector at a speed inversely proportional to their mass/charge (m/z) ratio, creating a signal according to the time taken to hit the detector by each of the ion particles. However, it heavily relies on the availability of the appropriate reference MALDI-TOF spectra in the commercial databases supplied with various MALDI-TOF platforms. In addition, it needs an initial heavy financial cost for procuring mass spec- trometers12.
The main drawback with molecular-based diagnostic tools is that they can only be performed at large diagnostic centers and cannot be applied in field settings. This is because most mycetoma patients live in far-flung areas, with no accessible large health centers. They need to travel long distance, in- volving significant travel expenses. Thus, the scientific com- munity should make concerted efforts to develop cheap, easy, and quicker field-based diagnostic tools to identify the causative agents to the species level, allowing the treating physician to prescribe proper treatment accordingly.
Since this disease is not endemic to Kuwait, physicians must be aware of its presentation and consider it in their differential diagnosis. Thus, a specific diagnosis can be made early in the disease process, and effective treatment can be initiated to avoid the usual complications of a long-term untreated disease.
References
1. Baby P, Mohan V, Eapen M, Kurian A, Ramachandran A, Babu BC, et al. Madurella mycetoma: A neglected tropical disease. Clin Microbiol Infect 2022;28:375-376
Google Scholar
2. Nenoff P, van de Sande WW, Fahal AH, Reinel D, Schöfer H. Eumycetoma and actinomycetoma – an update on causative agents, epidemiology, pathogenesis, diagnostics and therapy. J Eur Acad Dermatol Venereol 2015;29: 1873-1883
Google Scholar
3. Relhan V, Mahajan K, Agarwal P, Garg VK. Mycetoma: An update. Indian J Dermatol 2017;62:332-340
Google Scholar
4. van de Sande WW, Fahal AH, Goodfellow M, Mahgoub el S, Welsh O, Zijlstra EE. Merits and pitfalls of currently used diagnostic tools in mycetoma. PLoS Negl Trop Dis 2014;8:e2918
Google Scholar
5. Elkheir LY, Haroun R, Mohamed MA, Fahal AH. Madurella mycetomatis causing eumycetoma medical treatment: The challenges and prospects. PLoS Negl Trop Dis 2020; 14:e0008307
Google Scholar
6. Yan J, Deng J, Zhou CJ, Zhong BY, Hao F. Phenotypic and molecular characterization of Madurella pseudomyceto- matis sp. nov., a novel opportunistic fungus possibly causing black-grain mycetoma. J Clin Microbiol 2010;48: 251-257
Google Scholar
7. Smit S, Derks MF, Bervoets S, Fahal A, van Leeuwen W, van Belkum A, et al. Genome sequence of Madurella mycetomatis mm55, isolated from a human mycetoma case in Sudan. Genome Announc 2016;4:e00418-16
Google Scholar
8. van de Sande WW, Gorkink R, Simons G, Ott A, Ahmed AO, Verbrugh H, et al. Genotyping of Madurella myceto- matis by selective amplification of restriction fragments (amplified fragment length polymorphism) and subtype correlation with geographical origin and lesion size. J Clin Microbiol 2005;43:4349-4356
Google Scholar
9. Ahmed AO, Mukhtar MM, Kools-Sijmons M, Fahal AH, de Hoog S, van den Ende BG, et al. Development of a species-specific PCR restriction fragment length polymor- phism analysis procedure for identification of Madurella mycetomatis. J Clin Microbiol 1999;37:3175-3178
Google Scholar
10. Ahmed SA, van den Ende BH, Fahal AH, van de Sande WW, de Hoog GS. Rapid identification of black grain eumycetoma causative agents using rolling circle amplifi- cation. PLoS Negl Trop Dis 2014;8:e3368
Google Scholar
11. Ahmed SA, van de Sande WW, Desnos-Ollivier M, Fahal AH, Mahmoud NA, de Hoog GS. Application of isothermal amplification techniques for identification of Madurella mycetomatis, the prevalent agent of human mycetoma. J Clin Microbiol 2015;53:3280-3285
Google Scholar
12. Florio W, Tavanti A, Barnini S, Ghelardi E, Lupetti A. Recent advances and ongoing challenges in the diagnosis of microbial infections by MALDI-TOF mass spectrometry. Front Microbiol 2018;9:1097
Google Scholar
Congratulatory MessageClick here!
