pISSN : 3058-423X eISSN: 3058-4302
Open Access, Peer-reviewed
pISSN : 3058-423X eISSN: 3058-4302
Open Access, Peer-reviewed

Hye-Jin Ahn
10.17966/JMI.2026.31.2.61 Epub 2026 June 30
Abstract
Achieving a cure for onychomycosis remains challenging despite systemic and/or topical antifungal therapy. Topical antifungals have limitations due to hyperkeratotic nail plate, and systemic antifungals have the potential to cause systemic side effects and drug interactions. Nondermatophyte molds have a relatively low response to antifungal agents, and increased antifungal resistance dermatophyte strains have been reported recently. Furthermore, fungal biofilms are associated with enhanced resistance to antimicrobial agents. Therefore, better results can be achieved by combining nonpharmacological treatment modalities. Mechanical debridement/partial avulsion can reduce the infected keratin and contribute to shortening the duration of antifungal treatment. Device-based treatments are minimally invasive and have the potential to restore clear nail growth, although sufficient evidence is lacking. This review aims to discuss nonpharmacological treatments for onychomycosis and explore ways to improve the cure rate of onychomycosis.
Keywords
Carbon dioxide lasers Debridement Neodymium-YAG laser Nonthermal atmospheric pressure plasma Onychomycosis
Onychomycosis presents with nail discoloration (yellow or white, and brown in cases of heavy fungal burden), onycho- lysis, nail brittleness, nail plate thickening, and subungual hyperkeratotic debris. The condition can significantly impair the quality of life. It is a chronic fungal infection, and treatment typically requires prolonged therapy; however, recurrence remains a frequent challenge. Although oral systemic anti- fungal agents are the standard therapy for onychomycosis, cure rates are not high. Terbinafine achieves a mycological cure rate of approximately 70% and a complete cure rate of 38% in toenail infections, whereas itraconazole yields a mycological cure rate of 54% and a complete cure rate of 14%1. Furthermore, relapse or reinfection rates of approxi- mately 20-25% have been reported even after successful initial treatment1,2. Systemic conditions, including diabetes, impaired circulation, peripheral neuropathies, and immuno- suppression, as well as the type of causative fungus, are asso- ciated with poor treatment outcomes. The recent emergence of terbinafine-resistant Trichophyton indotineae has become a significant global concern. Although the optimal treatment for T. indotinea has not been established, increasing the dose and/or duration of antifungal therapy may help overcome resistance3. However, given the chronic, relapsing nature of infections caused by this organism, treatment with antifungal agents alone may be insufficient. Nonpharmacological treat- ments may provide an adjuvant effect by reducing fungal burden. In addition, biofilm formation may contribute to re- current infection and treatment resistance. Biofilms provide a protective barrier for organisms, conferring resistance to external insults and preserving a persistent infectious reservoir that promotes antifungal resistance4. Therefore, additional treatment options are needed to address the limitations of current therapies. In this review, we discuss nonmedical treatments for onychomycosis, including physical debridement and device-based treatments, with a focus on strategies to improve treatment efficacy.
Removing all infected keratin from a nail affected by onychomycosis can reduce the infectious load, similar to how drainage reduces the burden of an abscess. This approach has been shown to enhance mycological cure rates and may shorten the course of systemic treatment5.
2.1. Mechanical/Physical debridement
2.1.1. Recommended clinical subtypes
Physical debridement was suggested for some specific forms of onychomycosis6. In particular, surgical debridement may be beneficial in clinical subtypes in which systemic or topical antifungal therapies show limited efficacy. For instance, in cases involving a markedly thickened nail plate or dermato- phytoma, antifungal agents cannot adequately penetrate the dense keratin mass. In onycholysis, separation of the nail plate from the nail bed prevents systemic antifungals from reaching the nail plate via the nail bed, while topical agents cannot effectively penetrate from the nail plate to the nail bed. Similarly, antifungal treatment of lateral onychomycosis is often less effective because detachment of the nail plate from the nail bed impairs drug delivery6 (Table 1). Treatment of nondermatophyte molds (NDMs) is not well standardized, and these fungi respond poorly to systemic antifungal agents compared with dermatophytes7-10. In such cases, physical debridement combined with antifungal therapy is recom- mended as the first-line approach9,10.
|
Clinical
types |
Limitations
of antifungals |
|
|
Marked
thickened nail plate (>3 mm) |
Topical
antifungals |
Difficult
to penetrate the dense keratin mass. |
|
Dermatophytoma |
||
|
Onycholysis |
Systemic/topical |
- Systemic antifungals are difficult to reach the
nail - Topical agents are difficult to reach the nail
bed |
|
Lateral
onychomycosis |
||
|
Nondermatophyte
mold infection |
Systemic/topical |
Limited
efficacy against antifungal agents. |
|
Biofilm |
||
2.1.2. Method for mechanical/physical/ chemical debridement
Mechanical/physical debridement does not require local anesthesia, and the procedure is noninvasive and safe for all patients, including those with peripheral vascular disease and diabetes. Curettage to remove subungual debris (hyponychial keratin) is particularly important, as this material is rich in fungal filaments6.
Chemical avulsion using 40% urea occlusion has long been used6,11. This selective method acts only on the infected keratin. Urea dissolves the bonds between the nail bed and the nail plate and also softens the nail plate6. After approxi- mately one week of occlusion, the infected part of the nail can be removed painlessly12.
Laser devices have emerged as therapeutic alternatives for onychomycosis. Unlike antifungal drugs, which require demon- strated efficacy in strict randomized controlled trials for approval by the US Food and Drug Administration (FDA), the 1,064-nm neodymium-doped/yttrium aluminum garnet (Nd:YAG) laser was approved by the FDA in 2010 for the "temporary increase in clear nail," an aesthetic endpoint that does not necessarily reflect fungal eradication13,14. Accordingly, evidence supporting the efficacy of laser devices remains limited compared with antifungal agents. Among clinical studies of laser device-based treatments, the Nd:YAG laser is the most commonly studied and has shown mixed outcomes, followed by the carbon dioxide (CO2) lasers14. This review focuses on Nd:YAG lasers, CO2 lasers, and the emerging modality of nonthermal atmospheric pressure plasma (NTAP).
3.1. Neodymium doped/yttrium aluminum garnet (Nd:YAG) laser
3.1.1. Proposed mechanism of action against fungi
The antifungal effect of lasers is thought to rely primarily on photothermal effects, in which fungal cells absorb laser energy and convert it into heat, leading to cellular damage6,14,15. This heat causes protein denaturation and inactivation of fungal cells16. Optimization of laser parameters must account for the thermal properties of the surrounding tissues to avoid damage to healthy human cells and ensure selective targeting of fungal cells14,16. Fungal cells have a lower heat capacity than surrounding human dermal cells, allowing them to heat up more rapidly and retain heat longer6,14. Thermal relaxation time (TRT), defined as the time required for cells to dissipate heat, determines pulse duration and intervals between pulses14,15. Both fungal hyphae and conidia have a TRT of less than 1 μs6. Based on selective photothermolysis, pulse duration should be shorter than the TRT of the target to allow heat accumulation6,15. Q-switched Nd:YAG lasers use nanosecond pulse durations but produce minimal ther- mal effect. Long-pulsed 1,064-nm lasers require continuous cooling to avoid severe pain and injury. Short-pulsed Nd:YAG lasers are considered advantageous. Fungal chromophores are an additional factor that can be used to induce a fungicidal effect by lasers, which can be explained by photomechanical/ acoustic phenomena6. An in vitro study showed that treat- ment with 1,064-nm Q-switched Nd:YAG laser and 532-nm Q-switched Nd:YAG laser resulted in a much lower growth rate of Trichophyton rubrum Rcolonies17. The 1,064 nm wave- length is absorbed by melanin in fungal cell walls, whereas the 532-nm wavelength is absorbed by xanthomegnin17. However, wavelengths that effectively penetrate the nail range from 750 to 1,300 nm18, making the short-pulsed 1,064-nm Nd:YAG laser the most widely used modality.
3.1.2. In vitro studies of the Nd:YAG laser
Vural et al.17 demonstrated significant inhibition of T. rubrum colony growth following treatment with both 1,064-nm and 532-nm Nd:YAG lasers, suggesting the potential utility of laser therapy for onychomycosis. Temperature of 55℃ are the lowest capable of killing dermatophytes via heat19. Carney et al.20 reported that the temperature of 50℃ inhibited T. rubrum colonies after 5 min and was fungicidal after 15 min. Conversely, direct Nd:YAG irradiation failed to demonstrate any effect on T. rubrum's growth while the temperature on agar plates peaked at 40℃. The authors concluded that a fungicidal effect was only achieved by heat; however, the necessary parameters (high degree of temperature and dur- ation of heating) could not be adapted for clinical practice because temperatures over 45℃, resulting in pain and necrosis in humans18,20.
3.1.3. Reported RCTs of short-pulsed 1,064-nm Nd:YAG laser monotherapy
In South Korea, the approved indication for laser-based treatment of onychomycosis is limited to patients who cannot tolerate oral antifungal therapy or have contraindications to it. Numerous clinical studies of laser-based treatments have reported variable and inconsistent efficacy in onychomycosis. However, RCTs evaluating short-pulsed 1,064-nm Nd:YAG laser monotherapy have failed to show significant treatment effects21-23 (Table 2). In an RCT by Hollmig et al.21, patients in the laser group underwent two sessions of 1,064-nm Nd:YAG laser treatment at 2-week intervals, using a fluence of 5 J/cm2, pulse width of 0.3 ms, spot size of 6 mm, and a repetition rate of 6 Hz to achieve a target temperature of 40-42℃. The results showed no significant difference in the percentage of patients with negative nail cultures between the laser and control groups (p = .49). Although patients treated with laser showed greater proximal nail plate clearance than controls (0.44 vs 0.15 mm, p = .18), this difference was not statistically significant. Moreover, the modest improve ment of proximal nail plate clearance seen in the laser group was not sustained. In another RCT, 20 patients (82 mycotic toenails) were randomized to a short-pulsed 1,064-nm Nd: YAG laser group or a control group22. The laser group received four treatments at 4-6-week intervals, with a follow-up period of 12 months. Neither group achieved mycological remission, and Onychomycosis Severity Index scores did not significantly differ between groups. The authors conclude that the short-pulsed 1,064-nm Nd:YAG laser shows no long-term efficacy as a monotherapy. Similarly, Sabbah et al.23 reported that three treatments with a 1,064-nm Nd:YAG laser administered at 3-month intervals were ineffective for the treatment of onychomycosis. In their study, 51 patients were randomized to receive three treatments (at weeks 0, 12, and 24) with either a short-pulsed 1,064-nm Nd:YAG laser or a placebo sham laser. No patients (0%) in the laser group achieved the primary outcome.
|
|
Possible |
References |
Level of |
Baseline
characters, Protocol |
Reported
efficacy Mycological
cure (negative mycological result) |
Clinical
response |
Combination
strategies |
|
Nd:YAG |
- Photothermal |
Hollmig21 |
RCT |
- Laser - Control - The laser group underwent two |
33%
in the laser group |
More proximal nail |
|
|
Karsai22 |
RCT |
- Laser - Control - The laser group underwent four |
Mycological
remission |
A
comparison to |
Combination |
||
|
Sabbah23 |
RCT |
- Laser - Control - The laser group underwent three
treatments at intervals of 12 weeks. |
33%
in the laser group |
No
patient (0%) in the laser group reached a |
|
||
|
CO2 |
- Enhance the - Thermal |
Lim29 |
Single-arm |
- 24 patients with 119 nails - Three treatments at 4-week intervals |
- 50%
complete cure. |
92%
showed a |
Combination
with topical antifungal cream. |
|
Bhatta30 |
Single-arm |
- 75 patients with 356 nails. - Three treatments at 4-week intervals |
92%
after 3 months and |
|
Combination
with topical antifungal cream. |
||
|
Zaki34 |
RCT |
- Laser + topical (Group A) - Laser alone (Group B) - Topical
alone (Group C) |
Mycologically
negative |
Complete
clinical improvement 55% in Group A, 30% in |
Combination |
||
|
Ranjan36 |
A
pilot study |
- Urea occlusion + laser -
Laser only |
- |
In
the laser following overnight urea cream occlusion group, |
Combination |
||
|
NTAP |
Antimicrobial effect through reactive
oxygen and nitrogen species |
Lux49 |
Nonrandomized,
three-arm comparative |
- NTAP+ topical antifungals - Nail
removal+ NTAP |
The
mycological cure |
- The
overall therapeutic |
NTAP
irradiation |
|
*OSI:
onychomycosis severity index; NTAP: nonthermal atmospheric
pressure plasma |
|||||||
Numerous fungal spores have been identified within the infected nail plate, and a fungal biofilm surrounding a spore has also been observed24, contributing to the chronic infection course of onychomycosis. T. rubrum often produces arthro- conidia in vivo, and the arthroconidia are thought to be involved in pathogenesis and, in shed skin scales, act as a source of infection25. In vitro study revealed that arthroconidia formation of T. rubrum occurred optimally at 37℃ and pH 7.5 and was maximal at 10 days25. In the resting state, the toe skin temperature is approximately 27.8 ± 3.0℃26. When Nd:YAG laser treatment is delivered at suboptimal energy levels, the resulting temperature increase may fall within a range that favors arthrospore formation, potentially promoting rather than inhibiting spore production. A previous studies on the heat resistance of dermatophyte conidiospores has demonstrated that these spores exhibit high resistance to heat exposure at 80℃27. Therefore, even when nail plate temperatures approach 50℃ during the 1,064-nm Nd:YAG laser, fungal hyphae can be damaged or destroyed, whereas numerous viable spores may persist. RCTs have shown no significant therapeutic effect when treatment intervals exceed 1 month22,23. In contrast, laser treatments administered at 2-week intervals have demonstrated some clinical improvement; however, these effects were not sustained over time21. In this context, when treatment intervals are prolonged, residual fungal elements are more likely to contribute to fungal regrowth. Consequently, because the therapeutic mechanism of the Nd:YAG laser relies primarily on the photothermal effect, its efficacy as monotherapy is limited unless higher laser intensities and shorter treatment intervals are employed.
3.2. Carbon-dioxide lasers (CO2 lasers)
3.2.1. Reported clinical studies of CO2 laser
The CO2 laser represents the oldest laser-based approach for the treatment of onychomycosis28. It may be used as primary therapy or in combination with topical antifungals agents to enhance drug penetration through the nail plate into the nail bed29. The first study of ablative fractional CO2 laser combined with a topical antifungal reported a favorable clinical response after three laser sessions administered at 4-week intervals, along with once-daily amorolfine cream for 3 months. In that study, 50% of patients achieved a complete response, defined as negative microscopic findings, with no recurrence observed during the 3-month follow-up29. Similarly, studies evaluating fractional CO2 laser therapy in combination with topical antifungal creams have demonstrated efficacy in the treatment of onychomycosis30,31. Specifically, 33.33% of patients achieved a complete clinical response at 6 months of follow-up, and 80% were culture negative30. In another study, 69.6% of nails showed either complete or greater than 60% normalization in appearance, and 57.4% demonstrated negative fungal microscopic results31. In contrast to previous studies, a retrospective review literature reported a complete response (CR) rate—defined as 100% nail clearance of all treated toenails per patient—of only 15.6% after three or more fractional CO2 laser treatments administered at inter- vals of at least 4 weeks, in combination with topical anti- fungal agents32. This CR rate is comparable to or lower than that achieved with topical efinaconazole 10% (17.8% and 15.2%)33. Although results have been inconsistent, the CO2 laser emits light at a wavelength of 10,600 nm, at which water serves as the primary chromophore. Absorption of this energy leads to heat generation, which is thought to produce antifungal effects. In a study comparing fractional CO2 laser followed by topical antifungal treatment (ticonazole 28% solution) (Group A), fractional CO2 laser alone (Group B), and topical antifungal treatment alone (Group C), a significant difference in clinical response was observed among the three groups (p < .005)34. Complete clinical response was observed in 55% of patients in Group A, compared with 30% in Group B and 25% in Group C. Notable, CO2 laser monotherapy produced better clinical outcomes than topical antifungal therapy alone. Fractional CO2 laser treatment in a single session following 12% urea occlusion of the affected nail for 24 h showed excellent results35,36. Urea is a hygroscopic agent, and urea occlusion softens the nail plate and helps provide water chromophore at depth, thus enabling the accelerated fungicidal effect of a fractional CO2 laser36. Therefore, precise and selective delivery of high-energy laser irradiation to the infected nail plate is important in determining the therapeutic effect of CO2 laser treatment.
3.3. Nonthermal atmospheric pressure plasma
3.3.1. In vitro studies of NTAP
T. rubrum is the most common cause of nail infections, accounting for approximately 80% of all dermatophyte in- fections in humans37. Candida spp. and NDMs, i.e., Scopula- riopsis brevicaulis, Aspergillus spp., and Fusarium spp., can also be causative fungi. In addition, in untreated cases of onychomycosis, the nail plate may be completely destroyed, and infections with mixed bacteria and fungi may develop1,38. Nonthermal atmospheric pressure plasma (NTAP) is considered an attractive alternative option due to its surface disinfection and antimicrobial effect39. The antimicrobial effects of NTAP have been reported to include methicillin-resistant Staphylo- coccus aureus (MRSA)40, C. albicans41,42, dermatophytes39,43-45, and A. fumigatus46. Although the mechanism of NTAP is not fully understood, reactive oxygen and nitrogen species (ROS; RNS) generated by NTAP, rather than heat, are thought to play a key role in its antimicrobial effect47.
3.3.2. Reported clinical studies of NTAP
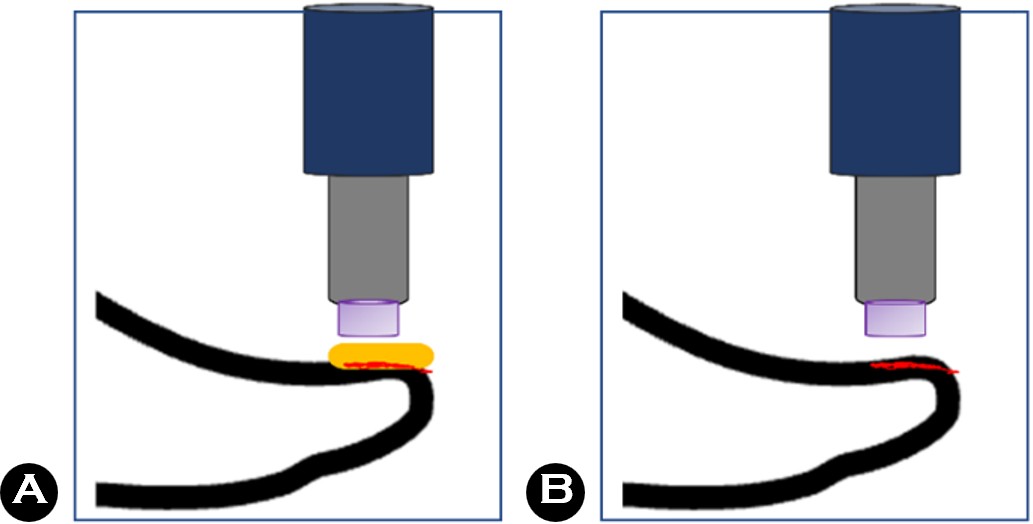
Despite numerous in vitro evidence of NTAP supporting antimicrobial effects, relatively few clinical studies48,49 have investigated their efficacy in the treatment of onychomycosis. The first pilot study reported overall clinical cure of 53.8%, and mycological cure of 15.4% after application to the dorsal layer of the nail plate48. However, the hyponychium is the primary site of dermatophyte entry into the nail, where abundant fungal elements are present50,51. In addition, the subungual space can serve as a reservoir for superinfecting bacteria and molds52. In this regard, applying NTAP after removing the nail plate can be a good strategy (Fig. 1). In addition, since the application of NTAP to damaged skin is generally tolerable53,54, it will be a suitable method for appli- cation to the nail bed without a nail plate. In another clinical study49, the combination of nail plate abrasion and NTAP resulted in better outcomes compared with NTAP combined with topical antifungal agents, with mycological cure achieved in 85.7% of patients in the case of nail plate abrasion with NTAP. In addition, all patients reported that the treatments were tolerable. Thus, with further validation in well-designed clinical trials, NTAP therapy has the potential to become an effective treatment modality for onychomycosis.
Physical debridement and device-based treatments may serve as useful adjunctive options in the management of onychomycosis. However, achieving effective treatment inten- sity while avoiding injury to adjacent normal tissues remains challenging. Improved outcomes will depend on a thorough understanding of disease characteristics, as well as the benefits and limitations of available device-based treatments.
References
1. 1. Gupta AK, Stec N, Summerbell RC, Shear NH, Piguet V, Tosti A, et al. Onychomycosis: A review. J Eur Acad Dermatol Venereol 2020;34:1972-1990
Google Scholar
2. 2. Piraccini BM, Sisti A, Tosti A. Long-term follow-up of toenail onychomycosis caused by dermatophytes after successful treatment with systemic antifungal agents. J Am Acad Dermatol 2010;62:411-414
Google Scholar
3. 3. Gupta AK, Susmita, Nguyen HC, Liddy A, Talukder M, Wang T, et al. Trichophyton indotineae: Epidemiology, antifungal resistance and antifungal stewardship strat- egies. J Eur Acad Dermatol Venereol 2026;40:29-45
Google Scholar
4. 4. Gupta AK, Daigle D, Carviel JL. The role of biofilms in onychomycosis. J Am Acad Dermatol 2016;74:1241-1246
Google Scholar
5. 5. Baran R, Hay RJ. Partial surgical avulsion of the nail in onychomycosis. Clin Exp Dermatol 1985;10:413-418
Google Scholar
6. 6. Rigopoulos D, Elewski B, Richert B. Onychomycosis: Diagnosis and effective management. John Wiley & Sons; 2018
Google Scholar
7. 7. Gupta AK, Summerbell RC, Venkataraman M, Quinlan EM. Nondermatophyte mould onychomycosis. J Eur Acad Dermatol Venereol 2021;35:1628-1641
Google Scholar
8. 8. Hwang SM, Suh MK, Ha GY. Onychomycosis due to nondermatophytic molds. Ann Dermatol 2012;24:175-180
Google Scholar
9. 9. Gupta AK, Drummond-Main C, Cooper EA, Brintnell W, Piraccini BM, Tosti A. Systematic review of nondermato- phyte mold onychomycosis: Diagnosis, clinical types, epidemiology, and treatment. J Am Acad Dermatol 2012; 66:494-502
Google Scholar
10. 10. Tosti A, Piraccini BM, Lorenzi S. Onychomycosis caused by nondermatophytic molds: Clinical features and response to treatment of 59 cases. J Am Acad Dermatol 2000;42:217-224
Google Scholar
11. 11. White MI, Clayton YM. The treatment of fungus and yeast infections of nails by the method of 'chemical removal'. Clin Exp Dermatol 1982;7:273-276
Google Scholar
12. 12. Baran R, Tosti A. Chemical avulsion with urea nail lacquer. J Dermatolog Treat 2002;13:161-164
Google Scholar
13. 13. Gupta AK, Venkataraman M, Quinlan EM. Efficacy of lasers for the management of dermatophyte toenail onychomycosis. J Am Podiatr Med Assoc 2022;112:20-236
Google Scholar
14. 14. Gupta AK, Polla Ravi S, Haas-Neill S, Wang T, Cooper EA. Utility of devices for onychomycosis: A review. J Dermatolog Treat 2023;34:2265658
Google Scholar
15. 15. Gupta AK, Simpson FC, Heller DF. The future of lasers in onychomycosis. J Dermatolog Treat 2016;27:167-172
Google Scholar
16. 16. Bhatta AK, Keyal U, Wang X, Gellén E. A review of the mechanism of action of lasers and photodynamic therapy for onychomycosis. Lasers Med Sci 2017;32:469-474
Google Scholar
17. 17. Vural E, Winfield HL, Shingleton AW, Horn TD, Shafirstein G. The effects of laser irradiation on Trichophyton rubrum growth. Lasers Med Sci 2008;23:349-353
Google Scholar
18. 18. Gupta AK, Versteeg SG. A critical review of improvement rates for laser therapy used to treat toenail onychomycosis. J Eur Acad Dermatol Venereol 2017;31:1111-1118
Google Scholar
19. 19. Engelhardt-Zasada C, Prochacki H. Influence of tem- perature on dermatophytes. Mycopathol Mycol Appl 1972;48:297-301
Google Scholar
20. 20. Carney C, Cantrell W, Warner J, Elewski B. Treatment of onychomycosis using a submillisecond 1064-nm neo- dymium: yttrium-aluminum-garnet laser. J Am Acad Dermatol 2013;69:578-582
Google Scholar
21. 21. Hollmig ST, Rahman Z, Henderson MT, Rotatori RM, Gladstone H, Tang JY. Lack of efficacy with 1064-nm neodymium: yttrium-aluminum-garnet laser for the treat- ment of onychomycosis: A randomized, controlled trial. J Am Acad Dermatol 2014;70:911-917
Google Scholar
22. 22. Karsai S, Jäger M, Oesterhelt A, Weiss C, Schneider SW, Jünger M, et al. Treating onychomycosis with the short-pulsed 1064-nm-Nd:YAG laser: Results of a prospective randomized controlled trial. J Eur Acad Dermatol Venereol 2017;31:175-180
Google Scholar
23. 23. Sabbah L, Gagnon C, Bernier FE, Maari C. A randomized, double-blind, controlled trial evaluating the efficacy of Nd:YAG 1064 nm short-pulse laser compared with placebo in the treatment of toenail onychomycosis. J Cutan Med Surg 2019;23:507-512
Google Scholar
24. 24. Ahn HJ, Lee JW, Shin MK. Ultrastructural study of onychomycotic nail plate. J Mycol Infect 2025;30:117-119
Google Scholar
25. 25. Yazdanparast SA, Barton RC. Arthroconidia production in Trichophyton rubrum and a new ex vivo model of onychomycosis. J Med Microbiol 2006;55:1577-1581
Google Scholar
26. 26. Norrbrand L, Kölegård R, Keramidas ME, Mekjavic IB, Eiken O. No association between hand and foot tempera- ture responses during local cold stress and rewarming. Eur J Appl Physiol 2017;117:1141-1153
Google Scholar
27. 27. Essien J, Jonah I, Umoh A, Eduok S, Akpan E, Umoiyoho A. Heat resistance of dermatophyte's conidiospores from athletes kits stored in Nigerian University Sport's Center. Acta Microbiol Immunol Hung 2009;56:71-79
Google Scholar
28. 28. Apfelberg D, Rothermel E, Widtfeldt A, Maser MR, Lash H. Preliminary report on use of carbon dioxide laser in podiatry. J Am Podiatry Assoc 1984;74:509-513
Google Scholar
29. 29. Lim EH, Kim HR, Park YO, Lee Y, Seo YJ, Kim CD, et al. Toenail onychomycosis treated with a fractional carbon-dioxide laser and topical antifungal cream. J Am Acad Dermatol 2014;70:918-923
Google Scholar
30. 30. Bhatta AK, Keyal U, Huang X, Zhao JJ. Fractional carbon-dioxide (CO2) laser-assisted topical therapy for the treat- ment of onychomycosis. J Am Acad Dermatol 2016;74: 916-923
Google Scholar
31. 31. Zhou BR, Lu Y, Permatasari F, Huang H, Li J, Liu J, et al. The efficacy of fractional carbon dioxide (CO2) laser com- bined with luliconazole 1% cream for the treatment of onychomycosis: A randomized, controlled trial. Medicine (Baltimore) 2016;95:e5141
Google Scholar
32. 32. Lee SK, Kim HY, Lee JH, Lee UH, Kim MS. Real-world effectiveness of a fractional CO2 laser with topical anti- fungal agents for the treatment of onychomycosis. Dermatol Ther 2022;35:e15498
Google Scholar
33. 33. Lipner SR, Scher RK. Efinaconazole 10% topical solution for the topical treatment of onychomycosis of the toenail. Expert Rev Clin Pharmacol 2015;8:719-731
Google Scholar
34. 34. Zaki AM, Abdo HM, Ebadah MA, Ibrahim SM. Fractional CO2 laser plus topical antifungal versus fractional CO2 laser versus topical antifungal in the treatment of onycho- mycosis. Dermatol Ther 2020;33:e13155
Google Scholar
35. 35. Arora S, Ranjan E. Urea occlusion prior to single session fractional CO2 laser as a treatment in onychomycosis. Indian J Dermatol Venereol Leprol 2020;86:331
Google Scholar
36. 36. Ranjan E, Arora S, Sharma AS, Sharma N, Dabas R. Single-session fractional CO2 laser following urea occlu- sion in management of onychomycosis: A pilot study. Skin Appendage Disord 2023;9:268-274
Google Scholar
37. 37. Zhan P, Liu W. The changing face of dermatophytic infections worldwide. Mycopathologia 2017;182:77-86
Google Scholar
38. 38. Gupta AK, Versteeg SG, Shear NH, Piguet V, Tosti A, Piraccini BM. A practical guide to curing onychomycosis: How to maximize cure at the patient, organism, treat- ment, and environmental level. Am J Clin Dermatol 2019; 20:123-133
Google Scholar
39. 39. Gnat S, Łagowski D, Dyląg M, Zielinski J, Studziński M, Nowakiewicz A. Cold atmospheric pressure plasma (CAPP) as a new alternative treatment method for onychomycosis caused by Trichophyton verrucosum: in vitro studies. Infection 2021;49:1233-1240
Google Scholar
40. 40. Brun P, Bernabè G, Marchiori C, Scarpa M, Zuin M, Cavazzana R, et al. Antibacterial efficacy and mechanisms of action of low power atmospheric pressure cold plasma: Membrane permeability, biofilm penetration and antimicrobial sensitization. J Appl Microbiol 2018;125: 398-408
Google Scholar
41. 41. Rahimi-Verki N, Shapoorzadeh A, Razzaghi-Abyaneh M, Atyabi SM, Shams-Ghahfarokhi M, Jahanshiri Z, et al. Cold atmospheric plasma inhibits the growth of Candida albicans by affecting ergosterol biosynthesis and sup- presses the fungal virulence factors in vitro. Photo- diagnosis Photodyn Ther 2016;13:66-72
Google Scholar
42. 42. Bulson JM, Liveris D, Derkatch I, Friedman G, Geliebter J, Park S, et al. Non-thermal atmospheric plasma treatment of onychomycosis in an in vitro human nail model. Mycoses 2020;63:225-232
Google Scholar
43. 43. Heinlin J, Maisch T, Zimmermann JL, Shimizu T, Holzmann T, Simon M, et al. Contact-free inactivation of Tricho- phyton rubrum and Microsporum canis by cold atmos- pheric plasma treatment. Future Microbiol 2013;8:1097-1106
Google Scholar
44. 44. Shemer A, Daniel R, Kassem R, Geffen Y, Galili E. Cold sub-atmospheric and atmospheric pressure plasma for the treatment of Trichophyton rubrum onychomycosis: An in-vitro study. Dermatol Ther 2020;33:e14084
Google Scholar
45. 45. Safi-Samghabadi A, Atyabi SM, Razzaghi-Abyaneh M. Anti-dermatophytic activity of cold atmospheric plasma against Trichophyton rubrum via affecting fungal growth, morphology, drug susceptibility and HSP90 gene ex- pression. Sci Rep 2022;12:9481
Google Scholar
46. 46. Nikmaram H, Kanavi MR, Ghoranneviss M, Balagholi S, Ahmadieh H, Roshandel D, et al. Cold atmospheric pressure plasma jet for the treatment of Aspergillus keratitis. Clin Plasma Med 2018;9:14-18
Google Scholar
47. 47. Bernhardt T, Semmler ML, Schäfer M, Bekeschus S, Emmert S, Boeckmann L. Plasma medicine: Applications of cold atmospheric pressure plasma in dermatology. Oxid Med Cell Longev 2019;2019:3873928
48. 48. Lipner SR, Friedman G, Scher RK. Pilot study to evaluate a plasma device for the treatment of onychomycosis. Clin Exp Dermatol 2017;42:295-298
Google Scholar
49. 49. Lux J, Dobiáš R, Kuklová I, Litvik R, Scholtz V, Soušková H, et al. Inactivation of dermatophytes causing onycho- mycosis and its therapy using non-thermal plasma. J Fungi (Basel) 2020;6:214
Google Scholar
50. 50. Rashid A, Scott E, Richardson MD. Early events in the invasion of the human nail plate by Trichophyton mentagrophytes. Br J Dermatol 1995;133:932-940
Google Scholar
51. 51. Grover C, Khurana A. Onychomycosis: Newer insights in pathogenesis and diagnosis. Indian J Dermatol Venereol Leprol 2012;78:263-270
Google Scholar
52. 52. Elewski BE. Onychomycosis: Pathogenesis, diagnosis, and management. Clin Microbiol Rev 1998;11:415-429
Google Scholar
53. 53. Samsavar S, Mahmoudi H, Shakouri R, Khani MR, Molavi B, Moosavi J, et al. The evaluation of efficacy of atmospheric pressure plasma in diabetic ulcers healing: A randomized clinical trial. Dermatol Ther 2021;34: e15169
Google Scholar
54. 54. He R, Li Q, Shen W, Wang T, Lu H, Lu J, et al. The efficacy and safety of cold atmospheric plasma as a novel therapy for diabetic wound in vitro and in vivo. Int Wound J 2020;17:851-863
Google Scholar
Congratulatory MessageClick here!
