pISSN : 3058-423X eISSN: 3058-4302
Open Access, Peer-reviewed
pISSN : 3058-423X eISSN: 3058-4302
Open Access, Peer-reviewed

Ji Hyun Yi
10.17966/JMI.2026.31.1.1 Epub 2026 March 31
Abstract
Tropical island nations, characterized by high temperatures, humidity, and often limited healthcare infrastructure, present a unique spectrum of dermatological challenges. This review synthesizes clinical experiences from the largest dermatological public referral center in Fiji, Tamavua Twomey Hospital, to delineate the prevalence, presentation, and management of skin diseases in the South Pacific. Infectious dermatoses dominate the patient load, with fungal infections and scabies infestations being paramount public health concerns. I highlight the significant burden of Leprosy, which persists at a rate substantially higher than in developed nations, often presenting with severe, multi-bacillary forms and complications like recurrent erythema nodosum leprosum. Management is profoundly constrained by a limited national essential drug list, frequent medication stockouts, and the absence of diagnostic tools such as immunofluorescence examination and fungal culture. Furthermore, skin malignancies in the albino population often face delayed diagnosis and suboptimal treatment, leading to poor outcomes. Dermatological patients in Fiji face limited access to healthcare facilities, inadequate education regarding disease management, and financial barriers to acquiring essential medications, moisturizer and sunscreens. Consequently, their conditions frequently deteriorate and may progress to life-threatening stages. During my three years of practice, I have personally experienced four cases of death among patients with skin diseases. This review serves as a crucial documentation of the dermatological pathology and systemic healthcare hurdles in Fiji, advocating for enhanced international collaboration, improved drug supply chains, and specialized training to fortify the local dermatological capacity.
Keywords
Chromoblastomycosis Fiji Healthcare disparities Infectious dermatoses Leprosy Public health Scabies Tropical dermatology
The author participated in the Korea International Co- operation Agency Global Doctor Program, providing dermato- logical care and training dermatology specialists in Fiji for three years1. The Republic of Fiji, an island nation in the South Pacific approximately 8,000 km from the Korean Peninsula, differs in dermatological disease distribution and treatment approaches compared with Korea due to its hot, humid climate and socio-cultural characteristics as a developing country. This paper reviews clinical cases encountered during duties at Tamavua Twomey Hospital (TTH) in Fiji and reflects on dermatological challenges and future directions in resource-limited settings.
TTH was established in 1970 in the Tamavua area near Suva, Fiji's capital, to relocate leprosy patients previously isolated on Makogai Island. Initially focused on the treatment of leprosy and infectious diseases, it remains Fiji's sole specialized dermatology institution and serves as a key national referral center for skin diseases nationwide.
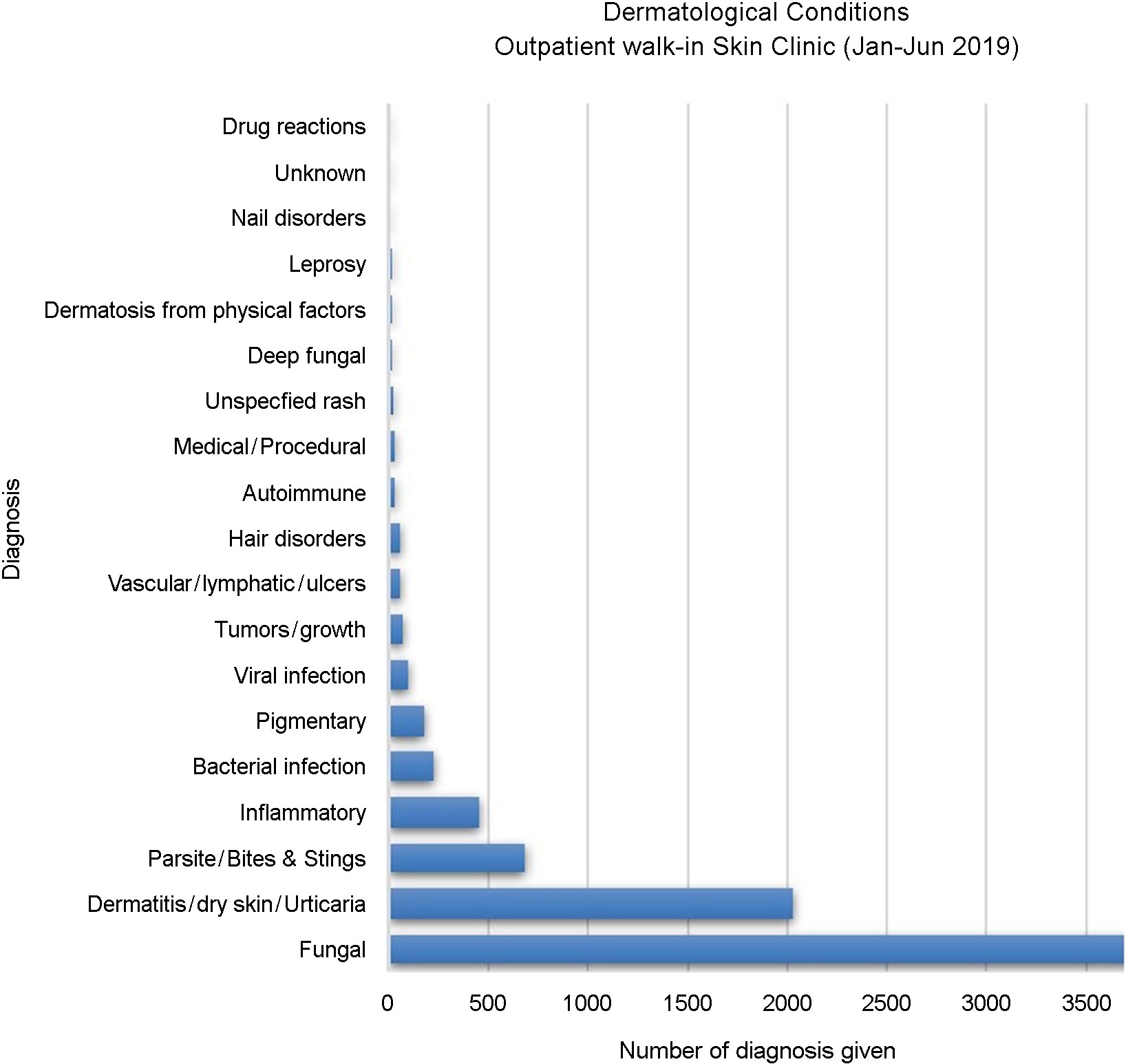
Clinical data from the TTH dermatology outpatient depart- ment reveal differences in disease prevalence compared with developed countries in temperate regions such as Korea. Analysis of TTH patient statistics showed that fungal infections were the most common skin disease, followed by allergic conditions, including dermatitis and urticaria, with parasitic infections (primarily scabies) ranking third. While the top ten conditions are similar to those seen in Korea, the pre- valence of the top three conditions in Korea is comparable, at 6.5-8% each, with fungal infections accounting for 7.0-7.8%2,3. In contrast, Fiji shows a markedly higher prevalence of fungal infections, exceeding 50% (see Fig. 1). Reports from the 1970s indicated that fungal infections accounted for 11.3-11.5% of dermatology outpatients in Korea, highlighting a substantial discrepancy compared with the prevalence observed in Fiji4,5. This high burden is attributed to the hot, humid environment, high household density, and a national culture centered on contact sports such as rugby, which facilitates transmission through sweat and close physical contact.
Fiji's healthcare system, shaped in part by its history as a British colony, follows a public model in which treatment and medications are provided free of charge and therefore relies heavily on the Fiji Essential Drugs List (EDL)6. Medications not included on the EDL, or those subject to early depletion or stockouts due to logistical constraints, cannot be provided. Moreover, most high-cost medications, including immuno- suppressants and biologics, are not listed on the EDL, and private pharmacies supplying them are difficult to access. These limitations substantially restrict dermatological treatment options. For example, antifungal agents such as itraconazole are often unavailable even in local private pharmacies, forcing clinicians to rely on older or less effective agents such as ketoconazole tablets. Despite being restricted or banned in developed countries because of hepatotoxicity, ketoconazole tablets remain widely used to treat pityriasis versicolor in Fiji.
Dermatological diagnostic capacity is also severely limited. Fungal cultures and immunofluorescence testing are unavail- able and, due to a shortage of pathologists, histopathology results typically require at least six weeks. As a result, many complex or potentially life-threatening conditions, including autoimmune bullous diseases and malignancies, are diag- nosed and managed primarily on the basis of clinical suspicion, increasing the risk of suboptimal outcomes.
Dermatology specialist staffing is also insufficient. Most patients depend on primary care physicians or intermittent outreach visits by doctors from TTH (approximately once every 2-3 months), leading to delayed diagnoses and inconsistent follow-up care.
3.1. Superficial fungal infections
Due to high temperatures and humidity, superficial fungal infections are ubiquitous in Fiji. Pityriasis versicolor, locally known as "Dani," is so prevalent that it is considered nearly universal.
Dermatomycoses, including tinea corporis and tinea capitis, are routinely encountered. Clinical manifestations are often severe, presenting as extensive, multiple lesions. Tinea capitis may progress to marked inflammatory reactions such as kerion, which were observed weekly at TTH. Griseofulvin remains the primary systemic treatment because of limited availability of newer agents such as terbinafine and itraconazole.
3.2. Endemic scabies
Scabies represents a major public health challenge in Fiji. In countries such as Fiji, families often have five or more children per household, and three or more generations frequently live together. Consequently, intrafamilial transmission of infectious diseases is common, with the national scabies prevalence in Fiji reported at 23.6%7. Symptoms are frequently complicated by secondary bacterial infections, including impetigo or furun- culosis. Severe forms, such as crusted scabies characterized by thick crusts and high mite density, are also observed and require active treatment with ivermectin.
A public health clinical trial in Fiji comparing mass drug administration strategies demonstrated that oral ivermectin (0.2 mg/kg) was more effective in reducing scabies prevalence and secondary bacterial infections than standard treatment or mass topical permethrin application8. These findings sup- port large-scale control efforts, including systemic treatment, despite a cost of $4.88 per person and ongoing supply chain challenges within public healthcare systems9.
Beyond common superficial infections, tropical environ- ments are associated with several unique and difficult-to-treat deep fungal infections.
4.1. Tinea imbricata
Tinea imbricata is a rare form of dermatophytosis pre- dominantly observed in tropical regions and uncommon in temperate climates. It is caused by Trichophyton concen- tricum10. Clinically, it is characterized by distinctive circular, concentric, layered, or wavy scaling patterns, often described as resembling roof tiles (Fig. 2).

To date, tinea imbricata has not been reported in Korea, and no cases have been documented in China since 2004. The estimated prevalence is approximately 9-18% in the Oceania region; in Fiji, prevalence varies by village and has been reported to range from 6-39. This condition is chronic and difficult to eradicate, often requiring prolonged systemic antifungal therapy12.
4.2. Chromoblastomycosis
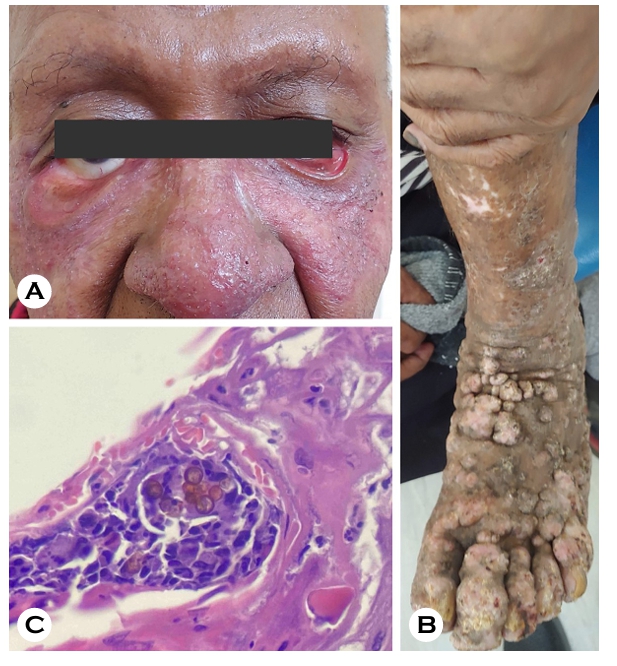
Chromoblastomycosis is a rare, chronic, progressive fungal infection of the skin and subcutaneous tissue caused by melanomycetes. Clinical manifestations are highly variable, including wart-like papules and plaques, hypertrophic raised plaques with central atrophy, and giant nodular masses13. In one severe case observed in Fiji, extensive facial lesions and scarring resulted in ptosis, while multiple nodular clusters appeared on the limbs and progressed to large masses (Fig. 3).
Diagnosis relies on identification of muriform cells, also termed "Medlar bodies," commonly found within Langhans giant cells on KOH preparation or histopathology (Fig. 3C). Treatment typically consists of surgical excision combined with high-dose or combination systemic antifungal therapy, including itraconazole and terbinafine. However, surgical in- tervention was difficult in extensive disease, and the required medications were not readily available. In such cases, alter- native approaches, including local hyperthermia using heating devices, were attempted based on previous reports14; how- ever, these methods were largely ineffective in extensive and chronic cases.
Despite global eradication efforts, TTH continues to man- age 5-20 new leprosy cases annually. Clinical presentations range from ill-defined hypopigmented macules with indistinct borders to sharply demarcated annular erythematous plaques, nodules, and severe multibacillary forms with peripheral nerve hypertrophy. All cases in this study were multibacillary leprosy.
In Fiji, leprosy is diagnosed based on clinical findings and slit-skin smear examination. This procedure involves collecting tissue fluid from the earlobes, elbows, knees, and represen- tative skin lesions to identify acid-fast bacilli.
Patients diagnosed with multibacillary leprosy receive a standard 12-month course of multidrug therapy (MDT)15. At diagnosis, patients are typically hospitalized for approximately one month to initiate treatment and receive education on disease management.
For the remaining 11 months, MDT is continued on an out- patient basis with support from local health centers. However, patients returning to remote islands often fail to complete the full 12-month treatment course, which is associated with serious complications, including retrogressive relapse, neuro- logical impairment (Fig. 4), and recurrent erythema nodosum leprosum. In such cases, prolonged hospitalization is required to ensure completion of therapy.

6.1. Bullous diseases
Autoimmune bullous diseases, such as bullous pemphi- goid, often present with typical tense blisters. However, definitive diagnosis was challenging in the field because direct immunofluorescence (DIF) testing was unavailable. One case clinically suspected of linear IgA dermatitis was treated with doxycycline based on clinical judgment. The absence of DIF prolonged diagnostic uncertainty in the management of auto- immune bullous diseases.
6.2. Skin cancer and albinism
The global prevalence of oculocutaneous albinism is esti- mated at approximately 1 in 17,000 to 1 in 20,000 individuals. In contrast, Fiji shows a markedly higher reported prevalence of approximately 1 in 70016. In isolated archipelagoes such as Fiji, the presence of an albinism gene mutation in a small founding population can lead to increased prevalence over successive generations. This phenomenon, known as the founder effect, is compounded by geographical isolation that restricts gene flow from external populations. Within small, closed communities, the likelihood of expressing autosomal recessive traits such as albinism increases due to higher rates of consanguinity17.
The substantially increased risk of malignant skin tumors in this population is driven by multiple factors, including in- tense ultraviolet radiation exposure related to tropical latitude, limited awareness of sun protection measures, and socioeco- nomic barriers that restrict access to affordable sunscreen and other photoprotective interventions.
In Fiji, three cases of malignant skin tumors associated with oculocutaneous albinism were documented, consisting primarily of squamous cell carcinoma and basal cell carcinoma (Fig. 5); malignant melanoma was not observed.
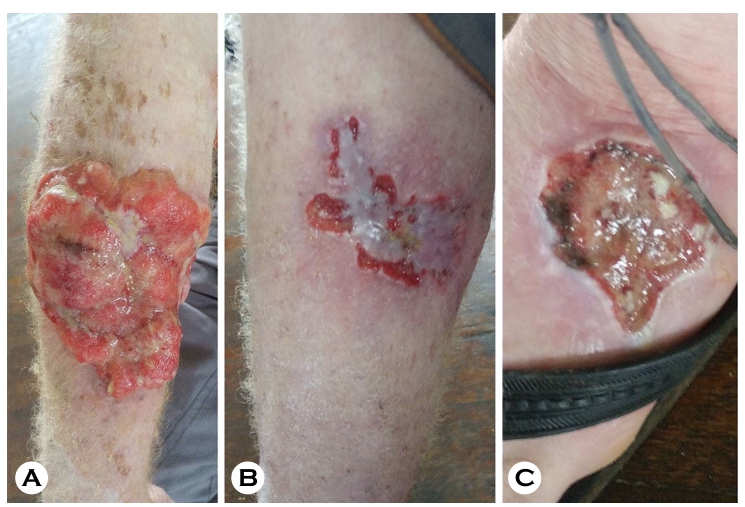
Most patients presented with advanced, ulcerative, and frequently metastatic disease that precluded curative surgical resection. In several cases, complete excision was not possible because of extensive metastasis, and one patient required palliative care and subsequently died from disease-related causes.
The burden of skin disease in Fiji demonstrates marked extremes in presentation and outcomes. Highly prevalent and largely preventable infectious dermatoses, such as superficial fungal infections, impetigo, and scabies, remain common, particularly in pediatric and community settings. Conversely, systemic and neoplastic conditions are frequently diagnosed at advanced stages, often precluding curative intervention and progressing to terminal disease.
These disparities arise from multiple interconnected factors, including limited access to specialist dermatological care, geographical and transportation barriers that delay referral to centralized facilities, and constraints in diagnostic infra- structure and the availability of appropriate therapeutic agents.
To address the severe shortage of trained dermatologists, international collaboration between Australian dermatologists and local stakeholders led to the establishment of the Pacific Dermatology Training Centre (PDTC) at TTH in 201918. The PDTC, in partnership with Fiji National University, provides structured postgraduate training programs, beginning with a one-year Postgraduate Diploma in Dermatology and pro- gressing to a three-year Master of Medicine (MMed) in Der- matology. The first cohort of diploma trainees was enrolled in 2019, and included participants from Fiji and other Pacific Island nations including Samoa, Kiribati, and the Solomon Islands. Recent reports indicate that 11 physicians have com- pleted the diploma program, and the inaugural cohort of MMed trainees, primarily from Fiji, is expected to graduate as fully qualified dermatology specialists in late 2024, repre- senting a significant milestone in regional capacity building19.
Future international and regional efforts should extend beyond direct clinical service provision to prioritize sustainable infrastructure strengthening. Key priorities include:
1) Ensuring a reliable and affordable supply chain for essential dermatological medications and photoprotective agents, such as broad-spectrum sunscreens, particularly for high-risk populations including individuals with oculocutaneous albinism.
2) Developing a centralized and functional diagnostic pipeline, including enhanced histopathology, dermoscopy, and teledermatology capabilities, to facilitate earlier detection of neoplastic lesions.
3) Continued investment in long-term, regionally appropriate training programs at the PDTC and similar centers to cultivate local expertise and reduce dependence on ex-ternal specialists.
4) Strategic decentralization of dermatological services, with trained specialists deployed to regional and divisional hospitals to improve access for underserved rural and outer-island populations.
By addressing these structural gaps through collaborative capacity-building initiatives, morbidity and mortality associated with advanced skin diseases in Fiji and the broader Pacific region may be substantially reduced, advancing progress toward equitable dermatological care.
References
1. https://koica.go.kr/koica_kr/951/subview.do
2. Lee SY, Choi HG, Ro BI, Cho HK. A statistical study of dermatoses in Goyang City (2009-2013). Korean J Dermatol 2015;53:106-112
Google Scholar
3. Choi JW, Ahn SK. A statistical study of dermatoses in Kangwon province, 2010-2014. Korean J Dermatol 2016; 54:26-34
Google Scholar
4. Huh KS, Kahng JB, Chun IK, Kim YP. A statistical study of dermatoses (1971-1980). Korean J Dermatol 1982;20: 59-68
Google Scholar
5. Bang DS, Cho SK, Lee SN. A statistical study of dermatoses during the last 5 years (1976-1980). Korean J Dermatol 1983;21:37-44
Google Scholar
6. https://health.gov.fj/wp-content/uploads/2018/02/Fiji-Essential-Medicines-List-4th-Edition-2015-.pdf
7. Romani L, Koroivueta J, Steer AC, Kama M, Kaldor JM, Wand H, et al. Scabies and impetigo prevalence and risk factors in Fiji: A national survey. PLoS Negl Trop Dis 2015; 9:e0003452
Google Scholar
8. Romani L, Whitfeld MJ, Koroivueta J, Kama M, Wand H, Tikoduadua L, et al. Mass drug administration for scabies control in a population with endemic disease. N Engl J Med 2015;373:2305-2313
Google Scholar
9. Mow M, Thean LJ, Parnaby M, Mani J, Rafai E, Sahukhan A, et al. Costs of mass drug administration for scabies in Fiji. PLoS Negl Trop Dis 2022;16:e0010147
Google Scholar
10. Hay RJ. Tinea imbricata. Curr Top Mycol 1988;2:55-72
11. Er YX, Lee SC, Than LT, Muslim A, Leong KF, Kwan Z, et al. Tinea imbricata among the indigenous communities: Current global epidemiology and research gaps asso- ciated with host genetics and skin microbiota. J Fungi (Basel) 2022;8:202
Google Scholar
12. James WD, Berger TG, Elston DM. Andrew's diseases of the skin clinical dermatology. 10th ed. Philadelphia: WB Sauders, 2006:303
Google Scholar
13. Queiroz-Telles F, de Hoog S, Santos DW, Salgado CG, Vicente VA, Bonifaz A, et al. Chromoblastomycosis. Clin Microbiol Rev 2017;30:233-276
Google Scholar
14. Hidayah RMN, Gunawan H, Fauziah N, Rianty F. Electric heating pad as an adjuvant treatment of extensive chromoblastomycosis in immunocompetent patient: A case report. Int Med Case Rep J 2025;18:315-320
Google Scholar
15. Scollard DM, Adams LB, Gillis TP, Krahenbuhl JL, Truman RW, Williams DL. The continuing challenges of leprosy. Clin Microbiol Rev 2006;19:338-381
Google Scholar
16. https://www.ohchr.org/en/statements-and-speeches/ 2017/12/statement-united-nations-independent-expert-enjoyment-human-rights
17. Johanson HC, Chen W, Wicking C, Sturm RA. Inheritance of a novel mutated allele of the OCA2 gene associated with high incidence of oculocutaneous albinism in a Polynesian community. J Hum Genet 2010;55:103-111
Google Scholar
18. https://pacificdermatology.org.au/
19. Whitfeld M, Wallace M, Nash E, Yeon J, Wilson A, Kama M, et al. Pacific Dermatology Training Centre 2024 update. Australas J Dermatol 2024;65(Suppl. 1):42-44
Congratulatory MessageClick here!
