pISSN : 3058-423X eISSN: 3058-4302
Open Access, Peer-reviewed
pISSN : 3058-423X eISSN: 3058-4302
Open Access, Peer-reviewed

Bok Won Park,Min Kyun An,Eun Byul Cho,Eun Joo Park,Kwang Ho Kim,Kwang Joong Kim
10.17966/JMI.2018.23.3.74 Epub 2018 September 28
Abstract
A 76-year-old female presented with a 2-month history of skin lesions on both her buttocks. The skin lesions showed diffuse, erythematous scattered papules and macules with brown to black crusts. The patient believed that she had skin cancer and that the lesions had to be scrapped. She thus soaked her buttock in sikhye, a traditional Korean beverage, to treat the lesions. Based on patient history, she was diagnosed with dermatitis artefacta at the initial hospital visit. KOH examination was positive for hyphae and fungal cultures of Saccharomyces cerevisiae. She was treated with oral and topical antifungal agents for 6 months. The skin lesions improved at that time; however, she continued to scratch her buttock, and the skin lesions aggravated. Repeat fungal culture of the lesions revealed Candida glabrata, which was confirmed by genetic polymerase chain reaction sequencing. Consequently, she was treated with antifungal agents for 6 months. S. cerevisiae is widely used in baking, brewing, wine making, and biotechnology. S. cerevisiae and C. glabrata are considered relatively non-pathogenic fungal organisms. Here, we report a rare case of dermatitis artefacta combined with superficial infection of non-pathogenic fungal organism.
Keywords
Candida glabrata Dermatitis artefacta Saccharomyces cerevisiae
Dermatitis artefacta (DA) is a skin disorder resulting from deliberately self-inflicted skin lesions, while patients repudiate all responsibility for their occurence1. Such skin lesions arise from an urge to satisfy a psychological need, most commonly an urge to receive medical treatment. DA presents a variety of clinical manifestations depending on the patient's creativity and the method used to cause the lesion. The most common skin lesions observed in DA include excoriation, ulcers, blisters, panniculitis, localized crusting, eczematous lesions, edemas, purpuras, and bruises1.
S. cerevisiae is broadly used in baking, brewing, wine making, and biotechnology; in addition, it was previously regarded as a non-pathogenic organism. However, recent evidences indicate that S. cerevisiae may cause superficial as well as systemic diseases2,3.
C. glabrata has also been considered a relatively non-pathogenic fungal organism of human mucosal tissues. However, mucosal and systemic infections caused by C. glabrata have significantly increased in response to the increased use of immunosuppressants4. Currently, C. glabrata is the second and third causative agent of superficial and systemic candidal infections4,5, respectively.
These two organisms usually cause superficial mucosal (oral, esophageal, vaginal, or urinary) infections3,4. However, in the present case, these organisms caused a superficial infection on the buttocks owing to the presence of DA. Herein, we report a unique case of superficial fungal infection resulting from the psychological belief of the patient.
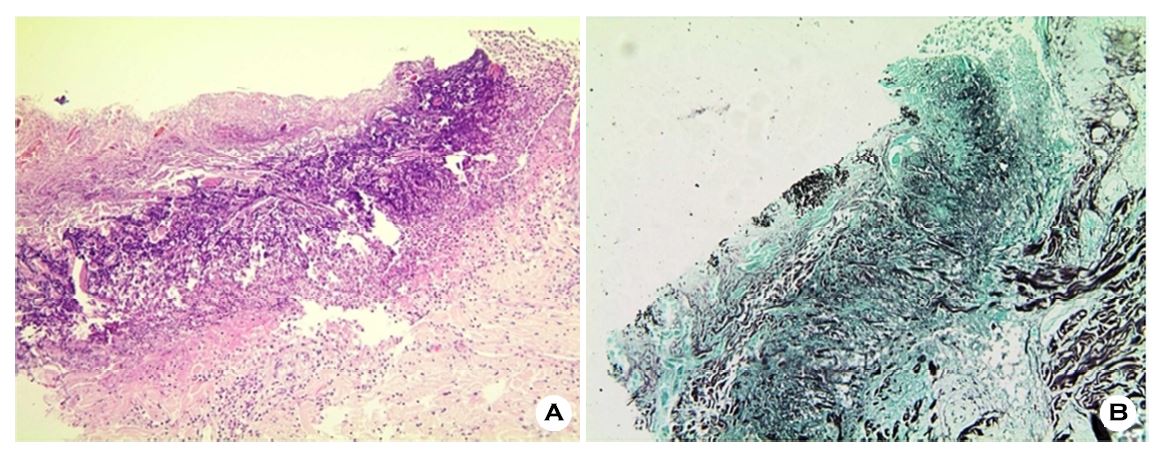
A 76-year-old female presented to our clinic with itchy and painful skin lesions on her buttocks (Figure 1A). Two months prior to admission, she insisted that she had skin cancer on her buttocks and kept scratching her buttocks to remove it. She also soaked her buttocks in hot sikhye, a traditional Korean beverage. She was referred to a psychiatrist for schizophrenia; however, she refused to receive treatment. Diffuse, erythematous scattered papules and macules with ulcerations and crusts were observed on her buttocks (Figure 1A). Skin biopsy was performed, and histological findings demonstrated epidermal necrosis, lymphohistiocytic infiltration in the superficial dermis, marked fibrotic change in the dermis, and presence of fungal spores in the superficial dermis (Figure 2A). Periodic acid Schiff and Gomori's methenamine silver staining confirmed the presence of fungal spores in the superficial dermis (Figure 2B). Bacterial and fungal cultures identified E. coli and S. cerevisiae, respectively.
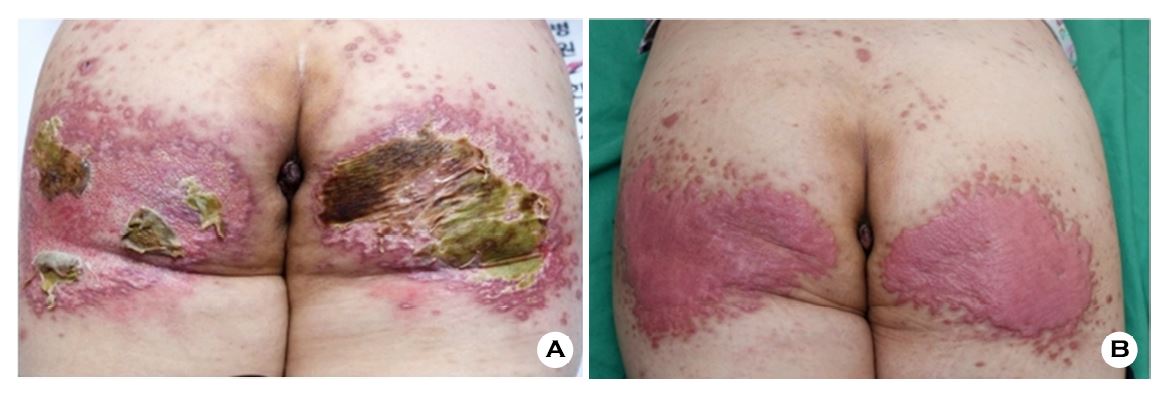
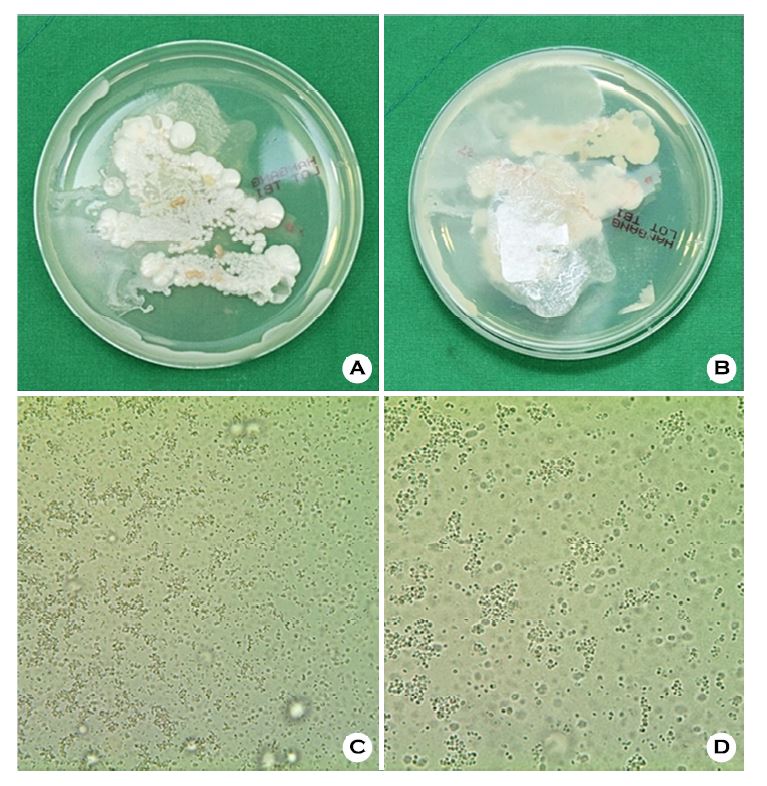
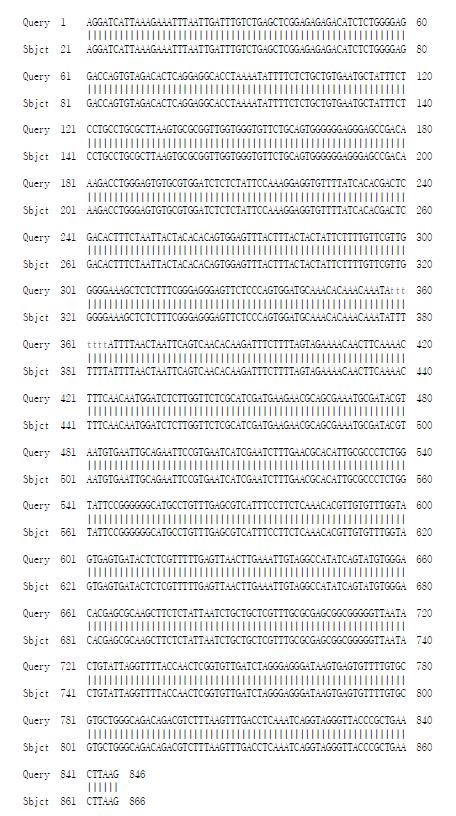
Based on the clinical and histological findings, she was diagnosed with DA with a superficial fungal infection. She was treated with ciprofloxacin 500 mg/day, itraconazole 100 mg/ day, topical flutrimazole, and topical fusidic acid for 3 months. Her skin lesions improved with the development of hyper-trophic scarring, and the treatment was subsequently discontinued (Figure 1B). However, 3 months after treatment termination, she revisited the hospital with aggravated skin lesions. She had been scratching and soaking her buttocks in various fluids owing to her delusional belief that she had skin cancer. Fungal and bacterial culturing was repeated, which showed positive results for C. glabrata (Figure 3). C. glabrata was con- firmed with rDNA ITS sequencing (Figure 4). Subsequently, she was treated with fluconazole 50 mg/day and topical flutrimazole for 3 months, following which the skin lesions improved with development of hypertrophic scars.
DA is a skin disorder caused by the deliberate production of skin lesions owing to the patient's underlying psychological disorder. The management of patients with DA is demanding as they usually refuse treatment due to their inability to recognize their underlying psychological disorder. However, careful exclusion of primary dermatological disease is important1,6.
Although it is primarily a dermatological diagnosis, cooperation with a psychiatrist is essential for appropriate management. When treating a dermatological condition, it is helpful to prescribe medications as they provide the patient with some contentment that "something is being done to me", potentially ceasing the destructive behavior responsible for lesion occurence1. As a therapeutic and preventive tool, occlusion of the skin lesion is also helpful7.
Cognitive behavioral therapy and psychotherapy have been successfully applied to manage psychological problems in such patients. Serotonin pathways are known to play an essential role in the mechanism of self-destructive behavior1,8. In addition, they are involved in obsessive-compulsive disorders, anxiety disorders, and depression8. In this context, selective serotonin reuptake inhibitors may be used in DA patients with obsessive-compulsive disease or any depressive disorder. The prognosis is uncertain and most likely linked to the type of underlying psychiatric or psychosocial problem.
S. cerevisiae is widely distributed in nature and has broad applications in various fields, including biotechnology. However, in recent years, there has been an increased incidence of clinical infections caused by S. cerevisiae2,8. Although regarded as non-pathogenic, recent evidences2,8-10 indicate that it may cause superficial and systemic diseases, particularly in immunocompromized individuals. Since the use of immunosuppressants has increased in recent years, S. cerevisiae is currently considered as an opportunistic pathogen of low virulence rather than a non-pathogenic yeast.
The most common superficial infection caused by S. cerevisiae is vaginitis. Studies10,11 revealed that S. cerevisiae was the causative agent of vaginitis in 0.45~1.06% of reported cases. However, in the present case, S. cerevisiae caused a superficial fungal infection on the buttocks and not the mucosa. The patient soaked her buttocks in sikhye that is produced using S. cerevisiae. The resultant superficial infection by S. cerevisiae may have aggravated the self-inflicted skin lesions.
C. glabrata is also one of the main causative organisms of vaginitis. Reportedly, S. cerevisiae is frequently detected in association with C. glabrata10. In this case, rDNA ITS sequencing was performed only for C. glabrata and not for S. cerevisiae. Considering this, C. glabrata may have been present since the initial presentation. Currently, there are data available regarding the relationship between these two organisms. In humans, C. glabrata and S. cerevisiae can be found as normal components of the gastrointestinal tract, resulting in co-infection10.
In conclusion, the underlying psychological disorder of the patient led to superficial fungal infection by S. cerevisiae and C. glabrata. Furthermore, a few cases of systemic infections caused by these two organisms have been reported. Therefore, physicians should not overlook these fungi, which were previously considered non-pathogenic, during diagnosis.
In relation to this article, I declare that there is no conflict of interest.
References
1. Mohandas P, Bewley A, Taylor R. Dermatitis artefacta and artefactual skin disease: the need for a psychodermato- logy multidisciplinary team to treat a difficult condition. Br J Dermatol 2013;169:600-606
Crossref
Google Scholar
PubMed
2. Romanio MR, Coraine LA, Maielo VP, Abramczyc ML, Souza RL, Oliveira NF. Saccharomyces cerevisiae fungemia in a pediatric patient after treatment with probiotics. Rev Paul Pediatr 2017;35:361-364
Crossref
Google Scholar
3. Murphy A, Kavanagh K. Emergence of Saccharomyces cerevisiae as a human pathogen: implications for biotechnology. Enzyme Microb Technol 1999;25:551-557
Crossref
Google Scholar
4. Fidel PL Jr, Vazquez JA, Sobel JD. Candida glabrata: review of epidemiology, pathogenesis, and clinical disease with comparison to C. albicans. Clin Microbiol Rev 1999;12:80 -96
Crossref
Google Scholar
5. Mtibaa L, Fakhfakh N, Kallel A, Belhadj S, Belhaj Salah N, Bada N, et al. Vulvovaginal candidiasis: Etiology, symptomatology and risk factors. J Mycol Med 2017;27:153-158
Crossref
Google Scholar
6. Rogers M, Fairley M, Santhanam R. Artefactual skin disease in children and adolescents. Australas J Dermatol 2001;42:264-270
Crossref
Google Scholar
PubMed
7. Fruensgaard K. Psychotherapeutic strategy and neurotic excoriations. Int J Dermatol 1991;30:198-203
Crossref
Google Scholar
PubMed
8. Jermain DM, Crismon ML. Pharmacotherapy of obsessive-compulsive disorder. Pharmacotherapy 1990;10:175-198
Crossref
PubMed
9. Enache-Angoulvant A, Hennequin C. Invasive Saccharomyces infection: a comprehensive review. Clin Infect Dis 2005;41:1559-1568
Crossref
Google Scholar
10. Sobel JD, Vazquez J, Lynch M, Meriwether C, Zervos MJ. Vaginitis due to Saccharomyces cerevisiae: epidemiology, clinical aspects and therapy. Clin Infect Dis 1993;16:93-99
Crossref
Google Scholar
11. Nyirjesy P, Vazquez JA, Ufberg DD, Sobel JD, Boikov DA, Buckley HR. Saccharomyces cerevisiae vaginitis: transmission from yeast used in baking. Obstet Gynecol 1995; 86:326-329
Crossref
Google Scholar
Congratulatory MessageClick here!
