pISSN : 3058-423X eISSN: 3058-4302
Open Access, Peer-reviewed
pISSN : 3058-423X eISSN: 3058-4302
Open Access, Peer-reviewed

Hee Chan Yang,Min Jae Kim,Je-Ho Mun
10.17966/JMI.2022.27.4.89 Epub 2023 January 04
Abstract
Keywords
Serratia marcescens Squamous cell carcinoma Tinea capitis
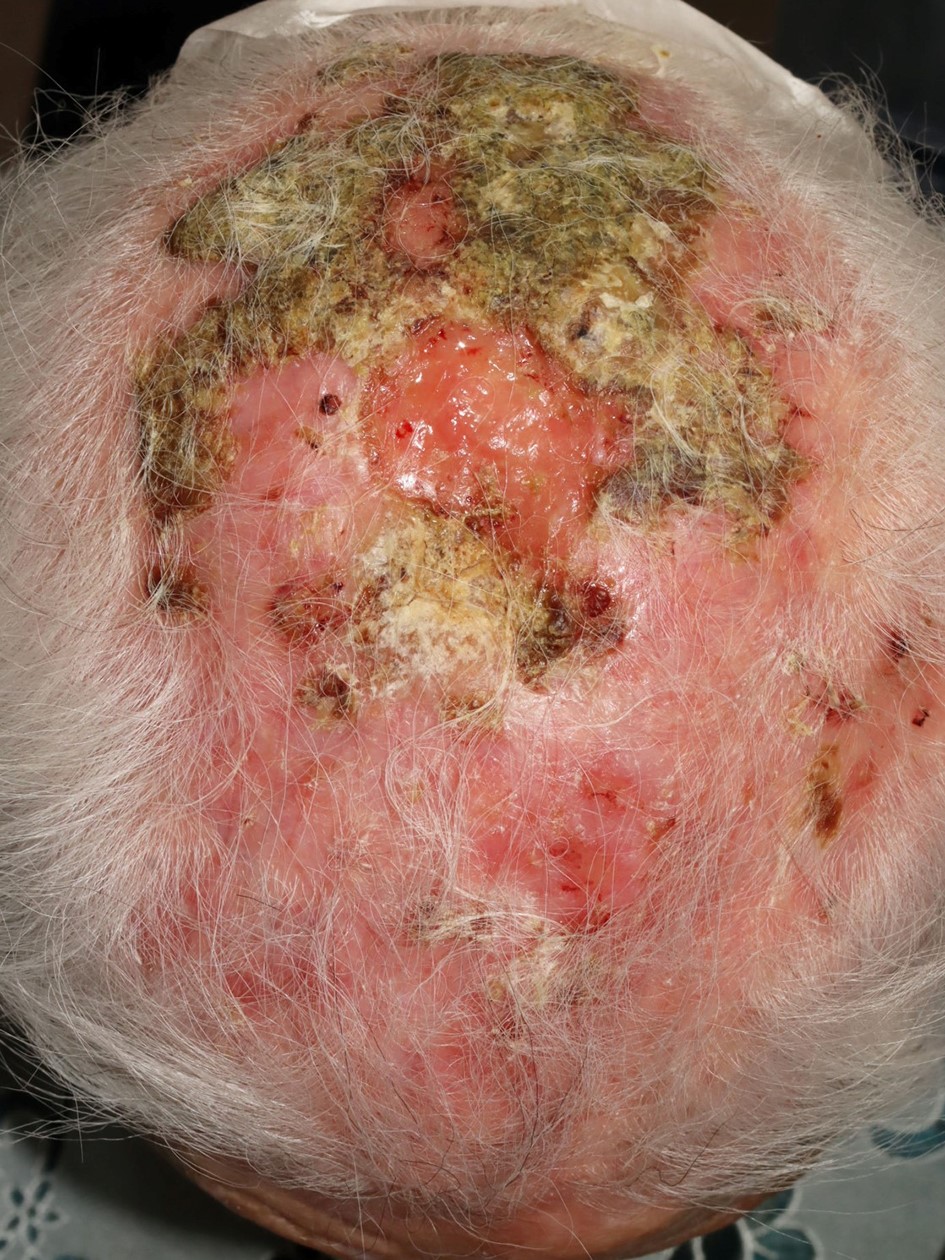
A 90-year-old woman presented with diffuse erythematous patches with geographic greenish-to-yellow oozy scales, crusts, ulcers, and hair loss on the scalp (Fig. 1). The patient has a history of being treated under seborrheic dermatitis for a 3-year history of scalp pruritus. The differential diagnosis included tinea capitis, pyoderma, seborrheic dermatitis, and squamous cell carcinoma (SCC).
Microscopy with 10% potassium hydroxide revealed the presence of hyphae and bacterial culture identified Serratia marcescens. Histopathologic findings of three punch biopsies from an ulcer, erythematous patch, and yellowish-crusted plaque showed dense infiltration of inflammatory cells in the dermis and atypical keratinocytes in the epidermis. However, no dermal invasion by atypical keratinocytes was observed. The dysplasia of epidermal keratinocytes may be due to an inflammatory response or malignant change. Oral antibiotics and topical antifungal medications were initially prescribed. Although four weeks of treatment resulted in partial impro- vement of the redness and scales on the scalp, SCC could not be excluded. Therefore, two further meticulous incisional biopsies were performed and confirmed the diagnosis of SCC.
The clinical features of tinea capitis, such as dandruff and itching sensation, are similar to that of seborrheic dermatitis, sometimes making it difficult to distinguish between those conditions1. SCC is an important addition to the differential for elderly individuals with crusty lumps on the scalp. In the present case, tinea capitis and secondary bacterial infection with S. marcescens resulted in exudative crusts and inflamed scalp, making the SCC diagnosis difficult2,3. Although no causal relationship could be demonstrated in the patient, con- comitant fungal and bacterial infections complicated and delayed the diagnosis of SCC.
This case highlights the importance of retaining clinical suspicion for a masked cutaneous malignancy in elderly patients with skin infections.
References
1. Elewski BE. Tinea capitis: a current perspective. J Am Acad Dermatol 2000;42:1-20
Google Scholar
2. Seo J, Shin D, Oh SH, Lee JH, Chung KY, Lee MG, et al. Cutaneous Serratia marcescens infections in Korea: a retrospective analysis of 13 patients. J Dermatol 2016;43: 149-155
Google Scholar
3. Brothers RP, Daveluy SD. Squamous cell carcinoma mimicking fungal infection. IDCases 2016;6:72-73
Google Scholar
Congratulatory MessageClick here!
