pISSN : 3058-423X eISSN: 3058-4302
Open Access, Peer-reviewed
pISSN : 3058-423X eISSN: 3058-4302
Open Access, Peer-reviewed
You Bum Song,Jun Gyu Song,Moo Kyu Suh,Gyoung Yim Ha,Jin Hwa Choi
http://dx.doi.org/10.17966/KJMM.2015.20.1.6 Epub 2015 September 17
Abstract
Onychomycosis is caused by dermatophytes usually, but some species of nondermatophytic molds and yeasts are also associated with invasion of nails. Aspergillus sydowii is a nondermatophytic mold which is opportunistic filamentous fungus in all environments. We report a case of onychomycosis caused by A. sydowii in a 65-year-old male. The patient showed yellowish discoloration with hyperkeratotic change on the distal and lateral portion of both great toenails. Direct microscopic examination of scraping on the potassium hydroxide preparation revealed dichotomous septate hyphae and repeated cultures on Sabouraud dextrose agar showed the same blue green velvety colonies. Biseriate phialides that cover entire vesicle with conidial structure resembling Penicillium were shown in the slide culture. The DNA sequence of internal transcribed spacer (ITS) region of clinical sample was 99% match to that of A. sydowii strain XWSFJJ1 (GenBank accession number FJ461692). We confirmed A. sydowii by KOH mount, colony, light microscopic morphology and DNA sequence analysis. The patient was treated with 250 mg oral terbinafine daily and topical 5% amorolfine nail lacquer for 3 months.
Keywords
Aspergillus sydowii Toenail onychomycosis
서 론
손발톱진균증은 손발톱의 진균성 감염증으로 그 원인균은 피부사상균 (dermatophytes)이 대부분이지만 비피부사상균성 사상균 (nondermatophyticmold)이나 효모균 (yeasts)에 의해 유발되기도 한다. 손발톱진균증을 야기하는 비피부사상균성 사상균으로 Aspergillus 균종, Scopulariopsis 균종, Fusarium 균종, Acremonium 균종 등이 있다[1]. 이러한 균들은 오염균이나 기회감염균으로 간주되어 쉽게 간과되어 왔지만 최근의 면역기능의 저하를 가져오는 많은 질환 및 환경적 변화와 더불어 중요성이 증가되고 있다. 최근 비피부사상균성 사상균에 의한 손발톱진균증의 유병율은 점점증가되고 있으며 이것은 이런 균들을 잠재적으로 원인균으로 보는 인식의 증가와 진단적 기술의 발달과 관련이 있다고 알려져 있다[2]. 손발톱진균증 중 Aspergillus 균종에 의한 손발톱진균증은 국외에서 보고자에 따라 2.6~6.1%로 다양하게 보고되고 있다[3],[4],[5],[6]. 국내 피부과 문헌상 A. sydowii에 의한 손발톱진균증은 1968년 Suh 등[7]이 처음 보고한 이후 2001년 Suh 등[8]이 1예를 추가하여 현재까지 총 2예 보고밖에 없어 드물지만, 손발톱진균증에서 A. sydowii가 분리되었을 때 오염균으로 간과해서는 안될 것으로 생각된다.
이에 저자들은 65세 남자 손발톱진균증 환자에서 임상, 진균배양, 광학 현미경 소견 및 분자생물학적 분석으로 A. sydowii에 의한 발톱 손발톱진균증으로 진단하고 드문 증례로 생각되어 문헌고찰과 함께 보고한다.

증 례
환 자: 김 O O, 65세, 남자
주 소: 양측 발의 소양감을 동반한 인설성 홍반성 반과 양측 모든 발톱의 황색 변색
현병력: 양극성 장애로 본원 정신과에 입원 중이었으며 약 10년 전부터 발톱의 황색 변색이 있었고, 양측 첫 번째 발톱의 원위외측부에서는 비후된 소견을 보여 의뢰되었다.
과거력: 특이 사항 없음
가족력: 특이 사항 없음
이학적 소견: 피부 소견 외 특이 사항 없음
피부 소견: 양측 발에 인설성 홍반성 반과 양측 모든 발톱의 황색 변색이 보이고 양측 첫 번째발톱의 원위부는 비후된 소견을 보였다 (Fig. 1).
검사실 소견: 일반혈액 및 말초혈액도말검사, 대소변검사, 매독혈청검사, 간기능 및 신기능 검사, 간염 항원 항체 검사, HIV검사, 흉부 X-선 검사, 심전도는 모두 정상범위내지 음성을 보였다.
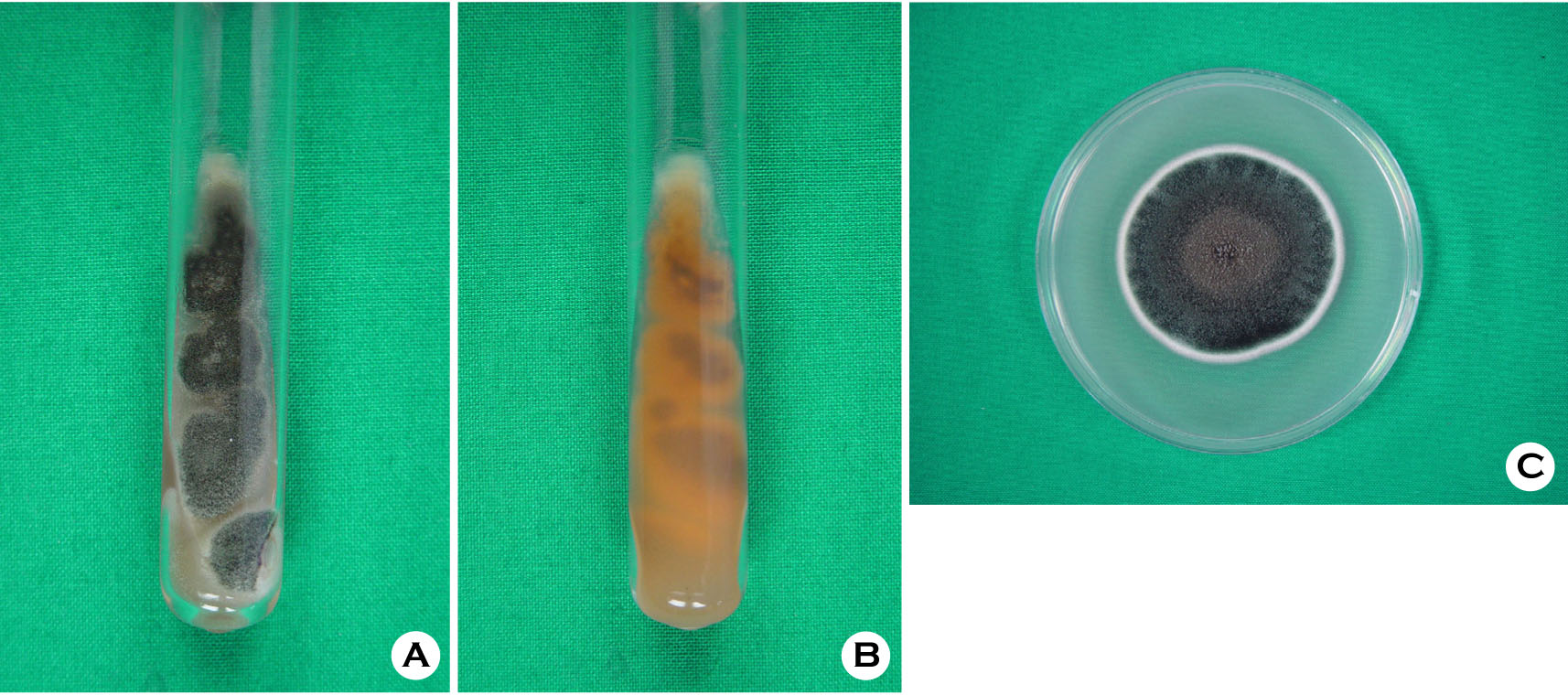
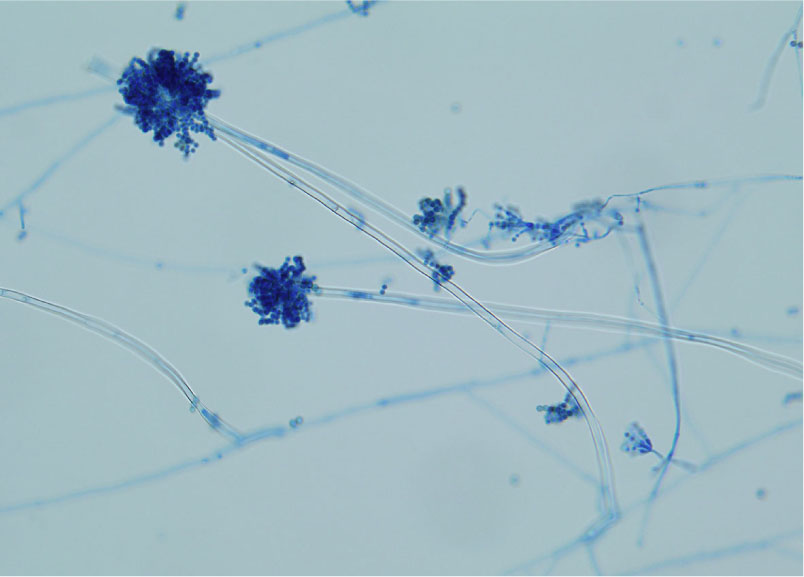
진균학적 소견: 병변부 손발톱의 potassium hydroxide (KOH) 검사상 두 갈래로 갈라진 분절균사를 관찰할 수 있었으며, Sabouraud dextrose agar (SDA)에 접종하여 25℃에서 1주간 배양한 결과 4개의 동일한 청녹색의 균집락이 관찰되었고, 각 집락의 경계부는 흰색을 띄었다. 배지의 뒷면은 노란색의 착색이 보였고, 평판배지에 계대배양 하였을 때도 동일한 소견을 보였다 (Fig.2A, B, C). 이 집락을 슬라이드 배양표본을 만들어 Lactophenol cotton blue로 염색하여 현미경 관찰상 유리질의 격막 균사 (hyaline septate hyphae)를 보이며, 구상의 정낭 (vesicle)과 방사상 2단경자 (biseriated phialides)의 끝에 분생포자가 전구상을 덮고 있으며, Penicillium 균종을 닮은 분생포자를 관찰할 수 있었다 (Fig. 3).
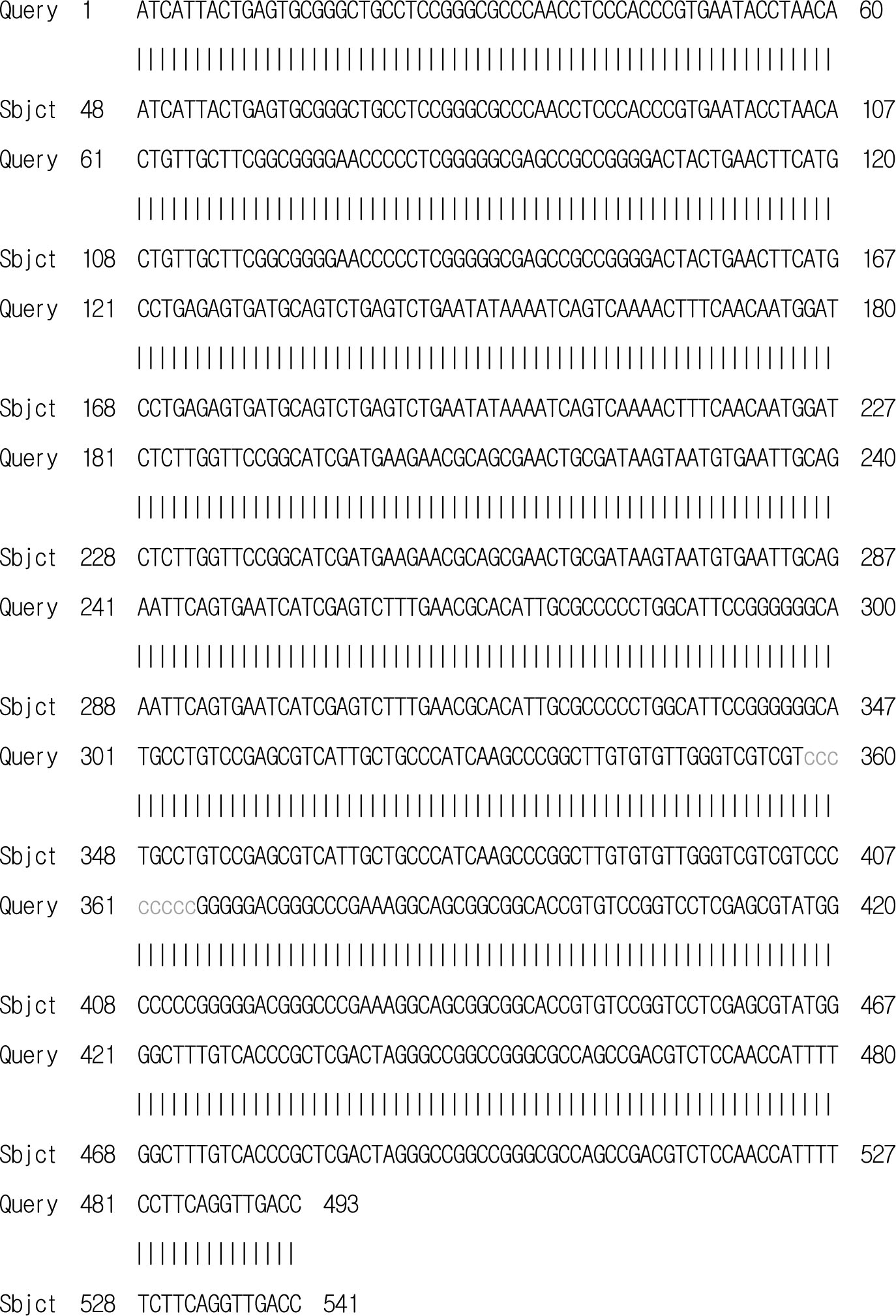
분자생물학적 분석: 환자의 배양된 균집락으로 부터 DNA를 분리하여 internal transcribed spacer (ITS) 부위의 염기서열을 얻은 후 Blast를 이용하여 GenBank에 있는 A. sydowii strain XWSFJJ1 (GenBank accession number FJ461692)의 ITS 부위의 염기서열과 비교한 결과 99% 일치하였다 (Fig.4). 이상의 KOH 소견, 진균배양, 광학 현미경 소견, 그리고 ITS 부위의 염기서열 분석으로 A.sydowii로 동정하였다.
치료 및 경과: 3개월간 terbinafine 1일 250 mg경구 투여와 5% amorolfine nail lacquer의 도포로 치료하였다.
고 찰
손발톱진균증은 피부사상균, 비피부사상균성 사상균, 그리고 효모균 등에 의해 유발되는 손발톱의 진균성 감염증으로 전체 손발톱질환의 약 20%를 차지하는 흔한 감염증이다[1]. 피부사상균을 제외한 비피부사상균성 사상균에 의한 손발톱진균증은 손발톱진균증의 1.5~17.6%를 차지하며, Aspergillus 균종, Scopulariopsis 균종, Fusarium 균종, Acremonium 균종 등이 원인이 될 수 있다[5],[9],[10],[11],[12].
Aspergillus 균종은 공기 토양 등 인류의 주거공간에 전 세계적으로 분포하는 진균으로 지금까지 약 900여종이 발견되었다[13]. Aspergillus 균종에 의한 손발톱진균증은 아마도Aspergillus 균종이 피부사상균과는 달리 각질친화적 (keratonophilic)이지 않기 때문에 족부 외상이나 또는 다양한 이전의 선행질환 후 이차적인 감염에 의해서 초래 되지만[14], 몇몇 연구들은 손발톱진균증의 1차 원인균으로 Aspergillus 균종을 보고하였다[15],[16]. Aspergillus 균종에 의한 손발톱진균증은 국외에서 보고자에 따라 2.6~6.1%로 다양하게 보고되고 있으며[3],[4],[5],[6], 국내에서는 Aspergillus 균종에 의한 손발톱진균증은 Lim 등[9]에 의해서 4.6%로 보고되고 있다. 이처럼 많은 차이를 보이는 이유는 비피부 사상균성 사상균의 분포의 지역적 차이, 비피부 사상균성 사상균에 의한 손발톱진균증의 진단에 있어서 다른 기준의 적용, 비피부사상균성 사상균의 배양에 있어서 부적절한 진균학적 방법의 사용 등에 기인한다고 한다[10].
기회감염균 (opportunistic filamentous fungus)인 A. sydowii는 주로 침습성 아스페루길루스증 (invasive aspergillosis), 손발톱진균증, 각막진균증 등 을 일으킨다고 보고되었다[13],[17]. Hwang 등[18]은 A. sydowii가 피부사상균을 제외한 비피부사상균성 사상균에 의한 손발톱진균증의 1.7%를 차지하는것으로 보고하였다.
Aspergillus 균종은 오염이 가능한 균이므로 감염된 손발톱에서 시행한 배양에서 Aspergillus 균종이 동정되었을 때 이것이 원인균인지 또는 단지 오염균인지 구별하는 것은 어렵다. 그래서 1976년 English[19]는 비피부사상균성 사상균이 배양되면 현미경 검사에서 균사, 또는 포자가 발견되고, 비피부사상균성 사상균에 의한 감염은 반복적인 배양검사에서 같은 균주가 동정될 때만손발톱진균증의 원인균으로 간주할 수 있다고 하였으며, 최근에는 균주의 진균핵내 ITS 부위의 염기서열 분석이 진단이 어려운 손발톱진균증의 확진에 보조적으로 유용하게 사용되고 있다[14],[20]. 전통적으로 원인균의 동정은 형태학적 특성을 기반으로 하여 이루어졌으나 이는 많은 시간이 소요되며 정확한 동정을 위해서 숙련된 전문가가 필요하다. 이에 비해 분자생물학적 동정은 소요 시간이 적으며 정확도가 높아 진균 동정에 도움을 주고 있다[21].
비피부사상균성 사상균인 A. sydowii는 Aspergillus 균종에서와 같이 KOH 검사상 특징적으로 두 갈래로 갈라진 분절 균사를 관찰할 수 있다 [14],[15],[22]. 이 균집락을 Lactophenol cotton blue 염색하여 현미경으로 관찰하면 유리질의 격막 균사를 보이고, 구상의 정낭 (vesicle)과 방사상 2단경자(biseriated phialides)의 끝에 분생포자가 전 구상을 덮고 있으며, Penicillium 균종을 닮은 분생포자가 관찰할 수 있다[17],[22]. 본 증례에서도 KOH 검사에서 두 갈래로 갈라진 분절 균사가 보였고, 반복적인 배양검사에서 동일한 배양 소견을 보였으며, Lactophenol cotton blue 염색에서 동일한 현미경 소견이 관찰되었다. 또한 균집락으로부터 DNA를 추출하여 진균핵내의 ITS 부위의 염기서열을 GenBank에 있는 A. sydowii strain XWSFJJ1 (Gen-Bank accession number FJ461692)의 ITS 부위의 염기서열과 비교한 결과 99% 일치하여 원인균주로 A. sydowii로 동정하였다.
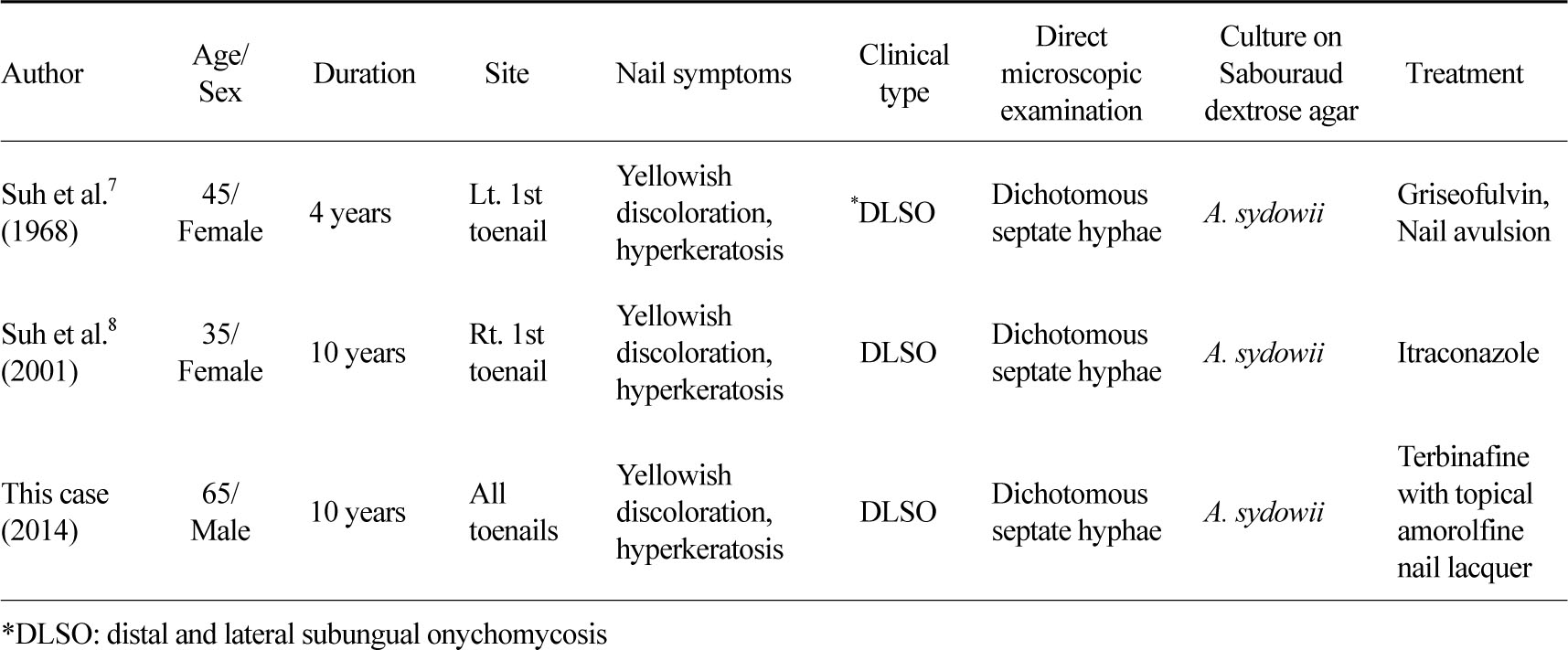
국내 피부과 문헌상 A. sydowii에 의한 손발톱 진균증은 1968년 Suh 등[7]의 보고와 2001년 Suh 등[8]의 보고 2예 뿐이다. 본 증례와 다른 두 보고 [7],[8]를 비교하여 보면 (Table 1) 3예 모두 30세 이상의 성인에서 발생하였고 유병기간은 각각 4~10 년으로 비교적 긴 유병기간을 가졌다. 3예 모두 발톱에서 발생하였으며 다른 두 보고[7],[8]는 여성에서 본 증례는 남성에서 발생하였다.
손발톱진균증의 임상형을 보면 1998년 Baran 등[23]은 손발톱진균증을 원위외측 손발톱하 손발톱진균증 (distal and lateral subungual onychomycosis, DLSO), 표재성 백색 손발톱진균증 (superficial white onychomycosis, SWO), 근위 손발톱하 손발톱진균증 (proximal subungual onychomycosis, PSO),손발톱내손발톱진균증 (endonyx onychomycosis, EO), 전이상성 손발톱진균증 (total dystrophic onychomycosis, TDO)으로 5가지 임상형으로 분류하였다. 이 중 손발톱진균증의 가장 흔한 유형은 DLSO이고, PSO는 비교적 드문 것으로 알려져 있다[1],[9]. Suh 등[7]과 Suh 등[8]의 2예 모두 임상형이 DLSO였고, 본 증례도 임상형이 DLSO였다. 그리고 3예 모두 KOH 검사에서 두 갈래로 갈라진 분절 균사가 관찰되었으며, 배양 시 청록색의 균집락이 관찰되었다.
비피부사상균성 사상균에 의한 손발톱진균증은 일반적으로 치료에 잘 반응하지 않는 것으로 알려져 있으나[24], Tosti 등[10] Aspergillus 균종에 의한 손발톱진균증 7예 중 치료받은 5예서 경구 및 국소 치료로 모두 완치를 관찰하여 다른 비피부사상균성 사상균과는 달리 Aspergillus 균종에 의한 손발톱진균증은 치료에 잘 반응한다고 하였고, Gianni와Romano[5]도 34예의Aspergillus 균종에 의한 손발톱진균증 환자 중 30예에서 매일 terbinafine 500 mg씩 1주 경구 복용하고 3주 쉬는 3개월 주기요법으로 완치되어 88%의 높은 치료율을 보였다. Suh 등[7]은 griseofulvin 1일 500 mg경구 투여와 외과적 발조술을 시행하였고, Suh 등[8]은 itraconazole 1일 100 mg 경구 투여로 완치를 관찰하였으며, 본 증례에서는 3개월간 terbinafine 1일 250 mg 경구 투여와 함께 최근 개발된 5% amorolfine nail lacquer 국소 도포를 병용함으로써 임상 및 진균학적 완치를 관찰할 수 있었다. 이에 저자들은 KOH 검사에서 두 갈래로 갈라진 균사가 관찰되고 항진균제에 비교적 잘 반응하는 비피부사상균성 손발톱진균증의 경우 A. sidowii를 원인균으로 의심해 보아야 할 것으로 생각한다.
References
1. Schieke SM, Garg A. Superficial fungal infection. In Goldsmith LA, Katz SI, Gilchrest BA, Paller AS, Leffell DJ, Wolff K, editors. Fitzpatrick's dermatology in general medicine. 8th ed. New York: McGraw-Hill, 2012:2278-2297
2. Gupta AK, Ryder JE, Baran R, Summerbell RC. Nondermatophyte onychomycosis. Dermatol Clin 2003; 21:257-268
3. Romano C, Gianni C, Difonzo EM. Retrospective study of onychomycosis in Italy: 1985-2000. Mycoses 2005;48:42-44
Google Scholar
4. Gupta M, Sharma NL, Kanga AK, Mahajan VK, Tegta GR. Onychomycosis: Clinico-mycologic study of 130 patients from Himachal Pradesh, India. Indian J Dermatol Venereol Leprol 2007;73:389-392
Google Scholar
5. Gianni C, Romano C. Clinical and histological aspects of toenail onychomyosis caused by Aspergillus spp.: 34 cases treated with weekly intermittent terbinafine. Dermatology 2004;209:104-110
Google Scholar
6. Hilmioqlu-Polat S, Metin DY, Inci R, Dereli T, Kilinc I, Tumbay E. Non-dermatophytic molds as agents of onychomycosis in Izmir, Turkey - a prospective study. Mycopathologia 2005;160:125-128
Google Scholar
7. Suh SB, Byun DK, Lee KY. A case of onychomycosis caused by Aspergillus sydowi. Korean J Dermatol 1968;6:39-43
8. Suh JC, Yeum JS, Na GY, Seo SK, Suh MK. A simple detection method of resistance to the treatment of onychomycosis: a case report of Aspergillus sydowii onychomycosis. Ann Dermatol 2001;13:62-65
Google Scholar
9. Lim SW, Suh MK, Ha GY. Clinical features and identification of etiologic agents in onychomycosis. Korean J Dermatol 2004;42:53-60
Google Scholar
10. Tosti A, Piraccini BM, Lorenzi S. Onychomycosis caused by nondermatophytic molds: clinical features and response to treatment 59 cases. J Am Acad Dermatol 2000;42:217-224
Google Scholar
11. Gianni C, Cerri A, Crosti C. Non-dermatophytic onychomycosis. An underestimated entity? A study of 51 cases. Mycoses 2000;43:29-33
Google Scholar
12. Summerbell RC, Kane J, Krajden S. Onychomycosis, tinea pedis and tinea manuum caused by nondermatophytic filamentous fungi. Mycoses 1989;32: 609-619
Google Scholar
13. Rippon JW. Medical mycology: The pathogenic fungi and the pathogenic actinomycetes. 3rd ed. Philadelphia: WB Saunders, 1988:618-650
14. Takahata Y, Hiruma M, Sugita T, Muto M. A case of onychomycosis due to Aspergillus sydowii diagnosed using DNA sequence analysis. 2008;51:170-173
Google Scholar
15. Tosti A, Piraccini BM. Proximal subungual onychomycosis due to Aspergillus niger: report of two cases. Br J Dermatol 1998;139:156-157
Google Scholar
16. Grover S. Clinicomycological evaluation of onychomycosis at banglore and Jorhat. Indian J Dermatol Venerol Leprol 2003;69:284-286
Google Scholar
17. De Hoog GS, Guarro J, Gene J, Figueras MJ. Atlas of clinical fungi. 2nd ed. Virgili, Centraalbureau voor Schimmelcultures, 2000:442-519
18. Hwang SM, Suh MK, Ha GY. Onychomycosis due to nondermatophytic molds. Ann Dermatol 2012;24: 175-180
Google Scholar
19. English MP. Nails and fungi. Br J Dermatol 1976;94: 697-701
20. Makimura K, Tamura Y, Mochizuki T, Hasegawa A, Tajiri Y, Hanazawa R, et al. Phylogenetic classification and species identification of dermatophyte strains based on DNA sequences of nuclear ribosomal internal transcribed spacer 1 regions. J Clin Microbiol 1999;37:920-924
Google Scholar
21. Ko JH, Hwang YJ, Kim JY, Lee YW, Choe YB, Ahn KJ. A case of concomitant tinea infection diagnosed with molecular biologic technique. Kor J Med Mycol 2010;15:150-155
Google Scholar
22. Kwon-Chung KJ, Bennett JE. Medical mycology. Philadelphia: Lea & Febiger, 1992:201-247
Google Scholar
23. Baran R, Hay RJ, Tosti A, Haneke E. A new classification of onychomycosis. Br J Dermatol 1998;139: 567-571
Google Scholar
24. Nolting S, Brautigam M, Weidinger G. Terbinafine in onychomycosis with involvement by nondermatophytic fungi. Br J Dermatol 1994;130(Suppl 43):16 -21
Google Scholar
