pISSN : 1226-4709 eISSN: 2465-8278
Open Access, Peer-reviewed
pISSN : 1226-4709 eISSN: 2465-8278
Open Access, Peer-reviewed
Soo Hyeon Bae,Min Young Lee,Jee-Bum Lee
http://dx.doi.org/10.17966/KJMM.2017.22.1.28 Epub 2017 March 30
Abstract
Tinea versicolor (TV) is a commonfungal skin disease caused by the Malasseziaspecies. This disease usually presents as hypopigmented- or hyperpigmented coalescing scalymacules, papules, patches or plaques on the trunk and upper arms.Herein, we report a rare clinical manifestation ofTV ina 29-year-oldman presenting with marked follicular, erythematous, and hyperkeratotic papuleson the trunk with erythematous scaly macules and patches on the upperextremities with intermittently spared skin. We initially suspected pityriasisrubra pilaris, however, skin biopsy results and mycological examinationrevealed TV. Polymerase chain reaction-based sequence analysis revealed Malassezia globosa. The patient wassuccessfully treated with oral itraconazole and topical terbinafine.
Keywords
Malassezia Malassezia globosa Tinea versicolor Pityriasis rubra pilaris
INTRODUCTION
Tinea versicolor (TV) is a common cutaneous fungal disease caused by the Malassezia species, mostly M. globosa. Although these organisms usu- ally inhabit the human skin as normal follicular flora in the yeast phase, they produce skin lesions when they grow to the hyphal phase[1]. Typically, TV presents in one of the three forms[1],[2]: papulo- squamous, folliculitis, or inverse. The papulosqua- mous form is the most common manifestation and is characterized by hypopigmented- or hyperpig- mented coalescing scaly macules, papules, patches or plaques on the trunk and upper arms. However, other unusual clinical presentations such as the atro- phying form[3] and mimicries of pityriasis rotunda[4], mycosis fungoides[5], and pityriasis rubra pilaris[2],[6] (PRP) have also been reported. In this case report, the authors describe a patient who showed hyper- keratotic follicular papules and scaly coalescent erythematous macules over the trunk and upper extremities with intermittently spared skin. Al- though we first suspected PRP, skin biopsy results confirmed a diagnosis of TV. To the best of our knowledge, this is the third reported case of TV mimicking PRP.
REPORT OF A CASE
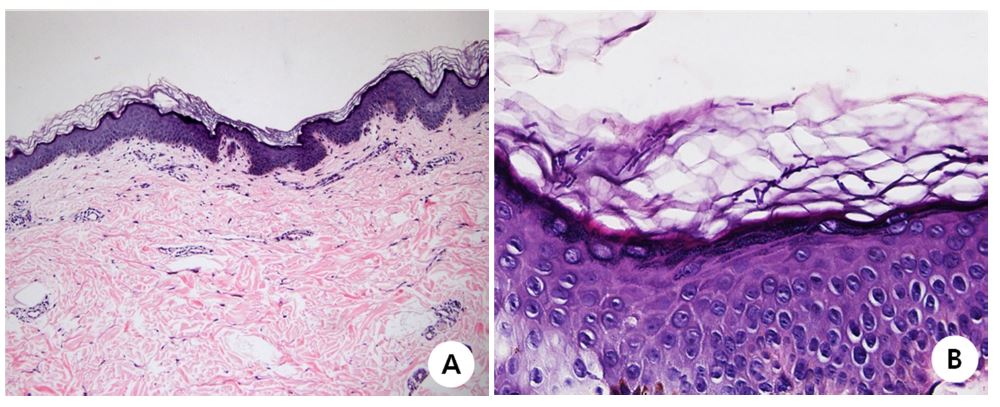
A 29-year-old man presented with a 10-year history of skin eruption. He denied any histories of medication and other cutaneous or systemic diseases, although topical steroid was applied on the skin lesion without improvement. On presen- tation, marked follicular, erythematous, hyper- keratotic papules were noted on the trunk (Fig. 1A, 1B). Erythematous scaly macules and patches with intermittent spared skin were also noted on upper extremities (Fig. 1C-F). He reported that the skin lesions progressed from his neck in a cephalo¬caudal distribution to involve his chest, abdomen, back, proximal arms, and proximal legs. Owing to the appearance, PRP was primarily raised as a pos- sible diagnosis and skin punch biopsy was perfor- med. Histologic examination revealed thick basket¬weave stratum corneum with septate hyphae and spores (Fig. 3A, 3B), consistent with TV. On the next visit, direct microscopic potassium hydroxide (KOH) examination revealed short, thick, fungal hyphae and large numbers of spores. Fungal culture of skin scrape showed growth of Malassezia species on a modified Leeming and Notman agar medium plate. PCR-based sequence analysis of the internal transcribed spacer region of the fungal rRNA gene was performed and showed 99% homology with M. globosa in the GenBank database (accession no. AY743630.1). The patient was treated with itraconazole 200 mg/d for 1 week and topical ter- binafine for 3 weeks. At the follow-up visit, KOH revealed no fungal organisms and skin lesions improved with remnant mild pigmentation (Fig. 2A-F).


DISCUSSION
TV is a common skin fungal infection caused by the Malassezia species. These organisms are usually present in 75~98% of healthy individuals as yeasts and are considered normal follicular flora[7]. They produce skin lesion, which is TV, when they grow to hyphaes. The prevalence of Malassezia is reportedly up to 50% in hot and humid regions compared to 1.1% in colder climates[1]. M. globosa, the major pathogen of TV, is a dimorphic, lipophilic organism that requires lipid for growth. This char- acteristic is apparent in that skin lesions are com- mon among adolescents whose sebaceous glands are more active and in oily areas of skin, such as the chest, abdomen, back, pubis, and intertriginous areas. Hyperhidrosis, oral contraceptives, systemic corticosteroid use, Cushing's disease, immunosup- pression, and malnourishment are also predisposing factors for TV[8].
Typically, a diagnosis of TV is based on a typical presentation of hypopigmented- or hyperpigmented, scaly, oval to round macules scattered over the upper trunk and arms, and can be confirmed through a microscopic KOH examination[1]. A combination of short, thick fungal hyphae and variably sized spores on KOH examination is commonly called "spaghetti and meatballs". M. globosa reveals whitish, dull, and friable colonies on a modified Leeming and Notman agar medium plate. Histo- logic examinations show clusters of oval budding yeast cells with short, septate, hyphae inhabiting the stratum corneum. TV should be differentiated from seborrheic dermatitis, pityriasis rosea, PRP, confluent and reticulated papillomatosis, pityriasis alba, Hansen's disease, syphilis, and vitiligo[8],[9]. Systemic regimens used for treating TV include itra- conazole, ketoconazole, and fluconazole[8]. Although topical terbinafine has been proven effective in TV treatment, it is ineffective via the oral route[8]. In this case, oral itraconazole and topical terbinafine are considered to have contributed to clinical improve- ment.
PRP is a rare, chronic papulosquamous disorder characterized by reddish-orange scaly patches, hyperkeratotic follicular papules, and palmoplantar keratoderma[1]. Skin lesions may progress to ery- throderma with sharply demarcated islands of nor- mal skin ("nappes claires"). The disease shows a bimodal age distribution with peak incidences in the first and fifth decades of life. It is known that there are no predilections for PRP regarding race and gender. PRP is classified into six types based on clinical characteristics such as age, pattern of lesion, prognosis, and medical or family history[1]. The classic adult type accounts for over 50% of all cases, shows a cephalo-caudal progression of skin lesions, and often resolves within three years. For the 10% of patients with atypical adult type, however, PRP shows a predilection for skin lesions on the legs, and runs a chronic course with skin lesions persisting for over 20 years. Histologically, erythematous lesions show acanthosis with broad and short rete ridges, and alternating orthokeratosis and parakeratosis in both vertical and horizontal directions[10]. Follicular papules show dilated in- fundibula filled with an orthokeratotic plug with perifollicular shoulders of parakeratosis at times. In our case, however, none of these histologic findings was apparent, indicating no concomitant PRP.
As far as we know, there have only been two cases of TV imitating PRP. Darling et al.[6] described a 54-year-old patient with a 20-year history of pruritic erythematous patches and keratotic follic- ular papules involving the trunk and upper arms, the patient was diagnosed with TV with only KOH findings. Berry and Khachemoune[2] confirmed TV with skin biopsy results in a 65-year-old patient presenting with similar skin lesions distributed along the trunk and proximal extremities. Although diagnoses were made, the exact pathogen could not be elucidated in both these cases. In our case, however, we confirmed TV with skin biopsy results and identified M. globosa as the causative organism. We believe that the long disease duration with improper use of corticosteroids may have led to this finding.
This case report represents an unusual presen- tation of TV mimicking PRP, which we consider unique and educational. Clinical presentations in- cluding scaly erythematous patches with islands of normal skin and hyperkeratotic follicular papules first led us to an initial diagnosis of PRP, however, skin biopsy confirmed TV. We suggest that der- matologists should always perform basic tests such as KOH when confronting patients with scaly erythematous patches before performing invasive examinations. Also, it is possible that TV with long duration and inappropriate treatment may demon- strate non-typical features mimicking many other diseases.
Conflict of interest
In relation to this article, I declare that there is no conflict of interest.
References
1. Kundu RV, Garg A. Yeast infections: Candidiasis, tinea (pityriasis) versicolor, and Malassezia (pityro- sporum) folliculitis. In: Goldsmith LA, Katz SI, Gilchrest BA, Paller AS, Leffell DJ, Wolff K, editors. Fitzpatrick's dermatology in general medicine, 8th ed. New York: McGraw-Hill, 2012:2307-2311
2. Berry M, Khachemoune A. Extensive tinea versicolor mimicking pityriasis rubra pilaris. J Drugs Dermatol 2009;8:490-491
Google Scholar
3. Lee DB, Chae WS, Jung HN, Choi YS, Suh HS. A case of pityriasis versicolor atrophicans. Korean J Med Mycol 2012;17:47-50
Google Scholar
4. Desruelles F, Gari-Toussaint M, Lacour J-P, Marty P, Le Fichoux Y, Ortonne J-P. Tinea versicolor mimic- king pityriasis rotunda. Int J Dermatol 1999;38:948 -949
Google Scholar
5. Werner B, Brown S, Ackerman AB. "Hypopigmented mycosis fungoides" is not always mycosis fungoides! Am J Dermatopathol 2005;27:56-67
Crossref
Google Scholar
6. Darling MJ, Lambiase MC, Young RJ. Tinea versi- color mimicking pityriasis rubra pilaris. Cutis 2005; 75:265-267
Google Scholar
7. Ljubojevi ĆS, Skerlev M, Lipozencčić J, Basta-Juzbašić A. The role of Malassezia furfur in derma- tology. Clin Dermatol 2002;20:179-182
Crossref
8. James WD, Berger TG, Elston DM. Diseases re- sulting from fungi and yeasts. In: James WD, Berger TG, Elston DM, editors. Andrews' diseases of the skin: clinical dermatology, 11th ed. Elsevier Health Sciences, 2015:287-321
9. Bruynzeel-Koomen CA, de Wit RFE. Confluent and reticulated papillomatosis successfully treated with the aromatic etretinate. Arch Dermatol 1984;120: 1236-1237
Crossref
Google Scholar
10. Braun-Falco O, Ryckmanns F, Schmoeckel C, Landthaler M. Pityriasis rubra pilaris: a clinico-pathological and therapeutic study with special refer- ence to histochemistry, autoradiography, and electron microscopy. Arch Dermatol Res 1983;275:287-295
Crossref
Google Scholar
