pISSN : 1226-4709 eISSN: 2465-8278
Open Access, Peer-reviewed
pISSN : 1226-4709 eISSN: 2465-8278
Open Access, Peer-reviewed

Joon Woo Jung,Eun Hye Hong,Eun Joo Park,Kwang Joong Kim,Kwang Ho Kim
10.17966/JMI.2021.26.1.1 Epub 2021 March 29
Abstract
Background: Acanthosis nigricans (AN) is a skin condition that presents clinically with hyperpigmented, hyperkeratotic, and velvety skin changes, especially in the intertriginous areas. The intertriginous areas are also susceptible to superficial cutaneous fungal infections. The potential relationship between AN and cutaneous fungal infection has not been investigated.
Objective: The aim of this study was to determine the relationship, if any, between AN and fungal infection, both clinically and pathologically.
Methods: A retrospective review was performed using electronic medical records and histology of biopsy slides obtained from 29 patients who were diagnosed with AN by two dermatopathologists. Comparison was made between the clinical and pathological findings of AN with fungal infection (ANFI+) and AN without fungal infection (ANFI-).
Results: Among the 29 patients with AN, fungal spores were detected on the biopsy slides of 18 patients (62.1%) and appeared in the epidermal furrow more often than in the epidermal ridge. No significant clinical difference was found between the ANFI+ and ANFI- groups; however, in the ANFI+ group, lesions were more prevalent in the neck area (p = 0.048). In addition, the ANFI+ biopsy slides revealed more papillomatosis than ANFI- biopsy slides (p = 0.006).
Conclusion: Fungal infection tends to appear in combination with AN when more severe papillomatosis is also present.
Keywords
Acanthosis nigricans Fungal infection Papillomatosis
Acanthosis nigricans (AN) is a skin condition that presents clinically with hyperpigmentation, hyperkeratosis, and velvety skin changes that typically appear on the axilla, neck, and inguinal areas and other flexor parts of the body. Several causes of this condition have been identified, such as insulin resistance, type 2 diabetes mellitus, metabolic syndrome, and polycystic ovary syndrome. Occasionally, AN can be an indicator of internal malignancy. Hyperkeratosis and papillomatosis are histopathological findings of AN. Hyperpigmented black or brown skin is typically due to hyperkeratosis rather than an increase in melanin content in patients with AN. Diagnosis of AN is based on both clinical and histopathological findings.
Cutaneous fungal infection is a common superficial skin dis- ease caused by dermatophytes, yeasts, and non-dermatophyte molds. Cutaneous fungal infections appear in various clinical findings and tend to be present in intertriginous areas that are hyperhydrated and subjected to higher amounts of friction than other parts of the body. Damage to the epidermal tissue and the skin barrier due to hyperhydration and friction can lead to secondary infections by microorganisms that may appear more frequently in these areas.
AN is more likely to appear in obese persons than in normal weight persons. Given this potential for secondary infections to occur in intertriginous areas, we believe that AN skin lesions are susceptible to fungal infections. At the time of this study, no specific research had investigated the relationship be- tween AN and cutaneous fungal infection. Therefore, our study aimed to examine the potential relationship between AN and cutaneous fungal infection, both clinically and histopathologically.
No AN-specific treatment exists, and current treatment practices are challenging and time-consuming. A previous study reported that patients with AN are more likely to report low self-esteem than non-AN patients. Because untreated AN can cause social and emotional stress in patients, the treatment of AN should be considered important.
Currently, several treatment strategies for AN are being attempted, but no studies have been conducted on the use of antifungal agents. The purpose of this study was to clinically and pathologically compare patients with AN and fungal infection (ANFI+) with those with AN without fungal infection (ANFI-) and to suggest which patients may benefit from the use of antifungal agents.
1. Patients
This retrospective study reviewed clinical and histopathological findings of 52 patients who visited the department of dermatology from January 2010 to June 2020 and were suspected of having AN. Among these patients, 29 were definitively diagnosed with AN based on clinical and histopathological findings and were included in the study. In addition, clinical images captured before skin biopsy were used for final diagnosis. Patients with AN had not received any topical or systemic treatment for their skin lesions in the past. Skin punch biopsies were performed at the most prominent skin lesion.
2. Clinical characteristics
A retrospective electronic medical record (EMR) review was conducted for the 29 patients with AN. Information on sex, age, disease duration, location, obesity, and glucose level was retrieved from the EMR, and clinical images were reviewed. The disease duration was classified as one of three groups: <1 month, 1 month to 1 year, and >1 year. The location of the skin lesion was classified as one of four areas: neck, trunk, axilla, and anterior cubital fossa. Finally, blood glucose level was classified as one of two groups: <100 mg/dL and ≥100 mg/ dL (normal range: 70~99 mg/dL).
3. Histopathological analysis
Two dermatopathologists independently analyzed hemato- xylin-eosin-stained biopsy slides of each patient. They reviewed the biopsy slides until consensus was achieved. Hyperkeratosis, papillomatosis, basal layer hyperpigmentation, dermal melanin component, and fungal infection were evaluated. The severity of hyperkeratosis and papillomatosis was classified into three levels: none, mild, and marked. When fungal spores were observed, the locations were analyzed by subdividing them into epidermal furrows, epidermal ridges, and hair follicles.
4. Statistical analyses
Relationships among fungal infection and sex, location, and glucose levels were analyzed using Fisher's exact test. Linear-by-linear association method was used to analyze the relationship between fungal infection and lesion duration and histopathological findings (hyperkeratosis and papillomatosis). The Mann-Whitney test was used to determine the relation- ship between fungal infection and age and glucose levels in patients with AN. Statistical Package for Social Science (SPSS) software version 26.0 (SPSS Inc., Chicago, IL, USA) was used for data analysis, and statistical significance was defined by a p-value < 0.05.
1. Clinical characteristics of patients with AN
A total of 29 patients (17 men and 12 women) diagnosed with AN based on clinical and histological findings were included in the study (Table 1). The mean age was 19 years (range: 10~58 years). The most common disease duration was >1 year (48.3%), followed by 1 month to 1 year (24.1%) and <1 month (6.9%). The neck (62.1%) was the most common location of the skin lesions, followed by the axilla (24.1%), trunk (10.3%), and anterior cubital fossa (3.4%). Of the 29 patients, 22 (75.9%) were obese, 2 (6.9%) were of normal weight, and the weights of 5 (17.2%) were unknown. Of the 22 patients whose blood glucose levels were evaluated, 10 had glucose levels <100 mg/dL and 12 had glucose levels ≥100 mg/dL. The mean glucose level was approximately 102.32 mg/dL (range: 80~159 mg/dL).
|
Characteristics |
Number
(%) |
|
Sex |
|
|
Male |
17
(58.6%) |
|
Female |
12
(41.4%) |
|
Age |
19±9.6 |
|
Duration |
|
|
<1
month |
2
(6.9%) |
|
1
month~1 year |
7 (24.1%) |
|
>1
year |
14
(48.3%) |
|
UK |
6 (20.7%) |
|
Location |
|
|
Neck |
18
(62.1%) |
|
Trunk |
3 (10.3%) |
|
Axilla |
7 (24.1%) |
|
Antecubital
fossa |
1 (3.4%) |
|
Obesity |
|
|
Yes |
22
(75.9%) |
|
No |
2 (6.9%) |
|
UK |
5 (17.2%) |
|
Blood glucose level |
|
|
<100
mg/dL |
10 |
|
≥100 mg/dL |
12 |
|
Mean ± SD (mg/dL) |
102.32±18.79 mg/dL |
|
UK |
7 |
|
Values are presented as number (%) or mean ± standard deviation UK = Unknown |
|
2. Histological features of AN patients
Five histopathological findings (hyperkeratosis, papillomatosis, basal layer hyperpigmentation, dermal melanin component, and fungal infection) were evaluated in 29 patients with AN (Table 2). Mild hyperkeratosis was observed in 17 patients (58.6%) and marked hyperkeratosis in 11 patients (37.9%). Thirteen (44.8%) had mild papillomatosis, and 14 (48.3%) had marked papillomatosis. In addition, basal layer hyperpigmentation was observed in 25 (86.2%); dermal melanin component, in 24 (82.8%); and fungal infection, in 18 patients (62.1%).
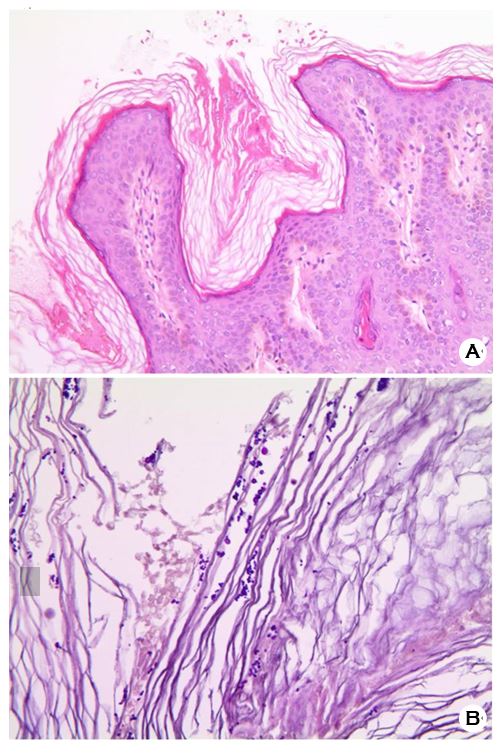
A pathological review was conducted to determine the location of fungal spores in patients with ANFI+. In 15 of the 18 patients, spores were observed in the epidermal furrow. Spores were also observed in the epidermal ridge in two patients, and hair follicles were observed in one patient. The presence of fungal spores was confirmed through periodic acid-Schiff staining (Fig. 1).
|
Pathological findings |
Number (%) |
|
Hyperkeratosis |
|
|
None |
1 (3.4%) |
|
Mild |
17 (58.6%) |
|
Marked |
11 (37.9%) |
|
Papillomatosis |
|
|
None |
2 (6.9%) |
|
Mild |
13 (44.8%) |
|
Marked |
14 (48.3%) |
|
Basal layer hyperpigmentation |
25 (86.2%) |
|
Dermal melanin component |
24 (82.8%) |
|
Fungal infection |
|
|
None |
11 (37.9%) |
|
Furrow |
15 (51.7%) |
|
Ridge |
2 (6.9%) |
|
Hair follicle |
1 (3.4%) |
|
Values are presented as a number (%) |
|
3. Comparison between ANFI+ and ANFI-
|
Characteristics |
AN without fungal (n=11) |
AN with (n=18) |
p-value |
|
Sex |
|
|
1.000 |
|
Male |
6 |
11 |
|
|
Female |
5 |
7 |
|
|
Age |
20±13.99 |
19±5.91 |
0.521 |
|
Duration |
|
|
0.440 |
|
<1 month |
- |
2 |
|
|
1 month ~ |
5 |
2 |
|
|
>1 year |
3 |
11 |
|
|
UK |
3 |
3 |
|
|
Location |
|
|
|
|
Neck |
4 |
14 |
0.048* |
|
Trunk |
2 |
1 |
0.539 |
|
Axilla |
4 |
3 |
0.375 |
|
Antecubital |
1 |
- |
0.379 |
|
Obesity |
|
|
0.101 |
|
Yes |
6 |
16 |
|
|
No |
2 |
- |
|
|
UK |
3 |
2 |
|
|
Blood glucose level |
|
|
1.000 |
|
<100 mg/dL |
3 |
7 |
|
|
≥100 mg/dL |
4 |
8 |
|
|
mean ± SD |
100.57± |
103.13± |
0.731 |
|
UK |
4 |
3 |
|
|
Values are presented as a number or mean ± standard de- viation (SD) UK = Unknown *: p-value < 0.05 |
|||
When the clinical characteristics of ANFI- (11 patients) and ANFI+ (18 patients) were compared, there were no statistically significant differences in sex and age categories (Table 3). The rate of ANFI+ of >1 year duration was higher than that of ANFI- (73.3% > 37.5%); however, there was no statistically significant difference between the degree of duration and the risk of fungal infection (p = 0.440). Regarding the location, the lesion was more likely to appear on the neck in ANFI+ patients (odds ratio: 6.125, p = 0.048). There was no statistical correlation between fungal infection and obesity in the patients (p = 0.101). The mean glucose level of ANFI+ was higher than that of ANFI-; however, it was not statistically significant (103.13 mg/dL > 100.57 mg/dL, p = 0.731).
The risk of fungal infection was also analyzed according to the severity of hyperkeratosis and papillomatosis (none/ mild/marked) (Table 4). No significant relationship was found between the degree of hyperkeratosis and the risk of fungal infection (p = 0.214). However, as the degree of papillomatosis increased, the association with fungal infection tended to increase (p = 0.006).
|
Histopathologic |
Fungal infection |
p-value |
|
|
No |
Yes |
||
|
Hyperkeratosis |
|
|
0.214 |
|
None |
1 |
0 |
|
|
Mild |
7 |
10 |
|
|
Moderate |
3 |
8 |
|
|
Papillomatosis |
|
|
0.006* |
|
None |
2 |
0 |
|
|
Mild |
7 |
6 |
|
|
Moderate |
2 |
12 |
|
|
Values
are presented as number *: p-value < 0.05 |
|||
AN is a skin condition that presents clinically with velvety, papillomatous, hyperpigmented patches, especially in the inter- triginous areas. AN is known to be associated with obesity, insulin resistance, type 2 diabetes mellitus, and malignancy. The clinical features of AN are attributed to the stimulation of growth factors of keratinocytes and dermal fibroblasts.
To date, no specific study has been conducted on the association between AN and fungal infection. However, in a report that described a case of hyperkeratotic head and neck Malassezia dermatosis, fungal spores were observed in the biopsy of a lesion that resembled AN clinically and histopathologically. This study is significant in that it is the first study that examined the relationship between AN and fungal infection.
Burke et al. reported that the severity of AN and fasting insulin, BMI, and waist circumference indicated positive cor- relations in patients with or without diabetes mellitus. In non-diabetic patients, it was reported that the severity of AN increases as fasting glucose increases. Mirimirani et al. reported that fungal infections were more frequently observed in obese patients than in patients with normal BMI. Obese patients are vulnerable to infection due to sweat, skin surface pH, and friction in the skin folds, which can cause changes in the skin barrier. In addition, the tendency of skin fungal infection increases with an increase in the glucose level. The expectation for the present study was that if the glucose level was elevated or accompanied by obesity in patients with AN, the risk of fungal infection might increase. However, there were no significant results. This result is likely due to insufficient sample size and missing data. Further studies on the associations between fungal infection, fasting glucose level, insulin level, and obesity in patients with AN are required in the future.
In this study, the severity of papillomatosis tended to be associated with fungal infection, suggesting that this is an important indicator of fungal infection. Skin fold areas are more sensitive to fungal infection than the other sites because of a high risk of underventilation, moisturization, and friction. These conditions could be a reason for skin infections, fungal or otherwise. In the investigation of the fungal spores on the biopsy slides, the spores were observed in the epidermal furrow in 83.3% of ANFI+ patients (15 out of 18 cases). This may be explained by the relationship of papillomatosis and the epidermal furrow: With the increase in severity of papillomatosis, the epidermal furrow becomes deeper, and, as a result, becomes more susceptible to fungal infection as in the skin folds.
In this study, although genome sequencing or fungus culture could not be used to identify the fungal species, Malassezia yeast was considered to be the most likely etiology in the fungal spores observed. More specifically, the etiological agents in this study were most likely M. restricta and M. globosa, which Lee et al. reported to be the most frequently observed Malassezia species in humans. Malassezia are a part of the normal flora in healthy humans; however, in patients with AN, opportunistic infection caused by Malassezia may occur because of skin barrier damage. Some of the patients with AN did not present with fungal spores on biopsy slides. In addition, when AN occurred in the neck, it was more likely to be accompanied by fungal infection. For this reason, the Malassezia yeast observed in this study could be thought of as an opportunistic infection rather than normal flora.
Treatment for the underlying disease is required for patients with AN. For example, obesity, hyperinsulinemia, and other factors should be corrected as part of treatment. In addition, treatments that address the underlying cutaneous pathology, such as hyperkeratosis using topical retinoid, topical vitamin D analog, and chemical peeling, have recently emerged. In sum, treatment alone is not sufficient; correcting the causes and addressing the cutaneous pathologies are also crucial. According to An et al., a patient in whom clinically and pathologically typical AN with fungal spores were found was successfully treated with an antifungal agent (terbinafine [250 mg] and topical flutrimazole). Although there have been no studies on the use of antifungal agents in patients with AN so far, this use is expected to be effective in AN patients with fungal infections. In the present study, the trend was as follows: The more severe the histopathological papillomatosis, the higher the tendency of fungal infection. Based on this, we believe that the use of an antifungal agent would be helpful in treating patients with AN and severe papillomatosis. Further studies on antifungal treatment of AN should be conducted.
The limitations of this study were the retrospective design and small sample size. The EMR for some patients was not completely recorded, leaving some clinical data missing. Therefore, further studies on the difference between AN patients with and without fungal infection should be conducted. In addition, accurate verification of the type of fungal infection in the patients was not possible. Future studies on the specific fungal etiological agents associated with AN are required.
This study compared the histopathological and clinical differences among patients with AN according to the presence or absence of fungal infection. Among patients with AN, higher severity of papillomatosis was associated with the presence of fungal infection. Further studies on AN and fungal infections are required, and studies of antifungal treatment and its therapeutic effects on patients with AN and concomitant fungal infections are also required.
References
1. Schwartz RA. Acanthosis nigricans. J Am Acad Dermatol 1994;31:1-19
Google Scholar
2. Stuart CA, Gilkison CR, Smith MM, Bosma AM, Keenan BS, Nagamani M. Acanthosis nigricans as a risk factor for non-insulin dependent diabetes mellitus. Clin Pediatr 1998;37:73-79
Google Scholar
3. Matsuoka LY, Wortsman J, Gavin JR, Goldman J. Spectrum of endocrine abnormalities associated with acanthosis nigricans. Am J Med 1987;83:719-725
Google Scholar
4. Cruz PD Jr, Hud JA Jr. Excess insulin binding to insulin-like growth factor receptors: proposed mechanism for acanthosis nigricans. J Invest Dermatol 1992;98:82S-85S
Google Scholar
5. Rendon MI, Cruz PD Jr, Sontheimer RD, Bergstresser PR. Acanthosis nigricans: a cutaneous marker of tissue re- sistance to insulin. J Am Acad Dermatol 1989;21:461-469
Google Scholar
6. Curth HO. Cancer associated with acanthosis nigricans: review of literature and report of a case of acanthosis nigricans with cancer of the breast. Arch Surg 1943;47: 517-552
Google Scholar
7. Higgins SP, Freemark M, Prose NS. Acanthosis nigricans: a practical approach to evaluation and management. Dermatol Online J 2008;14:2
Google Scholar
8. Sherertz EF. Improved acanthosis nigricans with lipodys- trophic diabetes during dietary fish oil supplementation. Arch Dermatol 1988;124:1094-1096
Google Scholar
9. Kapoor S. Diagnosis and treatment of acanthosis nigricans. Skinmed 2010;8:161-164
Google Scholar
10. Foster KW, Ghannoum MA, Elewski BE. Epidemiologic surveillance of cutaneous fungal infection in the United States from 1999 to 2002. J Am Acad Dermatol 2004; 50:748-752
Google Scholar
11. Kalra MG, Higgins KE, Kinney BS. Intertrigo and secondary skin infections. Am Fam Physician 2014;89:569-573
Google Scholar
12. Del Rosso JQ, Draelos ZD, Jorizzo JL, Joseph WS, Ribotsky BM, Rich P. Modern methods to treat superficial fungal disease. Cutis 2007;79(2 suppl):6-29
Google Scholar
13. Pirgon Ö, Sandal G, Gökçen C, Bilgin H, Dündar B. Social anxiety, depression and self-esteem in obese adolescent girls with acanthosis nigricans. J Clin Res Pediatr Endocrinol 2015;7:63-68
Google Scholar
14. Sinha S, Schwartz RA. Juvenile acanthosis nigricans. J Am Acad Dermatol 2007;57:502-508
Google Scholar
15. An MK, Yoon JH, Cho EB, Park EJ, Kim KH. A suspected case of hyperkeratotic head and neck Malassezia der- matosis presenting with acanthosis nigricans. J Mycol Infect 2018;23:111-114
Google Scholar
16. Burke JP, Hale DE, Hazuda HP, Stern MP. A quantitative scale of acanthosis nigricans. Diabetes Care 1999;22: 1655-1659
Google Scholar
17. Mirmirani P, Carpenter DM. Skin disorders associated with obesity in children and adolescents: a population-based study. Pediatr Dermatol 2014;31:183-190
18. Yosipovitch G, DeVore A, Dawn A. Obesity and the skin: skin physiology and skin manifestations of obesity. J Am Acad Dermatol 2007;56:901-916;quiz 917-920
Google Scholar
19. Yosipovitch G, Tur E, Cohen O, Rusecki Y. Skin surface pH in intertriginous areas in NIDDM patients. Possible correlation to candidal intertrigo. Diabetes Care 1993; 16:560-563
Google Scholar
20. Guida B, Nino M, Perrino NR, Laccetti R, Trio R, Labella S, et al. The impact of obesity on skin disease and epidermal permeability barrier status. J Eur Acad Dermatol Venereol 2010;24:191-195
Google Scholar
21. Oumeish OY. Skin disorders in patients with diabetes. Clin Dermatol 2008;26:235-242
22. Metin A, Dilek N, Demirseven DD. Fungal infections of the folds (intertriginous areas). Clin Dermatol 2015;33:437-447
Google Scholar
23. Lee YW, Yim SM, Lim SH, Choe YB, Ahn KJ. Quantitative investigation on the distribution of Malassezia species on healthy human skin in Korea. Mycoses 2006;49:405-410
Google Scholar
24. Ahn KJ. Taxonomy of the genus Malassezia. Korean J Med Mycol 1998;3:81-88
25. Puri N. A study of pathogenesis of acanthosis nigricans and its clinical implications. Indian J Dermatol 2011;56: 678-683
Google Scholar
26. Patel NU, Roach C, Alinia H, Huang WW, Feldman SR. Current treatment options for acanthosis nigricans. Clin Cosmet Investig Dermatol 2018;11:407-413
Congratulatory MessageClick here!
