pISSN : 1226-4709 eISSN: 2465-8278
Open Access, Peer-reviewed
pISSN : 1226-4709 eISSN: 2465-8278
Open Access, Peer-reviewed

Ye Ji Jang,Ji Ha Yoon,Eun Joo Park,Kwang Joong Kim,Kwang Ho Kim
10.17966/JMI.2019.24.4.96 Epub 2020 January 06
Abstract
Patients presenting with green nail syndrome often show coinfection with fungus. A delay in the accurate diagnosis of coinfection may warrant longer treatment duration. Four patients with green nail syndrome coinfected with fungus were reviewed retrospectively. Fungal culture, cultivating Candida parapsilosis and Candida albicans, was performed in two patients' samples. The mean time of the initiation of treatment for onychomycosis after the first visit was 5.75 weeks. If green nail syndrome is suspected, screening for fungal coinfections and precise management are necessary.
Keywords
Coinfection Green nail syndrome Onychomycosis Pseudomonas aeruginosa
The most common bacterial nail infection is green nail syndrome (GNS) caused by Pseudomonas aeruginosa. Recent studies suggest that fungal infections may promote colonization or growth of P. aeruginosa in the nail1. In addition, such coinfection of onychomycosis with P. aeruginosa can prevent the growth of fungi in fungal culture, owing to an excessive growth of bacteria in the culture2. We report four cases of onychomycosis coinfected with P. aeruginosa.
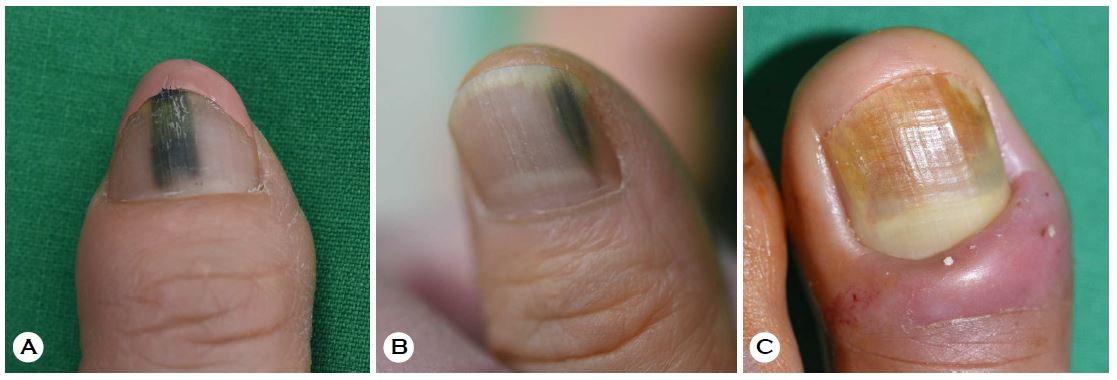
Patient 1, a 54-year-old woman, showed greenish nail color change on the right thumb fingernail approximately 2 months prior to the first visit (Figure 1A). Candida parapsilosis was isolated from the fungal culture with positive potassium hydroxide (KOH) test. P. aeruginosa was identified with sensitivity to ciprofloxacin in the bacterial culture. The patient was treated with ciprofloxacin 250 mg twice daily for 4 weeks following 3 cycles of itraconazole pulse therapy. Itraconazole pulse therapy was initiated 4 weeks after the first visit of the patient.
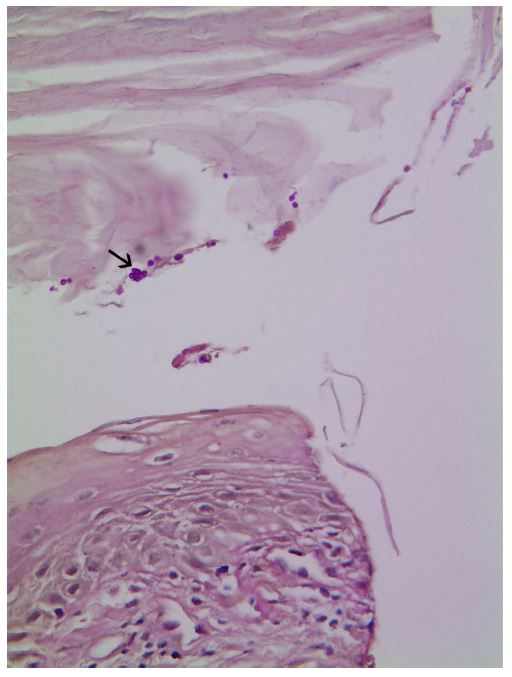
Patient 2, a 60-year-old woman, presented with bluish green melanonychia on her left thumb fingernail (Figure 1B). Periodic acid-Schiff (PAS) staining of 3 mm punch biopsy was positive (Figure 2). P. aeruginosa was identified with sensitivity to third generation cephalosporin in the bacterial culture. The patient was treated with cefpodoxime proxetil 100 mg twice daily for 2 weeks and terbinafine 250 mg daily 16 weeks. Terbinafine was initiated 1 week after the first visit. After 2 weeks of treatment, the green color change disappeared from the infected nail, and a new nail growth was observed.
Patient 3, a 45-year-old woman, presented with greenish nail color change on the left great toe nail (Figure 1C). KOH test, that was performed before the nail extraction, showed a positive result. P. aeruginosa was identified with sensitivity to ciprofloxacin in the bacterial culture. After nail extraction, the patient was treated with ciprofloxacin 250 mg twice daily for 3 weeks. After the 3-month observation period, the patient showed inadequate nail growth with suspected residual fungal infection in the affected nail. The patient was treated with topical flutrimazole and terbinafine 250 mg daily.
Patient 4, a 51-year-old woman, underwent nail extraction of the right thumb fingernail that was infected with Pseudomonas. C. albicans was isolated in the fungal culture with a positive KOH test. P. aeruginosa was identified with sensitivity to ciprofloxacin in the bacterial culture. After nail extraction, the patient was administered ciprofloxacin 250 mg twice daily for 3 weeks, and 2 cycles of itraconazole pulse therapy with topical eficonazole. Itraconazole was initiated 3 weeks after the first visit of the patient. Table 1 summarizes the patients' demographics and clinical characteristics.
|
Sex/Age |
Infected
nail |
Biopsy |
KOH test |
Fungus culture |
|
F/54 |
Right thumb |
Old hemorrhage and |
Positive |
Candida
parapsilosis |
|
F/60 |
Left thumb |
Some fungal spores in PAS stain: positive |
Not performed |
Not performed |
|
F/45 |
Left great
toe |
Hyperkeratotic nail with |
Positive |
Not performed |
|
F/51 |
Right thumb |
Not performed |
Positive |
Candida
albicans |
GNS is characterized by the colonization of P. aeruginosa on the dorsal or ventral nail plate. Chronic paronychia, onycholysis, onychotillomania, microtrauma to the nail fold, chronic exposure to water, soaps or detergents are known predisposing factors for the development of GNS. In green nails, a bacterial biofilm can be seen as a basophilic layer on the undersurface of the nail. In very faintly stained sections, a greenish tinge may be detectable3.
P. aeruginosa produces antifungal activity by the production of pyocyanin and 1-hydroxyphenazine2. P. aeruginosa kills mold by forming a dense biofilm on C. albicans filaments4. P. aeruginosa also inhibits the growths of Trichophyton rubrum and Trichophyton mentagrophytes5.
Dermatophytosis may be coupled with an infection of P. aeruginosa. Onychomycotic nails may provide a more favorable environment as long-term carriers of P. aeruginosa than normal nails1. Onychomycotic nails include the nail space under the lateral folds, that are ideal for the growth of P. aeruginosa. Another study reported that KOH-positive nail specimens are more likely to produce P. aeruginosa statistically significant than KOH-negative specimens6. This suggests that fungal infections may potentiate the colonization and growth of P. aeruginosa in nail specimen.
Yang et al.7 suggested the mechanism of coinfection in onychomycotic nail with P. aeruginosa. Fungal exudates containing sugars, amino acids, polyols, and organic acids aid in the positive chemotaxis of P. aeruginosa to the onychomycotic nail. Subsequently, P. aeruginosa produces an antifungal peptide toxin that inhibits fungal growth in infected nails. Thus, fungal species in the nails enhance the growth and colonization of P. aeruginosa, but are later replaced by P. aeruginosa.
For the treatment of green nail syndrome, the entire nail may be removed, or the detached nail plate may be cut off. Applying a few drops of chlorhexidine solution or diluted bleach twice or thrice daily topically removes pigmentation within a few weeks. Treatment with topical antibiotics such as nadifloxacin, gentamicin, and ciprofloxacin have also been reported as valuable therapeutic options. Topical antibiotics (polymyxin B or bacitracin) applied twice to quad times daily for one to four months have been reported to be effective in immunocompetent patients. Systemic antibiotics are not generally needed but some case reports have demonstrated successful treatment with twice or thrice weekly of oral ciprofloxacin.
All the four cases in our study support the hypothesis that onychomycosis may predispose P. aeruginosa infection. Although further investigations are needed to explain the interactions between these organisms, the cases in our study emphasize the importance of recognizing this coinfection relationship for proper treatment. Furthermore, when GNS is suspected, confirmation of the presence of fungal infection by KOH, fungal culture, or PAS stain may help determine the appropriate treatment direction.
The patient provided written informed consent for the publication and the use of his or her images.
References
1. Eckart H. Histopathology of the nail. Onychopathology. 1st ed. Florida: CRC Press, 2017:145-146
Google Scholar
2. Kerr JR, Taylor GW, Rutman A, Hoiby N, Cole PJ, Wilson R. Pseudomonas aeruginosa pyocyanin and 1-hydroxyphenazine inhibit fungal growth. J Clin Pathol 1999;52: 385-387
Google Scholar
3. Hogan DA, Kolter R. Pseudomonas-Candida interactions: an ecological role for virulence factors. Science 2002;296: 2229-2232
Google Scholar
4. Treat J, James WD, Nachamkin I, Seykora JT. Growth inhibition of Trichophyton species by Pseudomonas aeruginosa. Arch Dermatol 2007;143:61-64
Google Scholar
5. Mermel LA, McKay M, Dempsey J, Parenteau S. Pseudomonas surgical-site infections linked to a healthcare worker with onychomycosis. Infect Control Hosp Epidemiol 2003;24:749-752
Google Scholar
6. Foster KW, Thomas L, Warner J, Desmond R, Elewski BE. A bipartite-interaction between Pseudomonas aeruginosa and fungi in onychomycosis. Arch Dermatol 2005;141: 1467-1468
Google Scholar
7. Yang YS, Ahn JJ, Shin MK, Lee MH. Fusarium solani onychomycosis of the thumbnail coinfected with Pseudomonas aeruginosa: report of two cases. Mycoses 2011; 54:168-171
Google Scholar
Congratulatory MessageClick here!
