pISSN : 1226-4709 eISSN: 2465-8278
Open Access, Peer-reviewed
pISSN : 1226-4709 eISSN: 2465-8278
Open Access, Peer-reviewed

YongWoo Choi,Joonsoo Park
10.17966/JMI.2019.24.1.9 Epub 2019 March 28
Abstract
Background: Exposure and sensitization to fungal allergens can evoke the development and worsen allergic diseases. Many patients with allergies show multiple positive reactions to different allergens.
Objective: The purpose of this study was to analyze the relationship between fungal allergens that are mostly found in South Korea and other positive reactions to the allergens of the multiple allergosorbent simultaneous test chemiluminescent assay (MAST-CLA).
Methods: We enrolled 1,040 (588 men, 452 women) patients who showed positive reactions to three fungi, namely, Alternaria alternata, Aspergillus fumigatus, and Cladosporium herbarum, using MAST-CLA at Daegu Catholic University Medical Center from January 2010 to July 2017. The epidemiology and relationship between positive reactions to multiple fungal allergens and positive reactions to the allergens of the MAST-CLA were investigated.
Results: A. alternata was the most common fungal species, followed by C. herbarum and A. fumigatus (78.8% vs. 52.1% vs. 20.1%). Patients who showed positive reactions to all fungal allergens had 4.97 other antigens on average. Statistically significant results were obtained when comparing positive reactions to all fungal allergens to other allergens (Spearman correlation coefficient = 0.129, p < 0.05).
Conclusion: Patients should be educated on allergic diseases caused by other antigens if they are sensitized to fungal antigens.
Keywords
Allergen Alternaria alternata Aspergillus fumigatus Chemiluminescent assay Fungi
For the past 20~30 years, there has been a steady and rapid increase in the number of patients with allergic diseases worldwide1. Identification of potential allergens is important not only for diagnosis but also for the treatment of patients, which can help avoid causative allergens and initiate early immunotherapy. Multiple allergosorbent simultaneous test chemiluminescent assay (MAST-CLA) can detect specific IgE antibodies against various allergens. It was introduced in Korea in the early 1990s and is most commonly used up to date2. Patients with allergies often have allergies to ≥2 antigens2. Patients are often confirmed to have positive reactions to multiple allergens through MAST-CLA2. Some studies have investigated the relationship between antigens in the MAST-CLA panel other than fungal antigens. However, only a few studies have focused on the link between fungal antigens and other antigens2. Several fungal species are known to cause severe respiratory and cutaneous allergic diseases3, but only a few epidemiological studies have shown the prevalence of allergic reactivity to fungi using skin tests or IgE detection4-7. Therefore, this study aimed to analyze the epidemiology and the relationship between fungal allergens and other allergens.
1. Data
This study was a retrospective analysis of the electronic and written charts of patients with a positive reaction to, at least, one of the following three different fungi confirmed by MAST-CLA, which was performed at the dermatology department of Daegu Catholic University Medical Center (DCUMC) from January 2010 to July 2017. These fungal species were Alternaria alternata, Aspergillus fumigatus, and Cladosporium herbarum. Medical records were documented at DCUMC. Patient demographic data, namely, age, sex, department, season, and diagnosis, were analyzed. This study was conducted in accordance with the principles of the Declaration of Helsinki.
2. MAST-CLA
The MAST-CLA Allergy test (Hitachi Chemical Diagnostics, Inc., CA, USA) was used. The two types of MASTpettes® were food panel and inhalant panel (Table 1). In the MASTpette® chamber, 64 cellulosic chambers are arranged in a ladder shape. The chambers consist of a positive control on the first line, negative control on the second line, anti-IgE on the third line, and 61 allergens from the 4th line to the 64th line. The test was performed according to the kit instructions. Patient's serum was added to the chamber, sensitized at room temperature for 18 h, and then washed three times with washing buffer. The enzyme-labeled anti-IgE antibody solution was added to the chamber, sensitized at room temperature for 4 h and washed three times, and the reaction solution was sensitized at room temperature for 30 min. The results were sorted into six classes, 0, 1/0, 1, 2, 3, and 4, using a MAST-CLA-1 luminometer. In this study, class 2 and above were classified as positive.
|
Allergen |
No. (%) |
|
|
Both type |
Dermatophagoides pteronyssinus mite |
404 (38.8) |
|
D. farinae mite |
344 (33.1) |
|
|
Storage mite |
9 (0.9) |
|
|
Cat |
115 (11.1) |
|
|
Dog |
99 (9.5) |
|
|
Egg white |
30 (2.9) |
|
|
Milk |
61 (5.9) |
|
|
Maize |
0 |
|
|
Sesame |
0 |
|
|
Soybean |
16 (1.5) |
|
|
Crab |
52 (5.0) |
|
|
Shrimp |
31 (3.0) |
|
|
Potato |
10 (1.0) |
|
|
Apple |
3 (0.3) |
|
|
Cacao |
0 |
|
|
Peach |
24 (2.3) |
|
|
Mackerel |
17 (1.6) |
|
|
CCD (bromelain) |
0 |
|
|
Rye pollens |
137 (13.1) |
|
|
House dust |
182 (17.5) |
|
|
Cockroach |
77 (7.4) |
|
|
Cladosporium herbarum |
541 (52.1) |
|
|
Aspergillus fumigatus |
209 (20.1) |
|
|
Alternaria alternata |
818 (78.8) |
|
|
Alder |
92 (8.8) |
|
|
Birch |
0 |
|
|
Oak white |
28 (2.7) |
|
|
Ragweed |
38 (3.7) |
|
|
Mugwort |
96 (9.2) |
|
|
Japanese hop |
0 |
|
|
Food panel |
Pork |
20 (7.0) |
|
Beef |
10 (3.5) |
|
|
Cheddar cheese |
6
(2.1) |
|
|
Chicken |
12
(4.2) |
|
|
Pupa, silk cocoon |
0 |
|
|
Tomato |
30 (10.6) |
|
|
Kiwi |
0 |
|
|
Mango |
0 |
|
|
Banana |
0 |
|
|
Citrus mix |
28
(9.9) |
|
|
Peanut |
50 (17.6) |
|
|
Walnut |
42 (14.8) |
|
|
Chestnut |
0 |
|
|
Wheat flour |
24 (8.5) |
|
|
Barley meal |
10
(3.5) |
|
|
Rice |
34 (12.0) |
|
|
Buck wheat |
30 (10.6) |
|
|
Garlic |
10
(3.5) |
|
|
Onion |
20
(7.0) |
|
|
Celery |
0 |
|
|
Cucumber |
0 |
|
|
Codfish |
10
(3.5) |
|
|
Mussel |
0 |
|
|
Tuna |
18
(6.3) |
|
|
Salmon |
10
(3.5) |
|
|
Clam |
0 |
|
|
Squid |
0 |
|
|
Anchovy |
0 |
|
|
Yeast, bakers |
0 |
|
|
Mushroom |
0 |
|
|
Candida
albicans |
54 (19.0) |
|
|
Inhalant
panel |
Acarus
siro |
122
(16.1) |
|
Horse |
0 |
|
|
Guinea pig |
0 |
|
|
Sheep |
0 |
|
|
|
Rabbit |
0 |
|
Hamster |
0 |
|
|
Hazel |
0 |
|
|
Sweet vernal grass |
83 (11.0) |
|
|
Bermuda grass |
8 (1.1) |
|
|
Orchard grass |
92 (12.2) |
|
|
Timothy grass |
9 (1.2) |
|
|
Reed |
71 (9.4) |
|
|
Redtop, bent grass |
0 |
|
|
Honey bee |
0 |
|
|
Yellow jacket |
0 |
|
|
Latex |
0 |
|
|
Penicillium notatum |
148 (19.6) |
|
|
Sycamore mix |
74 (9.8) |
|
|
Sallow mix |
0 |
|
|
Poplar mix |
38 (5.0) |
|
|
Ash mix |
29 (3.8) |
|
|
Pine |
44 (5.8) |
|
|
Japanese cedar |
107 (14.2) |
|
|
Acacia |
0 |
|
|
Hinoki cypress |
0 |
|
|
Oxeye daisy |
74 (9.8) |
|
|
|
Dandelion |
72 (9.5) |
|
|
English plantain |
0 |
|
|
Russian thistle |
0 |
|
|
Goldenrod |
0 |
|
|
Pigweed |
0 |
3. Statistical analysis
All gathered data were coded as numerical values. Descriptive data are expressed in percentage and mean ± standard deviation. The analysis was performed using SPSS 19.0 version (SPSS, Inc., Chicago, USA). Spearman's correlation coefficient was used to investigate the relationship between the number of positive fungal allergens and other sensitized allergens.
1. Demographic analysis of all patients
A total of 1,040 patients had positive reactions to at least one fungal allergen using the MAST-CLA (Table 1). During the same time, we performed 3,450 MAST-CLA tests, and only 1040 patients (30.14%) showed a positive reaction to the fungal allergens. Among the fungal species, patients mostly showed sensitivity to A. alternata, followed by C. herbarum and A. fumigatus (78.8% vs. 52.1% vs. 20.1%). Patients' sex, age, season, department, and diagnosis were analyzed. Male predilection was observed with 588 (56.3%) patients (Table 2). Patient age ranged from 1 to 96 years, and the mean value was 33.1 (Table 3). Patients in their 20s had the largest proportion (24.8%). In the seasonal evaluation, the proportion of patients who reported the occurrence of allergies was the largest during summer (30.0%) (Table 4). Most patients visited the otorhinolaryngology department, followed by dermatology and internal medicine (Table 5). Patient diagnosis varied from mostly allergic diseases to other systemic diseases. The most common diagnosis was allergic rhinitis, followed by urticaria, atopic dermatitis, allergic contact dermatitis, asthma, drug eruption, and hypereosinophilic syndrome (Table 6). Others include various skin diseases, such as irritant contact dermatitis, Stevens-Johnson syndrome, prurigo, or suspected allergies.
|
Variable |
Variable:
Number (%) |
|||||||
|
Sex |
Positive
fungal allergen |
Total |
||||||
|
1
only |
2
only |
3
only |
1+2 |
2+3 |
1+3 |
1+2+3 |
||
|
Male |
81 (56.3) |
27 (55.1) |
279 (64.1) |
12 (44.4) |
6 (42.9) |
127 (50.4) |
56 (47.1) |
588 (56.3) |
|
Female |
63 (43.7) |
22 (44.9) |
156 (35.9) |
15 (55.6) |
8 (57.1) |
125 (49.6) |
63 (52.9) |
452 (43.7) |
|
Total |
144 (13.8) |
49 (4.7) |
435 (41.8) |
27 (2.6) |
14 (1.3) |
252 (24.2) |
119 (11.4) |
1,040 (100) |
|
Variable |
Variable:
Number (%) |
|||||||
|
Age |
Positive
fungal allergen |
Total |
||||||
|
1
only |
2
only |
3
only |
1+2 |
2+3 |
1+3 |
1+2+3 |
||
|
0~9 |
9 (6.3) |
8 (16.3) |
110 (25.3) |
1 (3.7) |
2 (14.3) |
22 (8.7) |
16 (13.4) |
168 (16.2) |
|
10~19 |
26 (18.1) |
3 (6.1) |
150 (34.5) |
6 (22.2) |
3 (21.4) |
49 (19.4) |
21 (17.6) |
258 (24.8) |
|
20~29 |
19 (13.2) |
3 (6.1) |
90 (20.7) |
5 (18.5) |
1 (7.1) |
37 (14.7) |
11 (9.2) |
166 (16) |
|
30 |
15 (10.4) |
6 (12.2) |
23 (5.3) |
5 (18.5) |
0 |
21 (8.3) |
11 (9.2) |
81 (7.8) |
|
40 |
9 (6.3) |
6 (12.2) |
14 (3.2) |
3 (11.1) |
3 (21.4) |
21 (8.3) |
16 (13.4) |
72 (6.9) |
|
50 |
26 (18.1) |
7 (14.3) |
14 (3.2) |
3 (11.1) |
2 (14.3) |
35 (13.9) |
12 (10) |
99 (9.5) |
|
60 |
20 (13.9) |
9 (18.4) |
12 (2.8) |
2 (7.4) |
2 (14.3) |
20 (7.9) |
16 (13.4) |
81 (7.8) |
|
70 |
13 (9) |
6 (12.2) |
18 (4.1) |
2 (7.4) |
0 |
42 (16.7) |
14 (11.8) |
95 (9.1) |
|
80 |
7 (4.9) |
1 (2) |
3 (0.7) |
0 |
1 (7.1) |
2 (0.8) |
2 (1.7) |
16 (1.5) |
|
90 |
0 |
0 |
1 (0.2) |
0 |
0 |
3 (1.2) |
0 |
4 (0.4) |
|
Total |
144 (13.8) |
49 (4.7) |
435 (41.8) |
27 (2.6) |
14 (1.3) |
252 (24.2) |
119 (11.4) |
1,040
(100) |
|
Variable |
Variable: Number (%) |
|||||||
|
Season |
Positive fungal allergen |
Total |
||||||
|
1 only |
2 only |
3 only |
1+2 |
2+3 |
1+3 |
1+2+3 |
||
|
Spring |
34 (23.6) |
22 (44.9) |
87 (20) |
10 (37) |
4 (28.5) |
44 (17.5) |
28 (23.5) |
229 (22) |
|
Summer |
51 (35.4) |
12 (24.5) |
142 (32.6) |
8 (29.6) |
4 (28.5) |
65 (25.8) |
29 (24.4) |
311 (30) |
|
Autumn |
28 (19.4) |
6 (12.2) |
96 (22.1) |
5 (18.5) |
2 (14.3) |
67 (26.6) |
29 (24.4) |
233 (22.4) |
|
Winter |
31 (21.5) |
9 (18.4) |
110 (25.3) |
4 (14.8) |
4 (28.5) |
76 (30.1) |
33 (27.7) |
267 (25.7) |
|
Total |
144 (13.8) |
49 (4.7) |
435 (41.8) |
27 (2.6) |
14 (1.3) |
252 (24.2) |
119 (11.4) |
1,040 (100) |
|
Variable |
Variable: Number (%) |
|||||||
|
Department |
Positive fungal allergen |
Total |
||||||
|
1 only |
2 only |
3 only |
1+2 |
2+3 |
1+3 |
1+2+3 |
||
|
DT |
58 (40.3) |
18 (36.7) |
144
(33.1) |
11 (40.7) |
6 (42.9) |
94 (37.3) |
43 (36.1) |
374
(36) |
|
IM |
34 (23.6) |
7 (14.3) |
52 (12) |
2 (7.4) |
2 (14.3) |
75 (29.8) |
37 (31.1) |
209
(20.1) |
|
ENT |
49 (34) |
21 (42.9) |
218
(50.1) |
13 (48.1) |
6 (42.9) |
79 (31.3) |
37 (31.1) |
423
(40.7) |
|
PD |
0 |
0 |
17 (3.9) |
0 |
0 |
2 (0.8) |
1 (0.8) |
20 (1.9) |
|
Others |
3 (2.1) |
3 (6.1) |
4 (0.9) |
1 (3.7) |
0 |
2 (0.8) |
1 (0.8) |
14 (1.4) |
|
Total |
144 (13.8) |
49 (4.7) |
435
(41.8) |
27 (2.6) |
14 (1.3) |
252 (24.2) |
119 (11.4) |
1,040 (100) |
|
Variable |
Variable:
Number (%) |
|||||||
|
Diagnosis |
Positive fungal allergen |
Total |
||||||
|
1 only |
2 only |
3 only |
1+2 |
2+3 |
1+3 |
1+2+3 |
||
|
AD |
18 |
10 |
42 |
2 (7.4) |
0 |
38 |
23 |
133 (12.8) |
|
Urticaria |
22 |
7 |
82 |
7 |
2 |
45 |
11 |
176 (16.9) |
|
ACD |
10 |
7 |
17 |
1 |
1 |
12 |
2 |
50 (4.8) |
|
AR |
51 |
13 |
233 |
12 (44.4) |
6 |
81 |
40 |
436 (41.9) |
|
Hypereosinophilic |
3 |
0 |
2 |
0 |
0 |
1 |
0 |
6 (0.6) |
|
Asthma |
6 |
3 |
7 |
2 |
0 |
11 |
7 |
36 (3.5) |
|
Drug
eruption |
4 |
0 |
5 |
0 |
0 |
3 |
3 |
15 (1.4) |
|
Others |
30 |
9 (18.4) |
47 |
3 |
5 |
61 |
33 |
188 (18.1) |
|
Total |
144 |
49 |
435 |
27 |
14 |
252 |
119 |
1,040 |
2. Demographic analysis of patients with posi- tivity for fungal allergen and concurrent fungal allergens
Of the patients, 628 showed a positive reaction to only one fungal allergen: 144 (13.8%) patients to C. herbarum, 49 (4.7%) patients to A. fumigatus, and 435 (41.8%) patients to A. alternata. In addition, 293 patients had a positive reaction to two fungal allergens: 27 (2.6%) patients had positive reaction to C. herbarum and A. fumigatus, 14 (1.3%) to A. fumigatus and A. alternata, and 252 (24.2%) to C. herbarum and A. alternata. Moreover, 119 (11.4%) patients had a positive reaction to all three fungal allergens in the MAST-CLA.
For the demographic study, more male patients had a positive reaction to only one fungal allergen (61.6%), but more female patients had a positive reaction to multiple fungal allergens (51.2%).
Only a small number of younger patients showed a positive reaction to A. alternata. Patients showing a positive reaction to only C. herbarum or A. fumigatus were evenly distributed regardless of age. Patients showing multiple positive reactions to allergens were also evenly distributed. No significant difference was noted in other groups, except that A. alternata allergies occurred most frequently in the summer, indicating a seasonal distribution. Among the patients who visited the otorhinolaryngology department, most had positive reactions to only A. alternata and A. fumigatus. For patients who visited the dermatology department, most visits were due to a positive reaction to C. herbarum. The highest frequency of positive reactions to multiple allergens was observed in patients who visited the dermatology department. Among all groups, allergic rhinitis was the most common diagnosis in patients with a positive reaction to A. alternata.
3. Positive reactions to multiple allergens
Mites and house dust are associated with fungal allergens8. Among the mite species, Dermatophagoides pteronyssinus take up the largest proportion followed by D. farinae and house dust. When excluding mites and house dust, the most common concurrent allergens to C. herbarum are Penicillium and Acarus siro (flour mite). A. fumigatus showed the highest simultaneous positive reaction rate with rye and orch. A. alternata showed the highest simultaneous positive reaction rate with cats and dogs. Mites were the most common simultaneous positive allergens for patients with all three fungal allergens, followed by cedar, Penicillium, and house dust (Table 7).
|
Variable |
Variable: Number (%) |
|||
|
Rank |
Cladosporium
herbarum |
Aspergillus
fumigatus |
Alternaria
alternata |
All simultaneously positive |
|
1st |
Dermatophagoides pteronyssinus mite |
Dermatophagoides pteronyssinus mite |
Dermatophagoides |
Dermatophagoides |
|
2nd |
Dermatophagoides |
Dermatophagoides |
Dermatophagoides |
Dermatophagoides |
|
3rd |
House dust |
Rye |
House dust |
Cedar |
|
4th |
Penicillium |
House dust |
Cat |
Penicillium |
|
5th |
Acarus siro |
Orch |
Dog |
House dust |
|
6th |
Cat |
Sweet vernal grass |
Alder |
Acarus siro |
|
7th |
Rye |
Dandelion |
Rye |
Rye |
|
8th |
Dog |
Reed |
Acarus siro |
Candida |
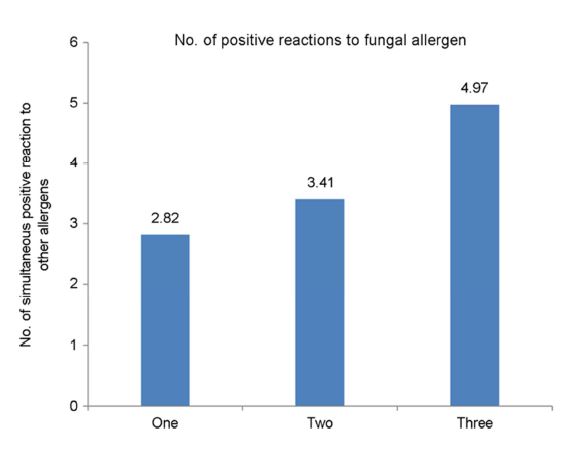
We examined the number of allergens showing simultaneously positive reactions to only one fungal allergen, two fungal allergens, and all three fungal allergens. When the reaction to only one fungal allergen was positive, the number of simultaneously positive allergens was 2.82 on average. When the reaction to two fungal allergens was positive, the number of simultaneously positive allergens was 3.41 on average. When the reaction to all three fungal allergens was positive, the number of other simultaneously positive allergens was 4.97 on average. Nonparametric method correlation analysis was performed, and Spearman's correlation coefficient showed a positive value of 0.129 (p < 0.05) (Figure 1).
People are exposed to allergens in various settings, both indoors and outdoors9-15. Fungi are ubiquitous airborne allergens and are important causes of various human diseases3,16. Several epidemiological and diagnostic studies reported the prevalence of fungal allergies using skin tests or IgE detection7,8,17. However, epidemiological investigation of fungal allergens has not been made yet. This is because identifying the role of specific fungi, which can cause allergy, is difficult18.
In this study, male patients were more likely to have a positive reaction to fungal allergens than female patients were. However, no significant difference was found between both sexes. In previous reports, the proportion of male patients who had atopic dermatitis, asthma, and hay fever were higher than female patients were, although these differences became narrower over time9,19. The incidence of allergic respiratory disease is higher in children than in adults. Longitudinal studies suggest that children with mild disease are likely to become asymptomatic as teenagers, whereas those with more severe disease will have symptoms that persist throughout their lifetime17. In one MAST-CLA study, the overall prevalence of positive allergens was the highest among teenagers. In that study, the 10~15 years age group showed the highest total IgE level, but the overall positive reaction rate and the number of positive allergens decreased with age. In the present study, teenagers had the largest proportion among all age groups. However, the prevalence of a positive reaction to multiple fungal allergens was distributed evenly in all age groups. This suggests that patients who are sensitized to multiple allergens may continue to be sensitized to multiple allergens over time.
C. herbarum and A. alternata allergies occur throughout the year, but they are highly observed in the late summer and autumn when plants grow20,21. The seasonal pattern of fungal spores has been reported to have little regional difference in the temperate zone, and domestic reports showed similar results8. In Korea, the growth of both types of fungi increased rapidly from mid-June and decreased at the end of October, and there was a slight increase in winter22. Meanwhile, A. fumigatus is usually considered an indoor fungus, rarely found in outdoor air, and can be found throughout the year23. Similar to previous studies, in this study, sensitization to fungus commonly occurs in summer. However, the proportion of patients who were sensitized in the winter was lower compared to that during summer. In particular, no particular seasonal difference was found for positive reactions to multiple fungal allergens. Therefore, seasonal deviations suggest that the frequency of patients having positive reactions to multiple fungal allergens is not significantly different by season.
Many studies have reported that exposure to fungus can cause an allergic reaction7,17,24-31. Respiratory symptoms have been mostly reported, which is thought to be an allergic reaction caused by fungal spores floating in the air25-31. There are also reports of allergic reactions due to skin contact with spores32. Allergies to fungi are often expressed as type I immediate, IgE-mediated hypersensitivity17. Atopic sensitization can manifest as asthma, rhinitis or conjunctivitis, urticaria, or atopic dermatitis10. Sometimes, an allergic reaction can be expressed as a type II hypersensitivity reaction17. An example of type III hypersensitivity is allergic alveolitis and bronchopulmonary aspergillosis (ABPA)33. ABPA is a pulmonary disease caused by hypersensitive Th2 response to A. fumigatus, which can worsen asthma and the condition of patients with cystic fibrosis34. Allergy to A. fumigatus is common in atopic asthma as well as in patients with cystic fibrosis34. Bronchopulmonary aspergillosis is characterized by wheezing and pulmonary infiltrates, which can lead to pulmonary fibrosis or bronchitis34. However, it is difficult to judge whether allergic diseases are clearly caused by fungi. This is because of the difficulty in finding the cause of allergic diseases, and patient distribution in each institution varies. In this study, patients are mostly diagnosed with allergic rhinitis, followed by dermatologic diseases. Thus, to determine the frequency of allergic diseases caused by fungi, clearly identifying allergens through multicenter studies is necessary.
Patients with allergies often have allergies to multiple allergens. Patients with positive reactions to multiple allergens are often identified through the MAST-CLA test2. Several studies reported on the positive reaction to each allergen in the MAST-CLA test, but information on the positive reaction to a combination of allergens and fungal allergens in the MAST-CLA panel is still unclear35-38. In many reports, D. farinae mite and D. pteronyssinus mite were the most commonly found co-existing allergens in the MAST-CLA test, and in this study, the positive reaction rate to D. farinae mite and D. pteronyssinus mite was the highest for both groups of patients who had a positive reaction to single and multiple fungal allergens39-42. In addition, we investigated allergens that showed the highest co-positive allergenic rate excluding mites and house dusts, which are well-known co-positive allergens. Regarding C. herbarum, A. siro was the most commonly observed co-positive allergen followed by the cat, rye, and dog. Regarding A. fumigatus, rye was the most commonly observed co-positive allergen followed by orch, sweet vernal grass, dandelion, and reed. Regarding A. alternata, the cat was a most commonly observed co-positive allergen followed by the dog, alder, rye, and A. siro. For allergens showing simultaneously positive reactions to all three fungal allergens, cedar rye was the most commonly observed co-positive allergen, followed by A. siro and rye.
In one study, the MAST-CLA panel allergens were divided into eight allergens with high simultaneous allergenicity, which were compared based on the similarity in the molecular structure. D. pteronyssinus mite, D. farinae mite, A. siro, house dust, dog, and cat were on cluster 519. Cross-reactivity among D. pteronyssinus mite, D. farinae mite, and A. siro are well established by Spitzauer et al., in which albumin was identified to demonstrate cross-reactivity to the aforementioned allergens43. House dust sensitization could be a result of co-sensitization to cat and dog, as they are all indoor allergens43.
In this study, we aimed to investigate the correlation between the number of positive reactions to fungal allergens and the number of positive reactions to other sensitized allergens. The correlation analysis showed a positive correlation. This suggests that the number of positive reactions to fungal allergens has a positive correlation with the number of positive reactions to sensitized allergens. The most common allergens that showed multiple positive reactions with fungi were pollens, cat, and dog.
Despite our findings, it is difficult to conclude whether the multiple positive reactions are co-sensitizations caused by exposure to each allergen and whether the multiple positive reactions are cross-reactivities caused by one allergen, in which the patient had previous exposure, and other allergens that show similar structure, but the patient had no previous exposure2.
The robustness of the allergen test has not yet been confirmed because the substances used in the allergen test are not quantified. Until now, only the molecular structures of the substances are identified, but their characteristics are unknown. Amino acid sequence, three-dimensional structure, and gene structure of allergic reactions were elucidated only recently. The development of allergen diagnostic reagents made of recombinant antigens will enable cross-reactivity and simultaneous sensitization and will be useful for the diagnosis and differential diagnosis of allergic disease and immunotherapy.
Fungal allergens are still the major causes of numerous allergic diseases. The demographic results of this study are not much different from those in previous studies, but the present results are meaningful as they help determine the occurrence of fungal allergens in southeastern Korea. This study provides useful information on the positive reactions to multiple allergens associated with fungal allergens. Therefore, the results can be used in choosing allergens when applying avoidance therapy.
Nevertheless, this study had some limitations. This study was conducted in one center in Korea; hence, it does not fully reflect regional and ethnic differences. Further multicenter studies and studies involving patients in other regions are needed. Moreover, data on the relationship between the clinical signs and positivity of fungal allergens will be more meaningful information to clinicians. Despite these limitations, this study can be a good reference for clinicians when educating patients with allergic diseases.
References
1. Lim HS, Yoon JK, Lee HH. Allergen pattern using MAST CLA test in Korean pediatric patients. Korean J Clin Pathol 2001;21:292-297
Crossref
Google Scholar
2. Kim HS, Kim DJ, Lee SG. Analysis of simultaneous positivity to multiple allergens on MAST CLA test. Korean J Lab Med 2005;25:448-456
Crossref
Google Scholar
3. Ezeamuzie CI, Al Ali S, Khan M, Hijazi Z, Dowaisan A, Thomson MS, et al. IgE-mediated sensitization to mould allergens among patients with allergic respiratory diseases in a desert environment. Int Arch Allergy Immunol 2000; 121:300-307
Crossref
Google Scholar
4. Nolles G, Hoekstra MO, Schouten JP, Gerritsen J, Kauffman HF. Prevalence of immunoglobulin E for fungi in atopic children. Clin Exp Allergy 2001;31:1564-1570
Crossref
Google Scholar
PubMed
5. D'Amato G, Chatzigeorgiou G, Corsico R, Gioulekas D, Jäger L, Jäger S, et al. Evaluation of the prevalence of skin prick test positivity to Alternaria and Cladosporium in patients with suspected respiratory allergy. A European multicenter study promoted by the Subcommittee on Aerobiology and Environmental Aspects of Inhalant Allergens of the European Academy of Allergology and Clinical Immunology. Allergy 1997;52:711-716
Crossref
Google Scholar
6. Corsico R, Cinti B, Feliziani V, Gallesio MT, Liccardi G, Loreti A, et al. Prevalence of sensitization to Alternaria in allergic patients in Italy. Ann Allergy Asthma Immunol 1998;80: 71-76
Crossref
Google Scholar
PubMed
7. Wioletta A. Żukiewicz-Sobczak. The role of fungi in allergic diseases. Postep Derm Alergol 2013;30:42-45
Crossref
Google Scholar
PubMed
8. Fukutomi Y, Taniguchi M. Sensitization to fungal allergens: resolved and unresolved issues. Allergol Int 2015;64:321 -331
Crossref
Google Scholar
PubMed
9. Mari A, Schneider P, Wally V, Breitenbach M, Simon-Nobbe B. Sensitization to fungi: epidemiology, comparative skin tests, and IgE reactivity of fungal extracts. Clin Exp Allergy 2003;33:1429-1438
Crossref
Google Scholar
10. Crameri R, Zeller S, Glaser AG, Vilhelmsson M, Rhyner C. Cross-reactivity among fungal allergens: A clinically relevant phenomenon? Mycoses 2008;52:99-106
Crossref
Google Scholar
PubMed
11. Katz Y, Verleger H, Barr J, Rachmiel M, Kivity S, Kuttin ES. Indoor survey of moulds and prevalence of mould atopy in Israel. Clin Exp Allergy 1999;29:186-192
Crossref
Google Scholar
PubMed
12. Gupta R, Singh BP, Sridhara S, Gaur SN, Kumar R, Chaudhary VK, et al. Identification of cross-reactive proteins amongst different Curvularia species. Int Arch Allergy Immunol 2002;127:38-46
Crossref
Google Scholar
PubMed
13. Helbling A, Brander KA, Horner WE, Lehrer SB. Allergy to basidiomycetes. Chem Immunol 2002;81:28-47
Crossref
PubMed
14. D'Amato G, Spieksma FT. Aerobiologic and clinical aspects of mould allergy in Europe. Allergy 1995;50:870-877
Crossref
Google Scholar
PubMed
15. Bush RK, Portnoy JM. The role and abatement of fungal allergens in allergic diseases. J Allergy Clin Immunol 2001; 107:430-440
Crossref
Google Scholar
PubMed
16. Woodfolk JA. Allergy and dermatophytes.Clin Microbiol Rev 2005;18:30-43
Crossref
PubMed
17. Simon-Nobbe B, Denk U, Poll V, Rid R, Breitenbach M. dermatophytes. The spectrum of fungal allergy. Int Arch Allergy Immunol 2008;145:58-86
Crossref
Google Scholar
PubMed
18. Shin JH. Fungus and allergy. Pediatr Allergy Respir Dis 1999; 9:13-23
Crossref
19. Ohn J, Paik SH, Doh EJ, Park HS, Yoon HS, Cho S. Allergen sensitization pattern by sex: a cluster analysis in Korea. Ann Dermatol 2017;29:735-741
Crossref
Google Scholar
20. Matsson P, Hamilton RG, Adkinson NF, Esch R, Homeburger HA, Maxim P, et al. Evaluation methods and analytical performance characteristics of immunologic assays for human immunoglobulin E (IgE) antibodies of defined allergen specificities. National Committee for Clinical Laboratory Standards (NCCLS), Wayne, PA, Approved guideline Ⅰ/LA20-A. 1997
Crossref
21. Beaumont F, Kauffman HF, van der Mark TH, Sluiter HJ, de Vries K. Volumetric aerobiological survey of conidial fungi in the North-East Netherlands. Ⅰ. Seasonal patterns and the influence of metrological variables. Allergy 1985; 40:173-180
Crossref
Google Scholar
22. Oh JW, Lee HB. Aerobiological study for airborne pollen and mold in Kuri-shi, Kyunggi-Do. Pediatr Allergy Respir Dis 1997;7:57-68
Crossref
Google Scholar
23. D'Amato G1, Spieksma FT. Aerobiol Aerobiologic and clinical aspects of mould allergy in Europe. Allergy 1995; 76:819-825
Crossref
Google Scholar
24. Crameri R, Garbani M, Rhyner C, Huitema C. Fungi: the neglected allergenic sources. Allergy 2014;69:176-185
Crossref
Google Scholar
PubMed
25. Scheynius A, Johansson C, Buentke E, Zargari A, Tengvall LM. Atopic eczema/dermatitis syndrome and Malassezia. Int Arch Allergy Immunol 2002;127:161-169
Crossref
Google Scholar
PubMed
26. Torricelli R, Johansson SG, Wuthrich B. Ingestive and inhalantive allergy to the mushroom Boletus edulis. Allergy 1997;52:747-751
Crossref
Google Scholar
PubMed
27. Kivity S, Schwarz Y, Fireman E. The association of perennial rhinitis with Trichophyton infection. Clin Exp Allergy 1992;22:498-500
Crossref
Google Scholar
PubMed
28. Scalabrin DM, Bavbek S, Perzanowski MS, Wilson BB, Platts-Mills TA, Wheatley LM. Use of specific IgE in assessing the relevance of fungal and dust mite allergens to atopic dermatitis: a comparison with asthmatic and nonasthmatic control subjects. J Allergy Clin Immunol 1999;104:1273 -1279
Crossref
Google Scholar
29. Dales RE, Cakmak S, Burnett RT, Judek S, Coates F, Brook JR. Influence of ambient fungal spores on emergency visits for asthma to a regional children's hospital. Am J Respir Crit Care Med 2000;162:2087-2090
Crossref
Google Scholar
30. Nissen D, Petersen LJ, Esch R, Svejgaard E, Skov PS, Poulsen LK, et al. IgE-sensitization to cellular and culture filtrates of fungal extracts in patients with atopic dermatitis. Ann Allergy Asthma Immunol 1998;81:247-255
Crossref
Google Scholar
31. Neukirch C, Henry C, Leynaert B, Liard R, Bousquet J, Neukirch F. Is sensitization to Alternaria alternata a risk factor for severe asthma? A population-based study. J Allergy Clin Immunol 1999;103:709-711
Crossref
Google Scholar
32. Lacey J. Fungi and Actinomycetes as allergens. In:Kay AB ed. Allergy and allergic diseases, 1st ed. Oxford: Blackwell Science, 1998:858-887.
Crossref
33. Bogacka E, Matkowski K. Effect of fungi on human health. Mikologialekarska 2001;8:175-178
Crossref
34. Knutsen AP, Slavin RG. Allergic bronchopulmonary Aspergillosis in asthma and cystic fibrosis. Clin Dev Immunol 2011; 2011:843763
Crossref
Google Scholar
35. Yu YI, Cho JS, Lee KH, Kim GH, Hong SM, Kim SW. A clinical statistics on allergens of allergic rhinitis: Prevalence of mixed sensitization. Korean J Otolaryngol 2003;46:48 -53
Crossref
36. Yun YY, Ko SH, Park JW, Hong CS. Cross-reactivity between pollens in patients sensitized to multiple pollens. Korean J Asthma Allergy Clin Immunol 1999;19:584-593
Crossref
Google Scholar
37. Mothes N, Horak F, Valenta R. Transition from a botanical to a molecular classification in tree pollen allergy: Implica- tions for diagnosis and therapy. Int Arch Allergy Immunol 2004;135:357-373
Crossref
Google Scholar
38. Ferreira F, Hawranek T, Gruber P, Wopfner N, Mari A. Allergic cross-reactivity: from gene to clinic. Allergy 2004; 59:243-267
Crossref
Google Scholar
PubMed
39. Lee EJ, Piao YJ, Kim KH, Suhr KB, Lee JH, Park JK. The relationship among the clinical evaluation, total IgE, and allergen-specific IgE of MAST-CLA in atopic dermatitis. Korean J Dermatol 2003;41:197-206
Crossref
Google Scholar
40. Park KI, Chun HS, Shin JW, Kim HS, Song KS. Allergen frequencies on MAST CLA by age groups using new Korean panel. J Clin Pathol Quality Control 1999;21:243-249
Crossref
Google Scholar
41. Yang SE, Oh HB, Hong SJ, Moon DH, Chi HS, Analysis of MAST chemiluminescent assay (MAST CLA) results performed in Asan medical center. Korean J Clin Pathol 1998; 18:606-606
Crossref
Google Scholar
42. Lee SR, Lee HR, Keum DG. Evaluation of the MAST-CLA allergy system (Korea IgE panel) for diagnosis of atopic allergy. Korean J Clin Pathol 1995;15:469-477
Crossref
43. Spitzauer S, Pandjaitan B, Mühl S, Ebner C, Kraft D, Valenta R, et al. Major cat and dog allergens share IgE epitopes. J Allergy Clin Immunol 1997;99:100-106
Crossref
Google Scholar
PubMed
Congratulatory MessageClick here!
