pISSN : 3058-423X eISSN: 3058-4302
Open Access, Peer-reviewed
pISSN : 3058-423X eISSN: 3058-4302
Open Access, Peer-reviewed
Hyun-Bin Kwak,Su Kyung Park,Seok Kweon Yun,Han Uk Kim,Jin Park
http://dx.doi.org/10.17966/KJMM.2017.22.1.42 Epub 2017 March 31
Abstract
Keywords
Purpureocillium lilacinum Paecilomyces lilacinus
서 론
Purpureocillium lilacinum(과거 Paecilomyces lila- cinus)은 hypomycetes에 속하는 진균이며 주로 토양과 식물의 부패과정에서 발견된다. 임상 검체에서는 대개 오염균으로 분류되지만 당뇨, 악성종양, 혈액질환 등 면역기능이 저하된 환자에서 주로 안구감염의 형태로 발생하며 드물게는 특별한 유발요인 없이 피부감염을 일으키는 경우도 있다. 균주 중에는 Paecilomyces lilacinus가 인체감염을 가장 잘 일으키는 것으로 알려져 있다[1]. Purpureo- cillium lilacinum은 1907년 Penicillium lilacinum으로 명명된 이후, 1974년 Paecilomyces lilacinus로 변경되었으며 2011년 계통발생학적 분석을 통해 Paecilomyces 속에서 분리되어 Purpureocillium이라는 새로운 속으로 재분류되었다[2]. 국내 문헌 상 Purpureocillium lilacinum에 의한 피부감염증은 4예만이 보고되어 있으나, 이들 모두 새로운 분류법이 아닌 이전 분류에 따라 Paecilomyces lilacinus에 의한 감염으로 명명되어 보고되어 있다[3],[4],[5],[6].
저자들은 건강한 81세 남성의 좌측 손등에 발생한 Purpureocillium lilacinum에 의한 국소 피부감염증 1예를 진균 배양검사 및 분자생물학 검사를 통해 진단하고 문헌고찰과 함께 보고한다.
증 례
환 자: 양 OO, 81세, 남자
주 소: 좌측 손등의 홍반성 인설성 판
현병력: 내원 3개월 전 좌측 손등에 홍반성 구진과 농포가 발생하였고, 며칠 후 가피를 동반한 홍반성 판으로 변하였다.
과거력: 특이 사항 없음.
가족력: 특이 사항 없음.
이학적 검사: 전신상태는 양호하였으며, 이학적 검사 상 피부 병변 이외에 폐, 중추신경계, 신장 등 다른 장기의 침범을 의심할 만한 소견은 관찰할 수 없었다.
피부 소견: 좌측 손등에 5.0 × 5.0 cm 크기의 비교적 경계가 명확하고 가피를 동반한 홍반성 판이 관찰되었다(Fig. 1).

검사 소견: 일반혈액검사, 소변검사, 간기능 및 신기능검사와 매독혈청반응검사, 흉부 X-선검사, 심전도 검사는 모두 정상 범위 내지 음성이었다.
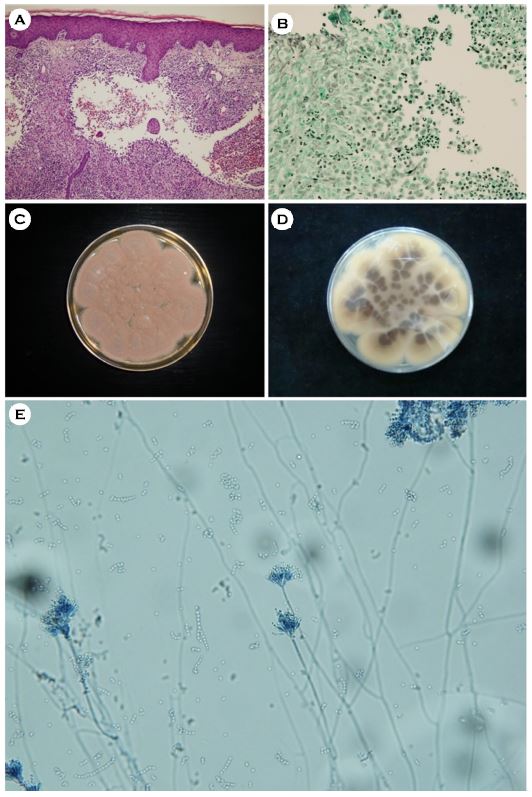
병리조직학적 소견: 유두진피에서 림프구, 조직구와 다핵거대 세포로 구성된 만성 육아종, 농양 형성이 관찰되었고(Fig. 2A), Periodic acid-Schiff 염색에서 유두진피 내 붉은색의 균사와 포자가 관찰되었으며, methenamine silver 염색에서는 검은색의 균사와 포자가 관찰되었다(Fig. 2B).
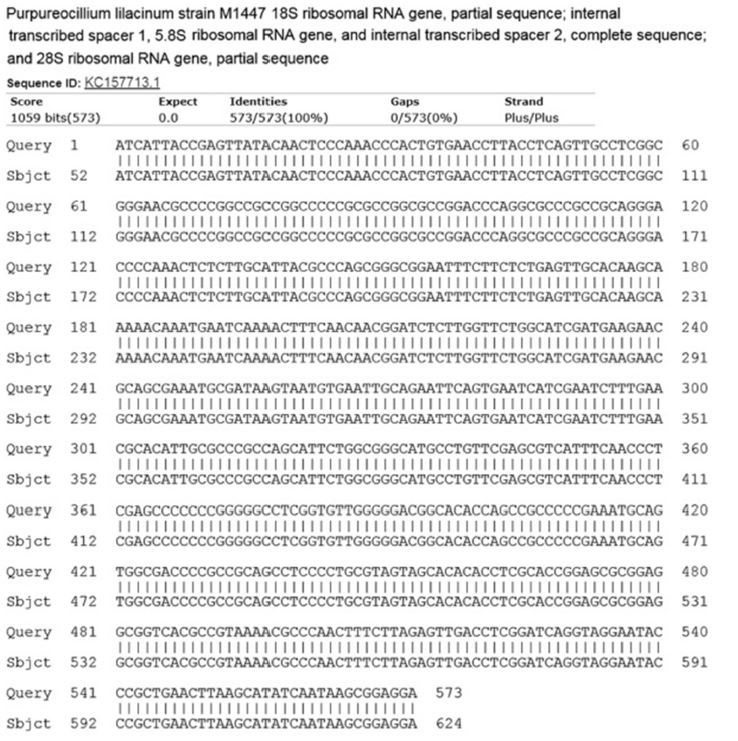
분자생물학적 검사: 환자의 배양된 균집락으로부터 DNA를 분리하여 진균핵 내의 internal tran-scribed spacer (ITS) 부위의 염기서열을 얻은 후 BLAST를 이용하여 GenBank에 있는 Purpureo- cillium lilacinum의 ITS 부위의 염기서열인 Pur- pureocillium lilacinum strain M1447 (GenBank acces- sion number KC157713)과 비교한 결과 100% 일치하여 Purpureocillium lilacinum으로 최종 동정하였다(Fig. 3).
치료 및 경과: 1일 itraconazole 200 mg을 2주간 경구 투여하여 홍반성 판의 크기와 두께가 줄어들면서 병변은 일부 호전되었으나, 이후 환자가 내원하지 않아 추적 관찰은 중단되었다.
고 찰
Purpureocillium 균종은 인체 감염의 드문 원인균으로 손톱바닥(nail bed) 감염부터 심부 조직 침범까지 다양한 범위를 가진다[7]. 이 균종은 Peni- cillium 및 Aspergillus 균종과 관련된 saprophytic mold로 처음 보고되어 1907년 Penicillium lilacinum으로 처음 명명된 이후 1974년 Paecilomyces lila- cinus로 변경되었다. 하지만 2000년대 Paecilo- myces 속이 단일계통이 아님이 밝혀지면서 2011년 Luangsa-Ard 등[2]의 상세한 계통발생학적 분석을 통해 유연관계가 깊다고 알려진 Paecilomyces nostocoides, Isaria takamizusanensis과 함께 잠자리동충하초과(Ophiocordycipitaceae family) 내 Pur- puerocillium이라는 새로운 속(genus)으로 분류되었고 Paecilomyces lilacinus는 Purpureocillium lilacinum으로 다시 명명되었다. 이후 2013년 Perdomo 등[9]이 Purpureocillium lilacinum의 종내 유전학적 다양성을 확인하기 위해 4개의 다른 부위(ITS, 28S rDNA, EF-1α, RNA polymerase II)의 유전적 정보를 이용한 다측면분류법을 시행한 결과, Purpureo- cillium lilacinum과 Paecilomyces nostocoides는 동종임을 재차 확인하였으며, Isaria takamizusanensis도 Purpureocillium lilacinum과 가장 가까운 계통으로 확인되어 Purpureocillum 속으로 함께 분류될 수 있음을 재차 확인하였다.
Purpureocillium lilacinum은 1972년에 흉막 삼출액에서 처음으로 동정되었으며, Purpureocillium lilacinum에 의한 국소 피부감염은 1977년 Takayasu 등이 얼굴에 생긴 연조직염의 형태로 처음 보고하였다[10],[11],[12]. 이 균은 개체의 면역 능력이 감소한 경우, 장기이식이나 기타 수술적 술기 이후 또는 기회감염에 노출되어 있는 경우에 감염을 잘 유발하지만[13], 최근에는 특별한 유발 요인 없이 정상인에서도 감염의 빈도가 증가하고 있다[7].
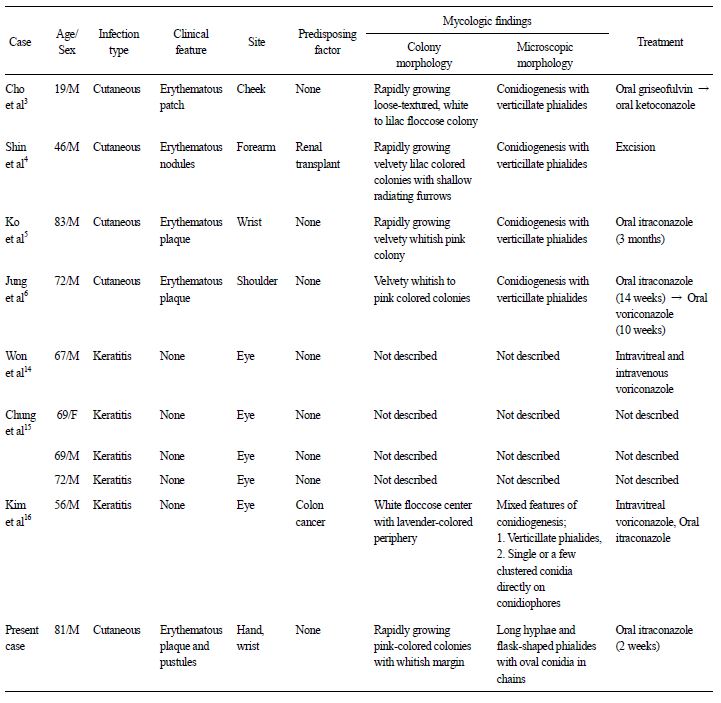
국내 피부과 문헌에서는 총 4예의 피부감염[3],[4],[5],[6], 안과 문헌에서는 총 5예[14],[15],[16](Table 1)의 안구감염이 보고되었는데, 최근 보고된 안감염 1예[16]를 제외하고는 모두 이전 분류에 따른 명명 법에 따라 보고되었으며, 새로운 계통발생학적 분석이 이루어진 2011년 이후 보고된 증례들도 Paecilomyces라는 이전 분류법을 따라 발표되었다[3],[14],[15]. 국내에 보고된 총 10예의 임상양상을 보면, 연령은 19세에서 83세까지 다양하였다. 피부 병변은 대개 홍반성 반점이나 판, 결절의 형태로 주로 노출 부위인 안면부, 팔에 발생하였다. 위험인자로는 2예가 콩팥이식술 후 장기간 면역억제제를 복용중인 환자 및 대장암을 진단받아 보조화학요법을 시행 받고 있는 환자에서 감염증이 발생하였으며, 나머지 8예는 위험인자가 없는 정상인에서 발생하였다. 본 증례에서도 환자는 특별한 위험인자 없는 면역정상인이었으며, 직업상 평소 손의 노출이 많은 농부인 것과 손등에 병변이 발생한 것으로 보아 환자가 기억하지 못하는 미세한 외상과 연관이 있을 것으로 추정된다.
Purpureocillium 감염증의 진단은 전통적으로 진균학적 배양과 현미경적 소견 및 병리조직학적 소견에 의해 이루어져 왔으며, 최근에는 분자생물학적 방법이 보완적으로 이용되고 있다[16]. Pur- pureocillium lilacinum은 Sabouraud dextrose agar 배지에서 실온 배양하면 빠르게 성장하여 흰색, 연분홍색, 라일락색의 돔 모양의 집락을 형성한다. 초기에는 집락의 표면이 흰색을 보이지만 점차 라일락색으로 변하고 주변으로 퍼져나가는 얕은 주름들이 생기며, 집락의 뒷면은 라일락색을 보이고 일부는 갈색 또는 짙은 갈색을 보인다[5],[6]. 일반적으로 Purpureocillium lilacinum은 lactophenol cotton blue 염색상 기저부는 부풀어 있고 긴 목을 가진 전형적인 플라스크 모양의 phialides가 중심축으로부터 약간 구부러진 모양을 띤다[17]. Purpureocillium lilacinum은 현미경적으로 두 가지 형태의 분생자 형성, 즉 분생자가 윤생구조의 경자로부터 기시하는 형태와 단일한 분생자병으로부터 기시하는 형태가 동시에 관찰될 수 있다[16]. 현미경적으로 두 가지 형태의 분생자 형성이 동시에 보이는 것은 일반적으로 오염을 시사하지만 집락의 형태가 단일한 경우 Purpureocillium lilacinum을 감별하여야 한다. 국소 피부감염증 4예에서는 Purpureocillium lilacinum의 형태학적 소견에 대해 기술되어 있으나, 모두 단일한 구조만을 기술하여 Paecilomyces 속에 합당한 형태만을 언급하고 있다. 모두 Purpureocillium lilacinum을 Purpureocillium이라는 새로운 속으로 보고하지 않고 Paecilomyces lilacinus로 보고하여 Paecilomyces 속에 합당하지 않은 구조에 대해서는 기술하지 않은 것으로 추정된다. 또한 현미경적으로 특징적인 경자의 윤생구조를 보일 경우 Purpureocillium lilacinum의 종 수준의 동정을 위하여 분자생물학적 동정법을 이용하는 것이 효과적일 것이다. 본 증례에서는 병변 부위의 조직을 25℃에서 15일간 배양한 결과 Purpureocillium lilacinum의 진균학적인 특징과 동일한 소견을 보였으며 DNA 염기서열결정(sequencing) 검사로 최종 동정하였다.
Purpureocillium 균종에 의한 감염은 현재까지 임상적 자료가 부족하여 명확하게 정립된 치료법이 없고, 대체로 전신적 항진균제 투여 또는 외과적 절제술을 시행한다[6]. 따라서 항진균제 감수성 결과나 기존 치료 증례들을 기반으로 적절한 항진균제를 선택하는 것이 중요한데, amphotericin B, flucytosine, fluconazole에는 저항성을 나타내며, itraconazole의 경우 보고자마다 다양하나 대체적으로 제한적인 효과를 보이는 것으로 알려져 있다[11]. 반면 terbinafine이나 새로운 triazole계 약물인 voriconazole, ravuconazole, fosaconazole는 생체 외에서 감수성 검사에서 대체로 낮은 최소억제농도(MIC, minimum inhibitory concentration)를 보였다. 최근 들어 voriconazole 단독 요법으로 Purpureo- cilllium lilacinum에 의한 피부감염증을 효과적으로 치료한 증례들이 보고되고 있으며[6],[18],[19], voriconazole 400 mg를 약 3개월 정도 경구 투여하여 성공적으로 치료했다고 보고하였다. Terbinafine의 경우 생체 외 감수성 검사 결과와는 달리 단독 투여 시 9예의 피부감염증에서 치료실패를 보인 보고가 있다[6],[12],[13]. 단독 투여로 인한 치료실패를 줄이기 위해 병용 투여가 도움이 될 수 있는데, terbinafine과 voriconazole 혹은 ravoconazole의 병합 시 생체 외 감수성 검사에서 상승효과를 보인 바 있다[11],[20]. 국내 보고된 피부감염증의 경우, 1예에서는 griseo- fluvin 500 mg로 6주간 치료하였으나 호전이 없어 경구 ketoconazole 400 mg로 변경한 뒤 12주 만에 호전을 보였으며, itraconazole (200 mg/day)을 3개월 간 경구 투여 후 병변의 호전을 보인 예와 itraconazole (200 mg/day)을 14주 투여 후에도 호전이 없어 voriconazole (400 mg/d)로 10주간 변경 투여하여 효과적으로 치료한 증례가 있다.
저자들은 특별한 기저질환이 없는 건강한 환자에서 발생한 Purpureocillium lilacinum에 의한 국소 피부감염증 1예를 경험하고 문헌고찰과 함께 보고한다. 향후 진균학적 및 분자생물학적 진단을 통한 진단과 함께 새로운 계통발생학적 분류를 기반으로 보고가 필요할 것으로 생각된다.
Conflict of interest
In relation to this article, I declare that there is no conflict of interest.
References
1. Clark NM. Paecilomyces lilacinus infection in a heart transplant recipient and successful treatment with terbinafine. Clin Infect Dis 1999;28:1169-1170
Google Scholar
2. Clark NM. Paecilomyces lilacinus infection in a heart transplant recipient and successful treatment with terbinafine. Clin Infect Dis 1999;28:1169-1170
Google Scholar
3. Cho GY, Cho EH, Choi GJ, Hong NS, Houh W. Facial cutaneous mycosis by Paecilomyces lilacinus. Korean J Dermatol 1984;22:89-93
Google Scholar
4. Shin SB, Lee HN, Kim SW, Park GS, Cho BK, Kim HJ. Cutaneous abscess caused by Paecilomyces lilacinus in a renal transplant patient. Korean J Med Mycol 1998;3:185-189
Google Scholar
5. Ko WT, Kim SH, Suh MK, Ha GY, Kim JR. A case of localized skin infection due to Paecilomyces lilacinus. Korean J Dermatol 2007;45:930-933
Google Scholar
6. Jung MY, Park JH, Lee JH, Lee JH, Yang JM, Lee DY. A localized cutaneous Paecilomyces lilacinus infection treated with voriconazole. Korean J Dermatol 2013;51:833-836
Google Scholar
7. Van Schooneveld T, Freifeld A, Lesiak B, Kalil A, Sutton DA, Iwen PC. Paecilomyces lilacinus infection in a liver transplant patient: Case report and review of the literature. Transpl Infect Dis 2008;10:117-122
Crossref
Google Scholar
8. Sung GH, Hywel-Jones NL, Sung JM, Luangsa-ard JJ, Shrestha B, Spatafora JW. Phylogenetic classifi- cation of Cordyceps and the clavicipitaceous fungi. Stud Mycol 2007;57:5-59
Google Scholar
9. Perdomo H, Cano J, Gené J, García D, Hernández M, Guarro J. Polyphasic analysis of Purpureocillium lila- cinum isolates from different origins and proposal of the new species Purpureocillium lavendulum. Myco- logia 2013;105:151-161
Crossref
10. Fenech FF, Millia CP. Pleural effusion caused by Penicillium lilacinus. Br J Dis Chest 1972;66:284-290
Google Scholar
11. Pastor FJ, Guarro J. Clinical manifestations, treatment and outcome of Paecilomyces lilacinus infection. Clin Microbiol Infect 2006;12:948-960
Crossref
Google Scholar
12. Takayasu S, Akagi M, Shimizu Y. Cutaneous mycosis caused by Paecilomyces lilacinus. Arch Dermatol 1977;113:1687-1690
Crossref
Google Scholar
13. Gutierrez-Rodero F, Morganon M, Ortiz de la Tabla V, Mayoll MJ, Martin C. Cutaneous hyalohyphomycosis caused by Paecilomyces lilacinus in an immunocom- petent host successfully treated with itraconazole: Case report and review. Eur J Clin Microbiol Infect Dis 1999;18:814-818
Crossref
Google Scholar
14. Won JY, Shin JY, Hwang JH, Joo CK. A case of fungal keratitis caused by Paecilomyces lilacinus after pene- trating keratoplasty. J Korean Ophthalmol Soc 2014; 55:1384-1387
Google Scholar
15. Chung SR, You IC, Cho NC, Ahn M. Paecilomyces keratitis: Cases in Korea and literature review. J Korean Ophthalmol Soc 2016;57:390-398
Crossref
Google Scholar
16. Kim JR, Kim DH, Jang JH, Sung HS, Kim MN. A case of fungal keratitis caused by Purpureocillium lilacinum: A microbiological review of Korean cases. Korean J Med Mycol 2016;21:84-91
Google Scholar
17. Castro LG, Salebian A, Sotto MN. Hyalohyphomycosis by Paecilomyces lilacinus in a renal transplant patient and a review of human Paecilomyces species infec- tions. J Med Vet Mycol 1990;28:15-26
Google Scholar
18. Keshtkar-Jahromi M, McTighe AH, Segalman KA, Fothergill AW, Campbell WN. Unusual case of cuta- neous and synovial Paecilomyces lilacinus infection of hand successfully treated with voriconazole and review of published literature. Mycopathologia 2012; 174:255-258
Google Scholar
19. Huang CY, Sun PL, Tseng HK. Cutaneous hyalo- hyphomycosis caused by Paecilomyces lilacinus suc- cessfully treated by oral voriconazole and nystatin packing. Mycopathologia 2011;172:141-145
Crossref
20. Ortoneda M, Capilla J, Pastor FJ, Pujol I, Yustes C, Serena C, et al. In vitro interactions of approved and novel drugs against Paecilomyces spp. Antimicrob Agents Chemother 2004;48:2727-2729
Crossref
Google Scholar
