pISSN : 3058-423X eISSN: 3058-4302
Open Access, Peer-reviewed
pISSN : 3058-423X eISSN: 3058-4302
Open Access, Peer-reviewed

Hyun Ji Lee,Seok Min Kim,Dong Hyuk Eun,Weon Ju Lee,Yong Jun Bang,Jae Bok Jun
10.17966/JMI.2018.23.4.99 Epub 2019 January 02
Abstract
Background: Trichophyton verrucosum (T. verrucosum) is a zoophilic dermatophyte that causes ringworm in cattle and is prevalent worldwide. This dermatophyte may be responsible for various conditions, especially inflammatory skin lesions.
Objective: In this study, we aimed to investigate the changes in the clinical and epidemiological characteristics of T. verrucosum infections in southeastern Korea.
Methods: A total of 34 patients who visited the Catholic Skin Clinic and the Kyungpook National University Hospital in Daegu, Korea from 2005 to 2017 were diagnosed with T. verrucosum infection. The diagnosis was confirmed using fungal culture. The data were based on a retrospective survey of the medical records.
Results: The annual incidence of T. verrucosum infection was very low. There was no difference in the sexual incidence. T. verrucosum infection was most common among subjects in their fifties and sixties. The highest incidence was during the month of September. The arm was most frequently involved, followed by the face. This infection was predominant in patients living in rural areas.
Conclusion: These clinicoepidemiological findings provide useful information for understanding the changes in the infection caused by T. verrucosum. In particular, it was interesting to note that the incidence was very low, majority of the affected subjects were in their fifties and sixties, and the most commonly affected site was the arm.
Keywords
Epidemiology Trichophyton verrucosum
Dermatophytosis is a common infection observed world- wide and is believed to affect more than 20~25% of the global population1. In the last 80 years, considerable changes have been observed in dermatophytosis in Korea, including changes in the common causative agents of dermatophytosis and its clinical characteristics. The epidemiology of a dermatophyte infection is influenced by the changing patterns of migration, growth in tourism, host immune competence, pathogenicity of the infectious agent, availability of medical treatment, and changes in the socioeconomic conditions2-8. Zoonotic diseases can be transmitted between animals and from animals to humans, causing outbreaks among exposed individuals9.
Trichophyton verrucosum (T. verrucosum) is a zoophilic fungus known as the primary dermatophyte causing ringworm among cattle in Europe, North America, and other countries. Humans are typically infected via direct contact with the infected cattle, contaminated fomites, or soil; T. verrucosum infection is observed worldwide10. Kerion celsi caused by T. verrucosum was first reported in the southwestern province of Korea in 1986 by Kim et al.11. Thereafter, several patients have been infected with T. verrucosum in the Young-nam province12-15. However, recently, the incidence of T. verrucosum infection has been decreasing.
In the present study, we investigated the changes in the epidemiology of T. verrucosum through a retrospective analysis of patient medical records from 2005 to 2017 and compared the data with our previous report on the data from 1986 to 2004.
1. Patients
We performed a retrospective analysis of the medical records of patients who visited the Catholic Skin Clinic and Kyungpook National University Hospital in Daegu from 2005 to 2017. The clinical and epidemiological characteristics of 34 patients infected with T. verrucosum were studied. Furthermore, the medical records were compared with those of 196 patients with T. verrucosum infection between 1986 and 2004. T test was used for the statistical analyses. p < 0.05 was considered to be statistically significant.
2. Methods
Total 34 patients with T. verrucosum were retrospectively reviewed to determine the annual incidence of the infection and its distribution as per age, sex, season, infection site, and place of residence. The diagnosis of T. verrucosum infection was confirmed with macroscopic and microscopic morphological examinations of the cultured colonies. Samples of the fungal examination were obtained by scraping the lesions with a scalpel and culturing them using potato dextrose agar-corn meal Tween 80 media. The cultures were kept at 24~26℃ and examined after 2~4 weeks.
1. Annual incidence
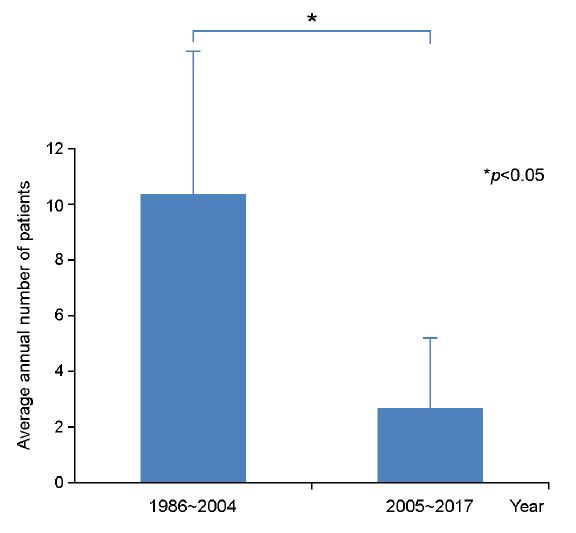
Total 34 patients were diagnosed with T. verrucosum infection (0.00041% among the whole dermatophytosis), and the annual incidence ranged from 0~8 (Table 1). The prevalence of T. verrucosum infection was significantly lower than that in our previous study (p < 0.05), with a decrease in the annual incidence from 10.3 to 2.6 (Figure 1). Although the incidence of T. verrucosum infection was very low, cases are still observed in Korea.
|
Year |
2005 |
2006 |
2007 |
2008 |
2009 |
2010 |
2011 |
2012 |
2013 |
2014 |
2015 |
2016 |
2017 |
|
No. of patients |
0 |
0 |
0 |
3 |
2 |
1 |
4 |
8 |
6 |
4 |
0 |
3 |
3 |
2. Age- and sex-based distribution
Of the 34 patients, 17 were men and 17 were women (sex ratio of 1:1) (Table 2). Among them, 14 patients (41.2%) were aged 50~69 years. Of the remaining patients, 6 (17.7%) patients were < 10 years old (Table 2). Our previous study showed that 41.3% of all the patients with T. verrucosum infection were aged < 15 years.
|
Age (y) |
Male (%) |
Female (%) |
Total (%) |
|
< 10 |
4
(11.8) |
2 (5.9) |
6 (17.7) |
|
10~19 |
3 (8.8) |
2 (5.9) |
5 (14.7) |
|
20~29 |
0 (0.0) |
1 (2.9) |
1 (2.9) |
|
30~39 |
3 (8.8) |
1 (2.9) |
4 (11.8) |
|
40~49 |
1 (2.9) |
2 (5.9) |
3 (8.8) |
|
50~59 |
1 (2.9) |
6
(17.6) |
7 (20.6) |
|
60~69 |
4
(11.8) |
3 (8.8) |
7 (20.6) |
|
70~79 |
1 (2.9) |
0 (0.0) |
1 (2.9) |
|
80~89 |
0 (0.0) |
0 (0.0) |
0 (0) |
|
≥
90 |
0 (0.0) |
0 (0.0) |
0 (0) |
|
Total (%) |
17 (50.0) |
17 (50.0) |
34 (100.0) |
3. Month and season-based distribution
Total 5 patients (14.7%) visited our hospital for the first time in September. Of the 34 patients, 10 each (29.4%) visited the hospital in spring, fall, or winter, representing the lowest incidence in summer (4, 11.8%) (Table 3).
|
Season |
Month |
No. of patients |
Total |
|
Spring |
Mar. |
2 (5.9) |
10 (29.4) |
|
Apr. |
4 (11.8) |
||
|
May. |
4 (11.8) |
||
|
Summer |
Jun. |
3 (8.8) |
4 (11.8) |
|
Jul. |
0 (0.0) |
||
|
Aug. |
1 (2.9) |
||
|
Fall |
Sep. |
5 (14.7) |
10 (29.4) |
|
Oct. |
3 (8.8) |
||
|
Nov. |
2 (5.9) |
||
|
Winter |
Dec. |
4 (11.8) |
10 (29.4) |
|
Jan. |
3 (8.8) |
||
|
Feb. |
3 (8.8) |
||
|
|
|||
4. Topographical distribution
The most common site for T. verrucosum infection was the arm. Of the 34 patients, 13 (38.2%) had an arm infection (Table 4). The face (9 cases, 26.5%) were the second most common site of infection, while the scalp, back, abdomen, and hip (each 2 cases, each 5.9%) were the third most common sites of infection, followed by the dorsal hand, neck, chest, and leg (each 1 case, each 2.9%) (Table 4). Our previous study reported that the face was the most commonly involved site. Dermatophytosis has several subtypes, depending on the infection site. Tinea corporis was the most common subtype of dermatophytosis caused by T. verrucosum, affecting 22 patients (64.7%) (Table 5). Tinea corporis was defined as dermatophytosis of the neck, chest, back, abdomen, upper and lower extremities, and hip. The second most common subtype was tinea faciei that was observed in 9 patients (26.5%). Tinea capitis was the third most common subtype, affecting 2 patients (5.9%), followed by tinea manus, affecting 1 patient (2.9%) (Table 5).
|
Infection site |
Number of patients |
Proportion (%) |
|
Dorsal hand |
1 |
2.9 |
|
Finger web |
0 |
0.0 |
|
Toe web |
0 |
0.0 |
|
Scalp |
2 |
5.9 |
|
Face |
9 |
26.5 |
|
Neck |
1 |
2.9 |
|
Chest |
1 |
2.9 |
|
Back |
2 |
5.9 |
|
Abdomen |
2 |
5.9 |
|
Arm |
13 |
38.2 |
|
Leg |
1 |
2.9 |
|
Hip |
2 |
5.9 |
|
Total |
34 |
100.0 |
|
Clinical type |
Number of patients |
Proportion (%) |
|
Tinea
faciei |
9 |
26.5 |
|
Tinea
capitis |
2 |
5.9 |
|
Tinea
corporis |
22 |
64.7 |
|
Tinea
manus |
1 |
2.9 |
|
Tinea
pedis |
0 |
0.0 |
|
Total |
34 |
100.0 |
5. Distribution as per the residential area
Of the 34 patients, 24 (70.6%) lived in rural areas, while 10 lived in urban areas.
T. verrucosum was first described by Sabouraud in 189316 and was named by Bodin in 190217. Folded, heaped, glabrous, and white colonies are observed in the fungal culture. The fungus grows slowly at room temperature, showing distinct chains of chlamydoconidia in the potassium hydroxide test18. Wood lamp examination shows positive results in infected cattle and negative results in infected humans. In human infections, positive results are observed only at the early stage of the infection19.
In cattle, T. verrucosum infection is often observed on the face, periocular area, and scalp as thick scales and hair loss patches. In humans, the infection presents as diffuse inflammation and confluent erythematous annular plaques with severe discharge and kerion celsi. Although T. verrucosum infection is known to be transmitted to humans via contact with infected cattle, there is no definite factor in the infection process that makes it spread12. In Korea, T. verrucosum was isolated from cattle infected with tinea in 1977 and 197820. In 1986, human infection was first reported in cattle-farming facilities in Jeon-nam area11. From 1962 to 1974, Korea had imported cattle from countries, such as North America. We believe that T. verrucosum strains in Korea may have entered from countries endemic for this infection. The spreading pathway of T. verrucosum in Japan may be similar to that in Korea21.
Since 1986, the prevalence of T. verrucosum infection had been increasing until 200022. Thereafter, the prevalence has progressively decreased owing to increased awareness regarding the mode of transmission (direct contact with infected cattle) and improved cattle-farming facilities22. This study showed a very low incidence of T. verrucosum infection.
As per our knowledge, susceptibility to T. verrucosum infection is independent of sex and age. Our study also showed similar results with respect to the sex-based distribution. However, age distribution showed a higher incidence of T. verrucosum infection among subjects in their fifties and sixties. Our previous study showed that the highest prevalence of T. verrucosum infection was among those aged < 10 years22. Good health care may be a major reason for the reduction in the prevalence of T. verrucosum infection among children. Takahashi et al.23 reported a female to male ratio of 1.3:1. George et al.24 reported that T. verrucosum infection was often transmitted within families via contact of contaminated clothes.
The occurrence of T. verrucosum infection is reportedly common in winter and spring, that is, from October to June. In this study, 20 patients (58.8%) were infected during winter or spring, that is, from December to May. The seasonal distribution of T. verrucosum is different from that of T. rubrum. T. rubrum infection is most commonly observed during summer25. The incidence of T. verrucosum infection correlates with that in cattle. Takahashi et al.23 reported 40 cases in 41 patients from November to April. Aoyagi el al.26 reported 11 cases from December to March, while Kubo et al.27 reported 47 cases, resulting in a total of 58 cases from December to June.
Kubo et al.27 and George et al.24 reported that T. verrucosum infection mainly occurs on the exposed body parts, such as the face, scalp, and upper extremities. Our previous study also reported similar results22. However, we found that the upper extremities were the most common infection site. The higher incidence of T. verrucosum infection among those in their fifties and sixties may explain that the upper extremities were more commonly involved than the face.
T. rubrum infection was checked predominantly in urban areas25; however, T. verrucosum infection was checked in rural areas, because of the exposure to infected cattle. Treatment for T. verrucosum infection includes the administration of oral antifungal agents, such as terbinafine, fluconazole, and griseofulvin, and some topical agents. However, treatment with topical agents alone may require more time and may have lower rates of patient compliance, making it less effective28.
As observed in the present study, the incidence of T. verrucosum infection has changed considerably over the previous 40 years. The gradual decrease in the annual incidence of T. verrucosum infections was prominent from 2000 to 2017. The common causes of dermatophytosis in Korea have been changing owing to increasing public health education and lifestyle diversity. T. verrucosum infection has almost disappeared from Korea; however, there is a possibility of its reappearance. Therefore, public awareness and continuous observation for this organism and infection are crucial. We believe that this study will help dermatologists obtain advanced information regarding the epidemiologic changes with respect to T. verrucosum in Korea.
In relation to this article, We declare that there is no conflict of interest.
References
1. Havlickova B, Czaika VA, Friedrich M. Epidemiological trends in skin mycoses worldwide. Mycoses 2008;51 Suppl 4:2-15
Crossref
Google Scholar
PubMed
2. Kim HS. The statistical and mycological survey on superficial dermatomycoses. Korean J Dermatol 1971;9:1-4
Crossref
Google Scholar
3. Rhim KJ, Kim JH, Shin S. A clinical and mycological study of superficial dermatophytoses. Korean J Dermatol 1978; 11:139-150
Crossref
Google Scholar
4. Min BK, Chung BS, Choi KC, Kim HK. Clinical and mycological studies on dermatophytosis. Korean J Dermatol 1984;22:604-609
Crossref
Google Scholar
5. Lee HK, Seo SJ, Kim MN, Hong CK, Ro BI. A clinical and mycological study of superficial fungal diseases (VII). Korean J Dermatol 1993;31:559-566
Crossref
Google Scholar
6. Moon HJ, Lee JB, Kim SJ, Lee SC, Won YH. Clinical and mycological studies on dermatomycosis. Korean J Med Mycol 2002;7:78-85
Crossref
Google Scholar
7. Lee DK, Moon KC, Koh JK. Clinical and mycological studies on superficial fungal infection. Korean J Med Mycol 2006; 11:54-63
Crossref
Google Scholar
8. Lee YW, Yun SJ, Lee JB, Kim SJ, Lee SC, Won YH. Clinical and mycological studies on dermatomycosis (2001~2010). Korean J Med Mycol 2013;18:30-38
Crossref
Google Scholar
9. Agnetti F, Righi C, Scoccia E, Felici A, Crotti S, Moretta I, et al. Trichophyton verrucosum infection in cattle farms of Umbria (Central Italy) and transmission to humans. Mycoses 2014;57:400-405
Crossref
Google Scholar
10. Korman T, Fuller A, Dowling J. Inflammatory tinea corporis due to Trichophyton verrucosum. Clin Infect Dis 1998;26: 220-221
Crossref
Google Scholar
PubMed
11. Kim YP, Chun IK, Kim SH. A case of kerion celsi caused by Trichophyton verrucosum and its epidemiologic study. Korean J Dermatol 1986;24:687-691
Crossref
Google Scholar
12. Kim HS, Choi JS, Kim KH. A case of kerion celsi caused by Trichophyton verrucosum. Korean J Dermatol 1987;27: 73-78
Crossref
Google Scholar
13. Kim YD, Park ES, Lee KS, Song JY. Tinea corporis occurring in one family caused by Trichophyton verrucosum. Korean J Dermatol 1989;27:435-439
Crossref
Google Scholar
14. Oh SH, Kim SH, Suh SB. Tinea capitis of adults in Taegu city for 11 years (1978~1988). Korean J Dermatol 1989; 27:666-679
Crossref
Google Scholar
15. Kim YP, Chun IK, Kim SH. A case of kerion celsi caused by Trichophyton verrucosum and treated with itraconazle. Korean J Dermatol 1994;32:124-129
Crossref
Google Scholar
16. Sabouraud R. Contribution a 1' etude de la trichophytie humaine. Ann Dermatol Syphiol 1893;4:814-835
Crossref
17. Bodin E. Trichophyton verrucosum. In Les champignons parasites de 1' home, pp 121. Paris, Masson et Cie, 1902
Crossref
18. Kim JC, Choi JS, Kim KH, Suh SB. Mycological features of Trichophyton verrucosum isolated in Taegu area. Korean J Dermatol 1992;30:761-768
Crossref
Google Scholar
19. Rippon JW. The pathogenic fungi and the pathogenic actinomycetes. Medical Mycology. 3rd ed. Philadelphia: WB Saunders, 1989:259-260
Crossref
20. Kim JC, Choi JS, Kim KH, Suh SB. Studies on dermatophytosis of Korean cattle. Korean J Vet Res 1979;19:149 -152
Crossref
Google Scholar
21. Murakami T, Kato H, Shinozaki K. Ueber eine Pilzzuechtung aus Trichophytie des Rindes. J Fac Agric 1955;2:143-147
Crossref
22. Choe YS, Park BC, Lee WJ, Jun JB, Suh SB, Bang YJ. The clinical observation of Trichophyton verrucosum infections during the last 19 years (1986~2004). Korean J Med Mycol 2006;11:45-53
Crossref
Google Scholar
23. Takahashi S, Makino Y, Fukushi G. Epidemiology and clinical observations of inflammatory ringworm due to Trichophyton verrucosum: epidemic in Tono area of Iwate prefecture and two sibling cases of kerion celsi. Jpn J Clin Dermatol 1971;25:427-442
Crossref
Google Scholar
24. Georg LK, Hand EA, Menges RA. Observations on rural and urban ringworm. J Invest Dermatol 1956;27:335-353
Crossref
PubMed
25. Lee WJ, Kim SL, Jang YH, Lee SJ, Kim DW, Bang YJ, et al. Increasing prevalence of Trichophyton rubrum identified through an analysis of 115,846 cases over the last 37 years. J Korean Med Sci 2015;30:639-643
Crossref
Google Scholar
26. Aoyagi T, Hirayama T, Miura Y. Endemy of Trichophyton verrucosum infection in human and cow. Jpn J Clin Dematol 1972;26:15-21
Crossref
27. Kubo H, Tamura T, Iizuka H, Shibaki H, Udawa S. Isolation of keratinophilic fungi from hair of wild fox (Vulpes vulpes schrenckii) and soil from affected areas in Hokkaido prefecture of Japan. Jpn J Med Mycol 1990;31:317-724
Crossref
Google Scholar
28. O'Gorman SM, Britton D, Collins P. An uncommon dermatophyte infection: two cases of cutaneous infection with Trichophyton verrucosum. Clin Exp Dermatol 2015; 40:395-398
Crossref
Google Scholar
Congratulatory MessageClick here!
