pISSN : 3058-423X eISSN: 3058-4302
Open Access, Peer-reviewed
pISSN : 3058-423X eISSN: 3058-4302
Open Access, Peer-reviewed

Ji Ha Yoon,Min Kyun An,Eun Joo Park,Kwang Ho Kim,Kwang Joong Kim
10.17966/JMI.2019.24.3.85 Epub 2019 October 02
Abstract
Fungal melanonychia is typically associated with onychomycosis and is known to be a relatively uncommon nail disorder. The known pathogens causing fungal melanonychia include both dematiaceous and non-dematiaceous fungi. Here we describe the case of a 60-year-old man with a 1-year history of nail discoloration in both index fingers. The possibility of subungual neoplasm was excluded by histological examination. Subsequent mycological examination revealed the presence of Cladosporium species in the lesion. The patient was successfully treated with oral itraconazole.
Keywords
Cladosporium Fungal melanonychia Melanonychia
Onychomycosis is defined as an infection of the nails by fungal organisms, including by dermatophyte and nondermatophyte mold and yeast. Melanonychia is usually detected by a brown or black pigmentation of the nail plate. Fungal melanonychia refers to melanonychia associated with onychomycosis and is a relatively rare nail disorder1. However, an increasing number of patients are being diagnosed with this condition recently, and it is expected that a higher number of causative species may be identified in the future2. Here we present a case of fungal melanonychia caused by Cladosporium.
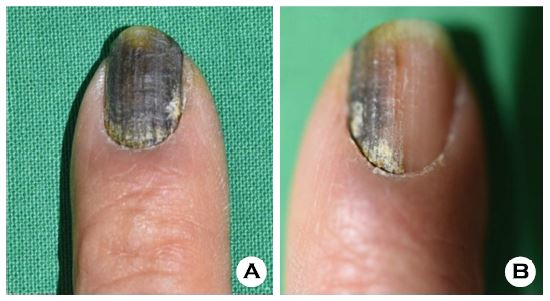
A 60-year-old man presented with a 1-year history of nail discoloration in both index fingers. The left nail showed a heterogeneous brown-to-black color change with some yellowish feature at the distal part of the nail (Figure 1A). The right nail showed discoloration in only half of the nail (Figure 1B). He had no other subjective symptoms, such as pain or pruritus. He had been receiving medication for hypertension, with no noted recent medication changes. Laboratory findings were within the normal limits, except for a mild increase in hepatic enzyme levels (aspartate aminotransferase and alanine aminotransferase). No abnormal findings were noted on the serological study.
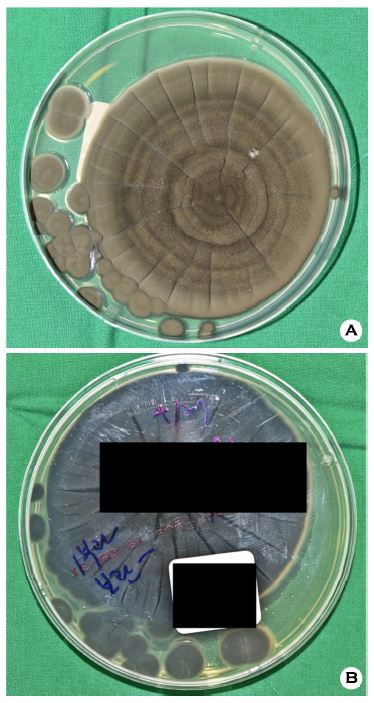
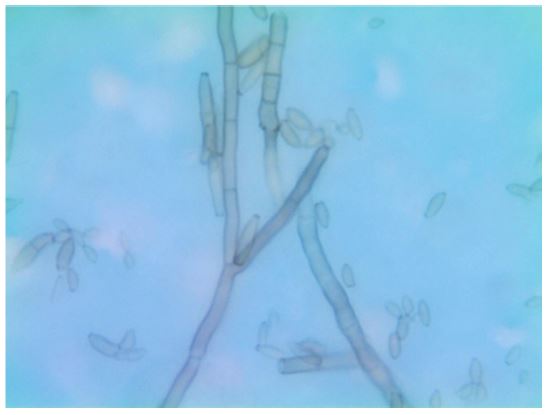
To confirm the cause of the pigmentation, we performed a nail biopsy and a mycological study. On biopsy, lichenoid lymphocytic infiltration was noted in the nail matrix, but there was no increase in the melanocytic activity of the skin. Therefore, we considered that the discoloration was not due to a change in melanin pigmentation in the nail bed, matrix, or plate. The mycological study included a KOH test and culture with samples collected directly from the involved nail plate. Sabouraud dextrose agar was used for this purpose. No definite hyphae were observed using the KOH test. However, in the cultures, black-to-brown fungal colonies were observed with a velvet-like surface (Figure 2A, B). Microscopic examination using typical adhesive tape preparation with lactophenol revealed the presence of dark pigmented septate hyphae and dark brown conidiophores. The typical chains of oval-shaped conidia were observed (Figure 3). Subsequently, RNA sequence analyses of the ITS1 and ITS2 regions were performed, and the results were assessed using the BLAST program. Results indicated a high similarity with Cladosporium species. Based on these results, we made a diagnosis of fungal melanonychia caused by Cladosporium. The patient was subsequently treated with 200 mg daily itraconazole and topical efinaconazole for 3 months.
Within the first month after the start of treatment, normal nail growth started to develop. At the end of the 3-month treatment, the patient exhibited normal nail growth, with some noted nail dystrophy associated with the earlier biopsy (Figure 4). No sign of relapse was observed in the 6 months of follow-up. Consent for publication of this case report was obtained from the patient.

Fungal melanonychia, also known as pigmented onychomycosis, is a relatively uncommon nail disorder caused by fungi that produce the melanin pigment, which are therefore referred to as "dematiaceous" fungi1. However, melanonychia can also be caused by other nondematiaceous fungi, including Trichophyton rubrum3, Aspergillus niger4, and Candida species5. The term "phaeohyphomycosis" is used to describe an infection caused by dematiaceous fungi, and fungal melanonychia is considered to be a form of superficial phaeohyphomycosis. Deep phaeohyphomycosis, which affects deep tissues, such as subcutaneous tissues, usually occurs in immunocompromised patients, but superficial phaeohyphomycosis can occur in healthy individuals2.
Cladosporium species are common fungi that can be found both indoors and outdoors. However, they are rarely considered as human pathogens. They can however cause allergic reactions, such as those in allergic asthma. In a literature search, two previous case reports of fungal melanonychia associated with Cladosporium species were found (Cladosporium carrionii6 and Cladosporium sphaerospermum7). Barde et al. reported a case of fungal melanonychia caused by Cladosporium carrionii6 in a 36-year-old man with no specific medical history who presented with onychomycosis. Their mycological study determined the genus of the fungus, but no report on the response to treatment was outlined. Onychomycosis caused by Cladosporium species could also occur without melanonychia. Shi et al. reported a case of onychomycosis associated with Cladosporium cladosporioides infection8. In their study, the patient presented with nail dystrophy and a periungual abscess and was successfully treated with oral itraconazole.
Limitations to our case study included the lack of serial culture testing for the presence of fungus. As Cladosporium species are present in the environment, there is also a possibility that culture contamination could have occurred. However, taking into consideration the patient's nail discoloration and the melanocytic property of Cladosporium species, our conclusion that pigmentation was due to fungal melanin was the most likely one. Additionally, the patient showed a good response to the concurrent topical and systemic antifungal medication. As fungal melanonychia is of relatively low incidence, there are no large randomized control studies for its treatment, and its management is based primarily on personal experience or case reports. Further research should be performed to assess the detailed clinical properties of fungal melanonychia associated with Cladosporium species.
The patient provided written informed consent for the publication and the use of his or her images.
References
1. Lee SW, Kim YC, Kim DK, Yoon TY, Park HJ, Cinn YW. Fungal melanonychia. J Dermatol 2004;31:904-909
2. Finch J, Arenas R, Baran R. Fungal melanonychia. J Am Acad Dermatol 2012;66:830-841
3. Perrin C, Baran R. Longitudinal melanonychia caused by Trichophyton rubrum: histochemical and ultrastructural studies of two cases. J Am Acad Dermatol 1994;31:311-316
Google Scholar
4. Tosti A, Piraccini BM, Lorenzi S. Onychomycosis caused by nondermatophytic molds: clinical features and response to treatment of 59 cases. J Am Acad Dermatol 2000; 42:217-224
Google Scholar
5. Parlak AH, Goksugur N, Karabay O. A case of melanonychia due to Candida albicans. Clin Exp Dermatol 2006;31:398-400
Google Scholar
6. Barde AK, Singh SM. Cladosporium carrionii Trejos 1954 infection of human nail. Mykosen 1984;27:366-369
Google Scholar
7. Male O, Trappeiner J. Nagelveranderungen durch Schimmelpilze. Dermatologische Wochenschrift 1965; 151:212-221
8. Shi D, Lu G, Mei H, Shen Y, Qiu Y, Liu W. A rare case of onychomycosis induced by Cladosporium cladosporioides. Open J Clin Med Case Rep 2016;2:1072
Congratulatory MessageClick here!
