pISSN : 3058-423X eISSN: 3058-4302
Open Access, Peer-reviewed
pISSN : 3058-423X eISSN: 3058-4302
Open Access, Peer-reviewed

Se Uk Oh,Ji Hun Park,Se Kwang Park,Joung Soo Kim ,Hyun-Min Seo
0.17966/JMI.2021.26.2.48 Epub 2021 July 01
Abstract
Keywords
Flap site Stenotrophomonas maltophilia
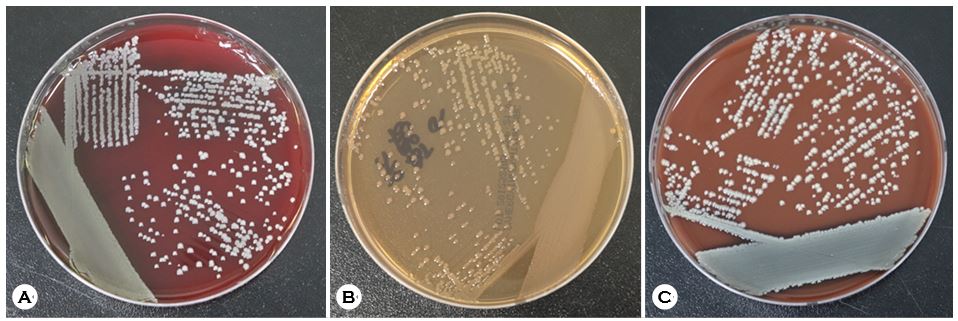
Stenotrophomonas maltophilia is a multidrug-resistant gram-negative bacillus frequently isolated from soil, water, animals, and plant matter. It forms colonies with an olive-green center and a lighter green peripheral area surrounded by a blue-green halo. S. maltophilia is associated with op- portunistic infections with high morbidity and mortality in immunocompromised individuals. Intensive care unit admission, mechanical ventilation, central venous catheter, recent surgery, trauma, previous therapy with extensive antibiotics, malignancy, and neutropenia are risk factors associated with S. maltophilia infection. Common infections include hospital-acquired pneumonia and bacteremia. However, S. maltophilia skin infections are extremely rare. Because of a recent increase in its incidence, an accurate understanding of this disease entity is necessary.
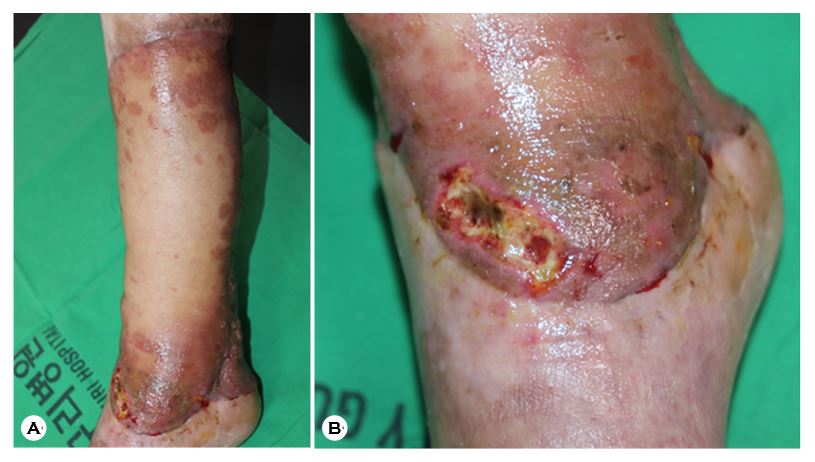
A 68-year-old man presented with a 1-week history of localized erosive erythematous patches with a blackish crust and secretions and scaly localized erythematous annular patches on the right lower leg (Fig. 1). He was diagnosed with squamous cell carcinoma on his right lower leg and had undergone wide excision and placement of a free flap 2 months before. A central venous catheter was placed before surgery and remained in place until 2 weeks after surgery. Levofloxacin and cefepime were administered for wound infection. Two months after surgery, he was referred to the dermatology department for skin lesions. The erosive patches were mainly distributed on the lower margin of the flap, whereas the scaly annular patches were on the upper and lateral margins. A KOH smear of the scaly erythematous annular patches was positive. Fungus and bacterial cultures were performed on the erythematous erosive patches. The fungus culture was negative, but Stenotrophomonas maltophilia was detected on blood, chocolate, and MacConkey agars (Fig. 2A-C). The patient was treated with oral trimethoprimsulfamethoxazole (80 mg/400 mg) twice a day because S. maltophilia was sensitive. Amorolfine cream was administered for fungal infection. The erosive lesions improved after a week of treatment.
In this patient, S. maltophilia and fungal infection coexisted on his leg, but their relationship seems low since they occurred in different places.
Skin presentations include primary cellulitis, metastatic nodular skin lesions or cellulitis, gangrenous cellulitis, soft tissue necrosis, ecthyma gangrenosum, and infected mucocutaneous ulcer. Treatment of S. maltophilia infections is difficult since this organism is intrinsically resistant to most antibiotics. It also grows slowly and has a high mutation rate, which results in antibiotic resistance. Its resistance to β-lactams, carbapenems, aminoglycosides, and quinolones is well known. Therefore, it is recommended to perform a susceptibility test before starting antibiotics. Because S. maltophilia can be isolated from nature, contamination or colonization can be suspected. However, single isolation of S. maltophilia implies infection rather than contamination or colonization. There were only five cases of skin and soft tissue infection with S. maltophilia in Korean dermatology literature. However, none occurred after surgery. To our knowledge, this is the first report of Stenotrophomonas maltophilia infection of a flap site in the Korean dermatology literature.
References
1. Apisarnthanarak A, Mayfield JL, Garison T, McLendon PM, DiPersio JF, Fraser VJ, et al. Risk factors for Stenotro- phomonas maltophilia bacteremia in oncology patients: a case-control study. Infect Control Host Epidemiol 2003; 24:269-274
Google Scholar
2. Adjidé CC, De Meyer A, Weyer M, Obin O, Lamory F, Lesueur C, et al. A sensitive, specific and predictive isolation medium developed for Stenotrophomonas maltophilia study in healthcare settings. Pathol Biol 2010;58:11-17
Google Scholar
3. Bin Abdulhak AA, Zimmerman V, Al Beirouti BT, Baddour LM, Tleyjeh IM. Stenotrophomonas maltophilia infections of intact skin: a systematic review of the literature. Diagn Microbiol Infect Dis 2009;63:330-333
Google Scholar
4. Kim MS, Kim CH, Won CH, Chang SE, Lee MW, Choi JH, et al. A case of metastatic cellulitis caused by Steno- trophomonas maltophilia. Korean J Dermatol 2009;47: 930-933
Google Scholar
5. Teo WY, Chan MY, Lam CM, Chong CY. Skin manifest- ation of Stenotrophomonas maltophilia infection-A case report and review article. Ann Acad Med Singap 2006; 35:897-900
Google Scholar
Congratulatory MessageClick here!
