pISSN : 3058-423X eISSN: 3058-4302
Open Access, Peer-reviewed
pISSN : 3058-423X eISSN: 3058-4302
Open Access, Peer-reviewed

Young-Min Han,Min Kyung Shin ,Hye-Jin Ahn
10.17966/JMI.2024.29.1.11 Epub 2024 March 28
Abstract
Individuals with frequent physical contact, such as wrestlers, are at an increased risk of developing infectious diseases, including bacterial, viral, and fungal infections. Herein, we report the case of a student wrestler who developed three common skin infections and a subsequent outbreak of methicillin-resistant Staphylococcus aureus (MRSA) skin infections in a single gym. A 14-year-old male presented with a 2-week history of an edematous, painful skin lesion on the left outer ear. He responded poorly to empirical antimicrobial therapy. Examination revealed multiple crusts and oozing on the left ear helix. A solitary, erythematous firm nodule was also observed on the left posterior neck. Bacterial culture confirmed MRSA resistance to clindamycin and tetracycline. Further assessment confirmed the diagnosis of herpes labialis and tinea faciei. Within 3 weeks, six additional cases of MRSA skin infections were reported, all linked to the same wrestling gym. Most patients were effectively treated with oral cephalosporins combined with topical fluoroquinolones and occlusive dressing.
Keywords
Herpes gladiatorum Methicillin-resistant Staphylococcus aureus Skin infections Tinea gladiatorum Wrestler
Skin-to-skin contact provides opportunities for the trans- mission of infections because bacteria, viruses, and fungi can spread from person to person. The most common species transmitted among wrestlers are Staphylococcus aureus, herpes simplex virus (HSV), and Trichophyton tonsurans1.
Methicillin-resistant S. aureus (MRSA) causes mild to severe skin and soft tissue infections. MRSA infections have increased and become prevalent as a causative strain of skin and sub- cutaneous tissue infections. A South Korean report revealed that more than half of S. aureus isolates from hospital tests were resistant to methicillin, and another study indicated that 18.1% of MRSA isolates were community-acquired2,3.
Community-acquired MRSA (CA-MRSA) infection has a different clinical profile than hospital-acquired MRSA (HA-MRSA) infection. Given that CA-MRSA infections often de- velop in immunocompetent individuals exposed to environ- ments with relatively high levels of physical contact, athletes, military personnel, and prisoners are at a high risk for this type of infection.
Herein, we report the case of a student wrestler who developed three common skin infections and a subsequent outbreak of MRSA skin infections in a single gym.
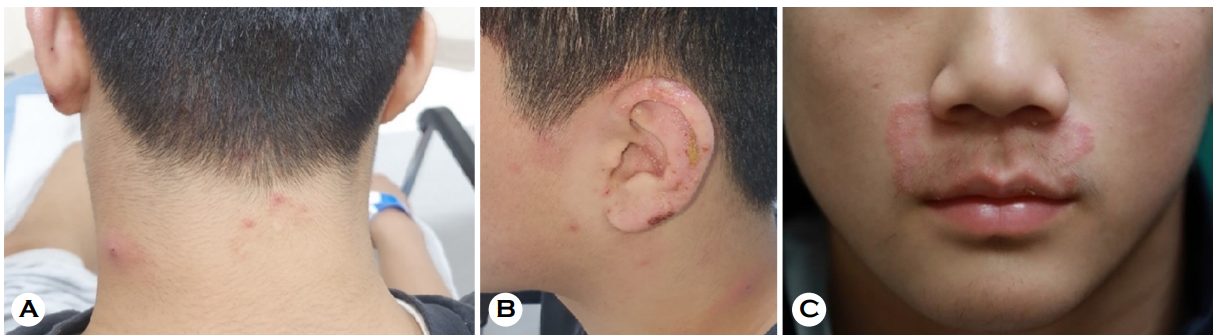
A 14-year-old male patient presented to the emergency department with an edematous skin lesion and pain in the left outer ear for 2 weeks. The patient had a fever of 37.8℃, and physical examination revealed multiple crusts and oozing on the left ear helix and a solitary, erythematous firm nodule on the left posterior neck (Figs. 1A and 1B). After being diag- nosed with cellulitis of the left arm at a primary care clinic, the patient had been taking cefaclor and applying mupirocin ointment for 2 months. However, his neck and ear lesions had not improved. In addition, the patient had a history of herpes zoster on the scalp approximately 2 months prior. The patient was a student wrestler, and some wrestlers in his gym exhibited similar skin symptoms. He received all man- datory vaccinations as scheduled and had no other underlying medical or drug history. Laboratory tests revealed elevated C-reactive protein levels and erythrocyte sedimentation rate and mild leukocytosis. Bacterial culture identified MRSA with resistance to clindamycin and tetracycline. Although the lesions initially improved with oral cefadroxil and topical ofloxacin, this improvement fluctuated within 2 months. After incision and drainage and switching to trimethoprim-sulfamethoxazole, all lesions resolved.
Other clinical symptoms were noted a week after the first visit. Vesicular lesions developed on the lips. Polymerase chain reaction assay of skin swab specimen detected HSV type 1, and famciclovir was added to the prescribed drugs. At the 1-month follow-up, an erythematous annular patch appeared on the philtrum (Fig. 1C), and fungal culture revealed T. tonsurans. The skin lesions resolved after 2 weeks of pulse therapy with itraconazole.
Six other patients presented to the outpatient clinic with cutaneous lesions within 3 weeks of the index case. Five of them were wrestlers in the same wrestling gym, and the remaining patient was the mother of the index case. A clinical photograph of one of the subsequent patients is shown in Fig. 2. According to the patients' statements, almost all 30 gym members developed similar dermatological symptoms within a month. The demographic and clinical features of the cases, including the index case, are summarized in Table 1. All patients showed insufficient responses to empiric anti- microbial therapy administered in primary care clinics. MRSA specimens with identical antimicrobial resistance profiles were isolated from bacterial cultures of skin lesions. The patients were instructed to thoroughly cover their lesions and avoid contact with others. All of them responded well to oral cephalosporins and topical fluoroquinolones.

|
Case |
Days after |
Age/ |
Skin lesion |
Type of |
Anatomical site |
Bacterial |
|
1 |
- |
14/M |
Erythematous nodule, |
Cellulitis |
Posterior neck, |
MRSA |
|
2 |
5 |
14/M |
Erythematous nodule |
Cellulitis |
Posterior neck, |
No growth |
|
3 |
6 |
17/M |
Crusted papules and nodules |
Impetigo |
Left shoulder |
MRSA |
|
4 |
9 |
14/M |
Erythematous ulcerated plaque |
Abscess |
Right posterior thigh |
MRSA |
|
5 |
11 |
15/M |
Erythematous nodule |
Impetigo |
Right shoulder |
MRSA |
|
6 |
12 |
14/M |
Erythematous papules |
Impetigo |
Left neck |
MRSA |
|
7 |
20 |
44/F |
Erythematous |
Abscess |
Right buttock |
MRSA |
CA-MRSA infections are a major problem among student athletes who participate in group training. Outbreaks have occurred in sports where physical contact is common, such as football, rugby, and wrestling. A study of high school and college athletes in the United States reported an incidence of 20.3 per 10,000 for CA-MRSA infection4. The rate was par- ticularly high among male gymnasts, rugby players, wrestlers, and soccer players. Nevertheless, outbreaks have also been reported in fencing, cross-country, and volleyball athletes without frequent physical contact, suggesting that contam- inated surfaces and environments may also contribute to the transmission of infections5.
In addition to bacterial skin infections, a nongenital cuta- neous HSV infection is commonly detected and transmitted in wrestlers. Referred to as herpes gladiator, this condition is predominantly caused by HSV type 1 and affects body areas that are in frequent contact with opponents during sports competitions. Among fungal infections, T. tonsurans has a widespread transmission. Named tinea gladiatorum, this infection may be transmitted via person-to-person contact. Other infectious diseases, such as varicella zoster virus infection, molluscum contagiosum, and verruca vulgaris, can also be transmitted among wrestlers1. The index patient had three common infections among wrestlers: MRSA skin infection, herpes gladiatorum, and tinea gladiator. However, no signs of transmission of viruses or fungi to other wrestlers were observed.
All the cases were epidemiologically relevant because all patients belonged to the same wrestling gym. Of the seven patients, six were young wrestlers aged between 14 and 17 years. The adult patient was the mother of the index case. MRSA was isolated in the bacterial cultures from six of the seven cases. All isolates had an identical antimicrobial sus- ceptibility profile.
The most affected anatomical site was the neck, followed by the shoulder. A possible explanation is that bare neck and shoulder contact is common during wrestling matches. According to a South Korean report, fungal infections of the head and neck area are common among wrestlers, with 1.7 times more infections recorded on the right side of the body than on the left6. This phenomenon is attributed to the relatively high number of right-handed wrestlers whose right body sides are often in contact during matches. However, no left or right bias was observed.
In our cases, the bacteria may have spread because of skin-to-skin contact and poor hygiene in the wrestling gym. Multiple interventions can be adopted to control infections among athletes. Proper education regarding personal hygiene and improved access to sanitizers can help prevent the spread of pathogens in the environment7.
The U.S. Center for Disease Control and Prevention pro- poses various strategies to prevent staphylococcal skin infec- tions and their transmission among athletes and emphasizes the importance of covering wounds, maintaining hygiene, and early recognition of infection.
Clindamycin and trimethoprim-sulfamethoxazole are re- commended as first-line empiric antibiotics for patients suspected of having CA-MRSA skin infections8. However, a Chinese study reported that most CA-MRSA strains are resistant to clindamycin and erythromycin9.
The resistance profiles of CA-MRSA differ from those of HA-MRSA. CA-MRSA demonstrates 94% susceptibility to ciprofloxacin, whereas HA-MRSA has only 14% susceptibility9. A Korean report recommended first-generation cephalo- sporins as the first-line treatment for suspected outpatient bacterial infections10.
The CA-MRSA strain identified in our cases was resistant to clindamycin. Oral cephalosporins combined with topical fluoroquinolones and occlusive dressing were effective in most of the patients except for the index case who responded to trimethoprim-sulfamethoxazole.
This case report describes a student wrestler diagnosed with three common skin infections confirmed by microbiological testing. The other six patients had an outbreak of MRSA skin infections linked to a single wrestling gym. Given that a gym can act as a site of pathogen transmission, regular disinfection of the gym and assessment of the players' skin lesions at an early stage are crucial to prevent the spread of infectious diseases.
References
1. Wilson EK, Deweber K, Berry JW, Wilckens JH. Cutaneous infections in wrestlers. Sports Health 2013;5:423-437
Google Scholar
2. Kim ES, Song JS, Lee HJ, Choe PG, Park KH, Cho JH, et al. A survey of community-associated methicillin-resistant Staphylococcus aureus in Korea. J Antimicrob Chemother 2007;60:1108-1114
Google Scholar
3. Sung JY, Lee J, Choi EH, Lee HJ. Changes in molecular epidemiology of community-associated and health care-associated methicillin-resistant Staphylococcus aureus in Korean children. Diagn Microbiol Infect Dis 2012;74:28-33
Google Scholar
4. Braun T, Kahanov L. Community-associated methicillin-resistant Staphylococcus aureus infection rates and man- agement among student-athletes. Med Sci Sports Exerc 2018;50:1802-1809
Google Scholar
5. Kirkland EB, Adams BB. Methicillin-resistant Staphylo- coccus aureus and athletes. J Am Acad Dermatol 2008; 59:494-502
Google Scholar
6. Jun JB, Kim YD. The Epidemiological, Clinical and mycol- ogical studies on trichophytosis gladiatorum prevailing among Korean wrestlers. Korean J Med Mycol 2004;9: 28-44
Google Scholar
7. LaBelle MW, Knapik DM, Arbogast JW, Zhou S, Bowersock L, Parker A, et al. Infection risk reduction program on pathogens in high school and collegiate athletic training rooms. Sports Health 2020;12:51-57
Google Scholar
8. Liu C, Bayer A, Cosgrove SE, Daum RS, Fridkin SK, Gorwitz RJ, et al. Clinical practice guidelines by the infectious dis- eases society of america for the treatment of methicillin-resistant Staphylococcus aureus infections in adults and children: executive summary. Clin Infect Dis 2011;52:285-292
Google Scholar
9. Peng H, Liu D, Ma Y, Gao W. Comparison of community- and healthcare-associated methicillin-resistant Staphylo- coccus aureus isolates at a Chinese tertiary hospital, 2012-2017. Sci Rep 2018;8:17916
Google Scholar
10. Lim JS, Park HS, Cho S, Yoon HS. Antibiotic susceptibility and treatment response in bacterial skin infection. Ann Dermatol 2018;30:186-191
Google Scholar
Congratulatory MessageClick here!
