pISSN : 3058-423X eISSN: 3058-4302
Open Access, Peer-reviewed
pISSN : 3058-423X eISSN: 3058-4302
Open Access, Peer-reviewed

Weon Ju Lee,Dong Hyuk Eun,Yong Hyun Jang,Yong Jun Bang,Jae Bok Jun
10.17966/JMI.2018.23.1.1 Epub 2018 April 01
Abstract
Background: Superficial fungal infections, including dermatophyte infection and cutaneous candidiasis, are common and affect more than 25% of the population worldwide.
Objective: The aim of this study was to investigate the recent clinical and mycological characteristics of dermatophytosis and cutaneous candidiasis in southeastern Korea.
Methods: Of 20,413 patients with dermatophyte infection, cutaneous candidiasis, or suspected fungal infection, 8,106 who were culture positive for infection were retrospectively evaluated using their medical records.
Results: The annual incidence rate of fungal infection tended to be constant. Such infections were more common in men than in women. Fungal infections most commonly occurred in patients in their 50s and in August. The most common clinical type of superficial fungal infections was tinea pedis. The most common causative fungus of superficial fungal infections was Trichophyton rubrum.
Conclusion: This study provides useful information on the clinical and mycological characteristics of fungal infections in southeastern Korea in recent years.
Keywords
Dermatophyte infection and cutaneous candidiasis are common and affect more than 25% of the population worldwide[1]. The main causative fungus of superficial mycoses has been changing dramatically in Korea[2]-[8]. Several factors such as socioeconomic status, lifestyle, and development of new antifungal drugs lead to changes in the main causative dermatophyte of superficial mycoses. Trichophyton (T.) rubrum is the most common causative agent of dermatophytosis in Korea since the 1960s[2]. T. mentagrophytes, Microsporum (M.) canis, T. verrucosum, M. gypseum, and T. tonsurans appeared as the main species of superficial mycoses in Korea during the past 100 years[9]-[18]. With the development of antifungal agents, an increasing number of patients have visited dermatologic clinics for appropriate treatment of dermatophytosis. However, only few recent domestic studies on fungal infections have been reported since 2013, while epidemiological studies are still being reported in various countries. The aim of this study was to investigate the clinical and mycological characteristics of dermatophytosis and cutaneous candidiasis in southeastern Korea in recent years.
1. Patients and methods
The medical records of 20,413 patients with dermatophyte infection or cutaneous candidiasis were retrospectively studied. The medical records were recorded at Kyungpook National University Hospital or the Catholic Skin Disease Clinic from 2013 to 2016. The patients were KOH- and/or culture positive. Most of the patients had lived in the southeastern area of South Korea.
The presence of dermatophytes and Candida was identified using KOH examination and fungal culture. Specimens for fungal examinations were obtained by scraping the lesions with a scalpel, and microscopic examination with 15% KOH solution was performed. Among the 20,413 patients, 13,441 (66%) were KOH positive. Diagnoses of dermatophyte and Candida infections were confirmed with fungal culture using potato cornmeal Tween 80 agar culture media. The culture media were kept at 24~26℃ for over 2 weeks. Dermatophytes and Candida on the culture media each showed a morphologically typical colony. Among the 20,413 patients, 8,106 (40%) were culture positive. The medical records of the culture-positive patients were used to evaluate the annual incidence and patient distribution according to sex, age, season, site, and causative fungus. Tinea pedis was designated as superficial fungal infection of the toe web, sole, and dorsum of the foot. Onychomycosis was defined as superficial fungal infection of the toenail and fingernail. Tinea corporis was designated as a superficial fungal infection of the neck, chest, back, abdomen, axilla, upper and lower extremities, and buttocks. Tinea manus was defined as a superficial fungal infection of the palm, finger web, and dorsum of the hand.
1. Annual incidence rates of dermatophyte and cutaneous Candida infections
The annual incidence rates of dermatophyte and cutaneous Candida infections were as follows: 2,029 in 2013, 1,841 in 2014, 1,799 in 2015, and 2,427 in 2016.
2. Distributions of dermatophyte and cutaneous Candida infections according to sex and age
Of 8,106 culture-positive patients, 5,101 (62.9%) were men and 3,005 (37.1%) were women (Table 1). However, the group aged ≥70 years had more women than men (Table 1). The most common age group was the 50s group (1,875; 23.1%), followed by the 40s (1,689; 20.8%) and 30s groups (1,299; 16.0%; Table 1).
|
0~9 |
10~19
years |
20~29
years |
30~39
years |
40~49
years |
50~59
years |
60~69
years |
70~79
years |
≥80 |
Total |
|
|
Male |
110 |
251 |
584 |
948 |
1,113 |
1,135 |
638 |
258 |
64 |
5,101 (62.9%) |
|
Female |
55 |
94 |
191 |
351 |
576 |
740 |
487 |
368 |
143 |
3,005 |
|
Total |
165 |
345 |
775 |
1,299 |
1,689 |
1,875 |
1,125 |
626 |
207 |
8,106 |
3. Monthly distributions of dermatophyte and cutaneous Candida infections
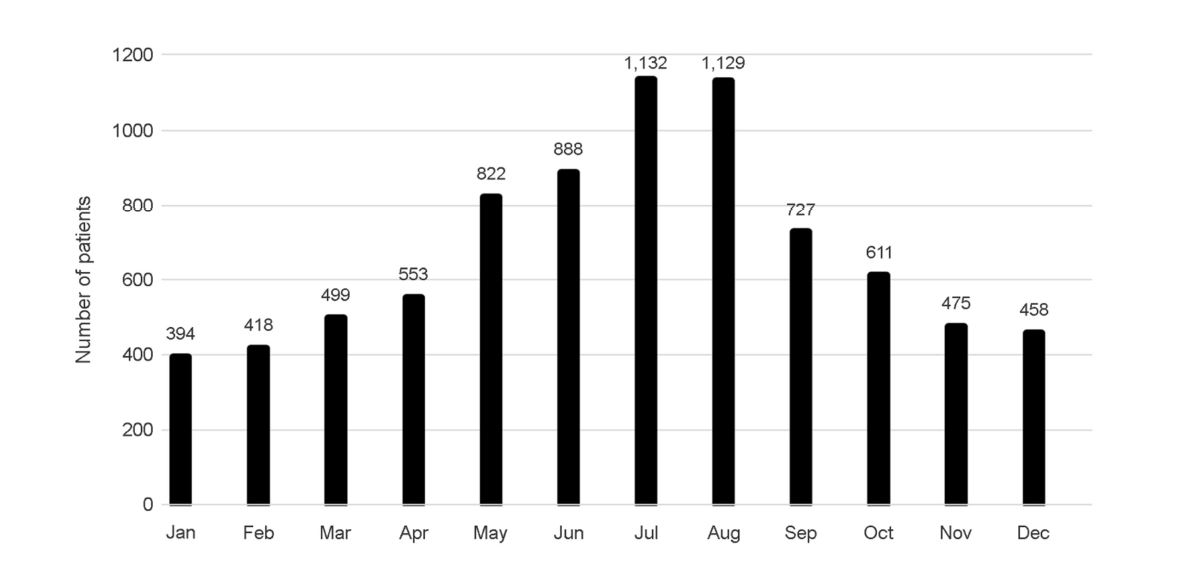
The incidence rates of dermatophyte and cutaneous Candida infections were highest in July, followed by August and June (Figure 1). Of 8,106 culture-positive patients, 1,132 (14.0%) were diagnosed in July, 1,129 (13.9%) in August, and 888 (11.0%) in June (Figure 1).
4. Topographical distributions of dermatophyte and cutaneous Candida infections
The most common clinical type of dermatophyte and cutaneous Candida infections was tinea pedis (3,898; 48.1%), followed by tinea unguium (2,389; 29.5%) and tinea cruris (1,057; 13.0%) (Table 2). Tinea capitis was more common in women than in men (Table 2). In addition, tinea capitis was most common at the age of ≤9 years, followed by the 70s and 80s and older (Table 3). Tinea cruris was less common in women than in men (Table 3).
|
Tinea |
Tinea |
Tinea |
Tinea |
Tinea |
Tinea |
Tinea |
Other |
|
|
Male |
106 |
2,556 |
1,329 |
14 |
90 |
169 |
820 |
17 |
|
Female |
60 |
1,342 |
1,060 |
34 |
61 |
185 |
237 |
26 |
|
Total |
166 |
3,898 |
2,389 |
48 |
151 |
354 |
1,057 |
43 |
|
Age, |
Tinea |
Tinea |
Tinea |
Tinea |
Tinea |
Tinea |
Tinea |
Other |
|
0~9 |
6 |
84 |
8 |
21 |
16 |
16 |
12 |
2 |
|
10~19 |
5 |
176 |
19 |
6 |
10 |
45 |
84 |
0 |
|
20~29 |
10 |
424 |
146 |
1 |
9 |
43 |
139 |
3 |
|
30~39 |
18 |
787 |
285 |
1 |
11 |
39 |
157 |
1 |
|
40~49 |
38 |
911 |
490 |
1 |
16 |
44 |
186 |
3 |
|
50~59 |
31 |
856 |
671 |
1 |
35 |
58 |
214 |
9 |
|
60~69 |
36 |
426 |
436 |
2 |
26 |
46 |
151 |
2 |
|
70~79 |
16 |
189 |
256 |
8 |
20 |
35 |
88 |
14 |
|
80~89 |
6 |
45 |
78 |
7 |
8 |
28 |
26 |
9 |
|
Total |
166 |
3,898 |
2,389 |
48 |
151 |
354 |
1,057 |
43 |
5. Distribution of causative fungi
The most common fungal strain was T. rubrum (7,332; 90.4%), followed by T. mentagrophytes (325; 4.0%) and Candida albicans (307; 3.8%) (Table 4). Most fungal infections, including T. rubrum infection, were more common in men, while M. canis infection was more common in women (Table 4). T. tonsurans infection only occurred in the 10s and 20s age groups. M. canis infection was most common in the ≤9-year age group. C. albicans infection was more common in the elderly group, including the 50s, 60s, and 70s age groups (Table 5). Most fungal infections were more in summer, but M. canis and T. tonsurans infections did not show monthly preponderance (Table 6). T. rubrum and T. mentagrophytes infections were the major causes of tinea pedis (Table 7). M. canis and T. tonsurans infections usually caused tinea faciei, tinea corporis, and tinea capitis (Table 7). C. albicans infection was the major cause of tine pedis, tinea corporis, and tinea unguium (Table 7).
|
|
T. rubrum |
T. mentagrophytes |
T. verrucosum |
T. tonsurans |
M. canis |
M. gypseum |
E. floccosum |
C. albicans |
|
Male |
4,706 |
194 |
1 |
14 |
25 |
4 |
7 |
151 |
|
Female |
2,626 |
131 |
3 |
3 |
82 |
3 |
0 |
156 |
|
Total |
7,332 |
325 |
4 |
17 |
107 |
7 |
7 |
307 |
|
Age, years |
T. rubrum |
T. mentagrophytes |
T. verrucosum |
T. tonsurans |
M. canis |
M. gypseum |
E. floccosum |
C. albicans |
|
0~9 |
119 |
9 |
1 |
0 |
27 |
1 |
0 |
8 |
|
10~19 |
295 |
9 |
0 |
14 |
22 |
0 |
0 |
5 |
|
20~29 |
700 |
38 |
0 |
3 |
16 |
0 |
2 |
16 |
|
30~39 |
1,199 |
57 |
2 |
0 |
13 |
2 |
0 |
26 |
|
40~49 |
1,565 |
79 |
0 |
0 |
4 |
2 |
1 |
38 |
|
50~59 |
1,713 |
70 |
0 |
0 |
5 |
0 |
3 |
84 |
|
60~69 |
1,013 |
40 |
1 |
0 |
6 |
1 |
1 |
63 |
|
70~79 |
550 |
17 |
0 |
0 |
11 |
0 |
0 |
48 |
|
≥80 |
178 |
6 |
0 |
0 |
3 |
1 |
0 |
19 |
|
Total |
7,332 |
325 |
4 |
17 |
107 |
7 |
7 |
307 |
|
|
T. rubrum |
T. mentagrophytes |
T. verrucosum |
T. tonsurans |
M. canis |
M. gypseum |
E. floccosum |
C. albicans |
|
Jan |
355 |
15 |
1 |
2 |
10 |
0 |
0 |
11 |
|
Feb |
383 |
11 |
0 |
2 |
2 |
2 |
0 |
18 |
|
Mar |
454 |
22 |
0 |
0 |
7 |
0 |
0 |
16 |
|
Apr |
487 |
28 |
0 |
6 |
7 |
0 |
0 |
25 |
|
May |
737 |
48 |
0 |
1 |
12 |
0 |
2 |
22 |
|
Jun |
819 |
33 |
2 |
1 |
8 |
2 |
2 |
21 |
|
Jul |
1,034 |
53 |
0 |
0 |
4 |
2 |
2 |
37 |
|
Aug |
1,023 |
39 |
0 |
0 |
15 |
0 |
0 |
52 |
|
Sep |
653 |
30 |
1 |
1 |
9 |
0 |
0 |
33 |
|
Oct |
551 |
16 |
0 |
0 |
9 |
0 |
0 |
35 |
|
Nov |
424 |
15 |
0 |
3 |
12 |
1 |
0 |
20 |
|
Dec |
412 |
15 |
0 |
1 |
12 |
0 |
1 |
17 |
|
Total |
7,332 |
325 |
4 |
17 |
107 |
7 |
7 |
307 |
|
T. rubrum |
T. mentagrophytes |
T. verrucosum |
T. tonsurans |
M. canis |
M. gypseum |
E. floccosum |
C. albicans |
|
|
Tinea manus |
145 |
5 |
0 |
0 |
2 |
0 |
0 |
14 |
|
Tinea pedis |
3,569 |
209 |
0 |
0 |
1 |
2 |
4 |
113 |
|
Tinea |
2,254 |
79 |
0 |
1 |
0 |
3 |
2 |
50 |
|
Tinea capitis |
13 |
0 |
0 |
3 |
32 |
0 |
0 |
0 |
|
Tinea faciei |
117 |
9 |
2 |
4 |
18 |
0 |
0 |
1 |
|
Tinea corporis |
259 |
16 |
1 |
9 |
53 |
2 |
0 |
14 |
|
Tinea cruris |
973 |
6 |
1 |
0 |
1 |
0 |
1 |
75 |
|
Others |
2 |
1 |
0 |
0 |
0 |
0 |
0 |
40 |
|
Total |
7,332 |
325 |
4 |
17 |
107 |
7 |
7 |
307 |
The incidence of fungal infection is influenced by lifestyle, hygiene, and accessibility to hospitals. Despite the recent economic developments, the incidence of fungal infection in Korea has been increasing. Fungal infection is generally known to affect more than 25% of the population worldwide[1]. This study showed a steady incidence in recent years.
In Korea, dermatophytosis was most common in young adults in the past but in middle-aged adults in recent years. This study also showed that fungal infection was more common in middle-aged individuals. Unusually, fungal infections caused by M. canis and T. tonsurans developed in young children, like in this study[19],[20]. Unlike previous reports, this study demonstrated that M. gypseum infection did not show preponderance in young children[19]. However, because the incidence of M. gypseum infection was low, we could not draw a definite conclusion. The ratio of men in this study was greater than that in previous reports. In addition, the ≥70-year age group had more women than men.
Superficial fungal infections usually develop in summer because dermatophyte infection of the human skin is accelerated by a hot and humid weather. However, some studies showed that M. canis infection had greater incidences in winter than in any other season[19]. T. tonsurans infection was also found to occur more commonly in spring[20]. In this study, the seasonal incidences of M. canis infection and T. tonsurans infections did not show the same patterns as those reported in previous studies.
The most common clinical type of superficial fungal infections was tinea pedis. Tinea pedis is a common dermatophyte infection. Moreover, the incidence of tinea pedis has increased in low socioeconomic countries[21]. In this study, we found that tinea cruris occurred less frequently in women than in men. Macura reported that tinea cruris is commonly found in men living in warm climates[22]. Tinea cruris can coexist with tinea pedis because dermatophytes spread from the feet to the groin by scratching. Therefore, tinea cruris was the third most common clinical type of dermatophytosis.
The causative species of fungal infections has considerable variability. T. rubrum was reported to be a major cause of fungal infections in Europe, whereas T. mentagrophytes infection is more common in Asia[1]. T. rubrum has also been considered the most common causative agent of dermatophytosis in Korea since the 1960s[2]. Lee et al. reported that 88.35% of patients in Korea had T. rubrum infection[23]. This study also showed that the most common dermatophyte was T. rubrum. T. rubrum infection was more common in men, while M. canis infection was more common in women. In addition, the predominant species of dermatophytes vary with the clinical type of dermatophytosis. Tinea pedis is usually caused by T. rubrum, T. interdigitale, and Epidermophyton (E.) floccosum. In our study, the major causative agents of tinea pedis were T. rubrum and T. mentagrophytes. In addition, C. albicans was one of the major causes of tinea pedis. Tinea pedis caused by T. rubrum seems to be related to exercise, outdoor activity, obesity, diabetes mellitus, and increasing age. Conversely, M. canis and T. tonsurans usually cause tinea faciei, tinea corporis, and tinea capitis as reported in the literature. Infections caused by M. canis could be related to the close contact between humans and contaminated animals. Infection caused by T. tonsurans could be associated with frequent international sports activities. Contrary to previous reports, E. floccosum was not found as a causative agent of fungal infections. Kim et al. reported that the incidence of E. floccosum infection had rapidly decreased in Korea since 1990[24].
Fungal infections still exist worldwide. Therefore, we should have awareness on fungal infections. Our results are not significantly different from the previous data but are meaningful in that they show the recent trend of fungal infection, including cutaneous candidiasis. This study provides useful information on the recent clinical and mycological characteristics of fungal infections in the southeastern area of Korea.
References
1. Havlickova B, Czaika VA, Friedrich M. Epidemiological trends in skin mycoses worldwide. Mycoses 2008;51:2-15
Crossref
Google Scholar
PubMed
2. Kim HS. The statistical and mycological survey on superficial dermatomycoses. Korean J Dermatol 1971;9:1-4
Crossref
Google Scholar
3. Rhim KJ, Kim JH, Shin S. A clinical and mycological study of superficial dermatophytoses. Korean J Dermatol 1978; 16:435-442
Crossref
Google Scholar
4. Min BK, Chung BS, Choi KC, Kim HK. Clinical and mycol- ogical studies on dermatophytosis. Korean J Dermatol 1984;22:604-609
Crossref
Google Scholar
5. Lee HK, Seo SJ, Kim MN, Hong CK, Ro BI. A clinical and mycological study of superficial fungal diseases (vii) Korean J Dermatol 1993;31:559-566
Crossref
Google Scholar
6. Moon HJ, Lee JB, Kim SJ, Lee SC, Won YH. Clinical and mycological studies on dermatomycosis (1991-2000) Korean J Med Mycol 2002;7:78-85
Crossref
Google Scholar
7. Lee DK, Moon KC, Koh JK. Clinical and mycological studies on superficial fungal infection. Korean J Med Mycol 2006; 11:54-63
Crossref
Google Scholar
8. Lee YW, Yun SJ, Lee JB, Kim SJ, Lee SC, Won YH. Clinical and mycological studies on dermatomycosis (2001-2010) Korean J Med Mycol 2013;18:30-38
Crossref
Google Scholar
9. Kim BS, Suh SB. Mycological and clinical observation on dermatophytosis. Korean J Dermatol 1976;14:325-334
Crossref
Google Scholar
10. Suh SB, Kim SW, Oh SH, Choi SK, Bang YJ. A case of block dot ringworm caused by Trichophyton tonsurans. Korean J Dermatol 1998;36:918-923
Crossref
Google Scholar
11. Sung SY, Kim HY, Kim HU, Ihm CW. Trichophyton ton- surans infection in wrestlers and a child. Korean J Der- matol 1998;36:732-736
Crossref
Google Scholar
12. Kim JC, Choi JS, Kim KH, Suh SB. Mycological features of Trichophyton verrucosum isolated in Taegu area. Korean J Dermatol 1992;30:761-768
Crossref
Google Scholar
13. Kim YP, Chun IK, Kim SH. A case of kerion celsi caused by Trichophyton verrucosum and its epidemiologic study. Korean J Dermatol 1986;24:687-691
Crossref
Google Scholar
14. Jun JB, Suh SB. Clinical and mycological studies on Micro- sporum gypseum infection. Korean J Dermatol 1980;18: 369-381
Crossref
Google Scholar
15. Lee DS, Cho GY, Kim YH, Houh W. A case of tinea capitis due to Microsporum gypseum. Korean J Dermatol 1984;22:643-646
Crossref
Google Scholar
16. Lee H, Lee ES, Kang WH, Lee SN. An unusual clinical manifestation of tinea corporis caused by Microsporum ferrugineum. Korean J Dermatol 1987;25:383-388
Crossref
Google Scholar
17. Kim HU, Choi CJ, Yun SK. Three cases of tinea capitis caused by Microsporum ferrugineum. Korean J Dermatol 1993;31:760-764
Crossref
Google Scholar
18. Kim YA, Lee KH, Lee JB, Suh SB. A case of fungal gran- uloma caused by Trichophyton violaceum. Korean J Der- matol 1989;27:304-307
Crossref
Google Scholar
19. Lee WJ, Song CH, Lee SJ, Kim DW, Jun JB, Bang YJ. Decreasing prevalence of Microsporum canis infection in Korea: through analysis of 944 cases (1993-2009) and review of our previous data (1975-1992). Mycopathologia 2012;173:235-239
Crossref
Google Scholar
20. Lee WJ, Sim HB, Jang YH, Lee SJ, Kim DW, Jun JB, et al. Skin Infection due to Trichophyton tonsurans still occurs in people in Korea but not as outbreaks. J Korean Med Sci 2016;31:296-300
Crossref
Google Scholar
PubMed
21. Nenoff P, Herrmann J, Gräser Y. Trichophyton mentagro- phytes sive interdigitale? A dermatophyte in the course of time. JDDG 2007;5:198-202
Crossref
Google Scholar
PubMed
22. Macura AB. Dermatophyte infections. Int J Dermatol. 1993;32:313-323
Crossref
PubMed
23. Lee WJ, Kim SL, Jang YH, Lee SJ, Kim DW, Bang YJ. Increasing prevalence of Trichophyton rubrum identified through an analysis of 115,846 cases over the last 37 years. J Korean Med Sci 2015;30:639-643
Crossref
Google Scholar
24. Kim SL, Lee KC, Jang YH, Lee SJ, Kim DW, Lee WJ, et al. The epidemiology of dermatophyte infection in south- eastern Korea (1979-2013). Ann Dermatol 2016;28:524 -527
Crossref
Google Scholar
PubMed
Congratulatory MessageClick here!
