pISSN : 3058-423X eISSN: 3058-4302
Open Access, Peer-reviewed
pISSN : 3058-423X eISSN: 3058-4302
Open Access, Peer-reviewed

Dongyoung Roh,Hyojin Kim,Jae-Hui Nam,Je-Ho Mun,Joonsoo Park,Jin Park,Yang Won Lee,Jee-Bum Lee,Ji Hyun Lee,Jong Soo Choi,Hyun Chang Ko
10.17966/JMI.2018.23.1.15 Epub 2018 April 01
Abstract
Background: The prevalence of onychomycosis is increasing due to the recent increase of the elderly population and immunosuppressed individuals. Clinical studies on onychomycosis have been reported several times in Korea. However, the public awareness of onychomycosis has not received considerable attention, and there have been no Korean studies focused on it.
Objective: To evaluate public awareness and experience of onychomycosis in Korean.
Methods: A total of 621 participants were given questions developed for this survey. Sociodemographic characteristics, public awareness, general knowledge and experience about onychomycosis, and diagnostic and treatment behavior were surveyed.
Results: According to this survey, 99.5% of respondents have heard of onychomycosis, 79.4% of respondents experienced onychomycosis suspicious symptoms, and 52.8% of them responded that onychomycosis can be completely cured only by cleansing the hands and feet. The rate of self-diagnosis was 64.1% among the respondents who experienced symptoms. Only 23.9% of the respondents who were diagnosed with onychomycosis visited the hospital for the first time. Of the respondents, 54.6% who were treated at the hospital discontinued their treatments before complete cure mainly because of long treatment period.
Conclusion: Participants were well aware of onychomycosis, but the rate of self-diagnosis was high. They generally agreed to the importance of hospital treatment, but the number of patients visiting hospital was low. Moreover, people frequently discontinue their hospital treatment despite insufficient treatment duration. Patient's behaviors need to be changed, and the roles of dermatologists are important in the diagnosis, treatment, and education of the patients.
Keywords
Awareness Onychomycosis Tinea unguium
Onychomycosis is a chronic fungal nail infection from dermatophytes, nondermatophytic molds, or yeasts. It accounts for about 50% of all nail diseases and 30% of all cutaneous fungal infections[1]. The prevalence of onychomycosis in various populations has ranged from 2 to 14%[2]-[7]. Onychomycosis have been prevailing lately due to the recent increase of the elderly population and immunosuppressed individuals[8]. Further, increased exposure to various fungi after the use of ill-fitting shoes and public lockers in sport facilities is a contributing factor[8]. Studies on onychomycosis have been reported several times in Korea[9]-[19]. Recently, Yoo et al.[20] investigated the clinical and mycological features of onychomycosis in Korean elderly population. Moreover, the epidemiology of onychomycosis in Koreans had been studied by Hwang et al[10]. However, public awareness of onychomycosis has not received considerable attention, and there have been no Korean studies focused on it. The aim of this study was to evaluate public awareness of onychomycosis to emphasize the need for changes in patient's attitude toward onychomycosis and the importance of the role of dermatologists in diagnosis and treatment of onychomycosis.
1. Study population and study design
Eligible participants for this study were Korean men or women aged over 20 years with or without onychomycosis. The questionnaire developed for this survey by the investigators was implemented on the Internet via the Gallup Korea agency, and the data were collected online from 621 eligible subjects on June 2~7, 2017. The subjects were randomly selected on the internet as the same sex and age distribution of the Korean population. The subjects were informed that the questionnaire was anonymous and confidential.
2. Questionnaire
This questionnaire survey was developed through the Korean Society for Medical Mycology to investigate general awareness about onychomycosis. This questionnaire was composed of several parts: sociodemographic characteristics of the participants, public awareness, general knowledge and experience about onychomycosis, and diagnostic and treatment behavior of the participants. The survey included questions on age, sex, occupation, accompanying disease, and medication history. Public awareness, knowledge and experiences about onychomycosis were addressed with several questions, and participants were asked to choose phrases that they agree with, regardless of whether they were affected or not.
1. Sociodemographic characteristics
Male-to-female ratio was 1.02:1 with 313 (50.4%) men and 308 (49.6%) women. The age group revealed that the number of participants in their 40s was the largest (24.3%), followed by those in their 50s (23.2%), 30s (19.6%), 20s (18.7%), and over 60s (14.2%). Regarding the occupations of the respondents, white-collar occupation was the most common (50.9%), followed by housewife, student, and unemployed (31.1%), self-employed (9.5%), and blue-collar occupation (8.5%).
2. Public awareness and understanding of onychomycosis
The data of public awareness of onychomycosis are summarized in Table 1. Of the participants, 88.1% responded that they have heard about onychomycosis and know what it is, 11.9% responded that they do not know about onychomycosis, and 0.5% said they have never heard of it. Of the participants, 52.8% agreed that onychomycosis can be completely cured with just clear hand and foot washing, 38.6% responded that onychomycosis causes only a cosmetic problem, not a health problem, 56.8% answered that it takes more than a year to completely cure onychomycosis, and 45.6% agreed that oral antifungals are the most effective treatment for onychomycosis; besides, 44.8% of the respondents thought that everyone can be cured by oral antifungal agents. As regard the question about the contagiousness of onychomycosis, 74.9% of the participants replied that onychomycosis can be transmitted. When divided into age groups, the rate was the lowest in their 60s (67.0%).
Regarding the public awareness of the treatment of onychomycosis, 67.3% of respondents stated that hospitals are essential in treating onychomycosis. When asked about the reason, exact diagnosis was the most important reason, accounting for 52.2%, followed by shorter treatment period (32.5%) and safe treatment (14.4%).
|
Questions |
Respondents |
|
Have you
ever heard about onychomycosis? |
N=621 (100%) |
|
Yes, and I know what it is |
547 (88.1%) |
|
Yes, but I don't know what it is |
71 (11.4%) |
|
No, I've never heard |
3 (0.5%) |
|
How do you
think about onychomycosis? (multiple answer) |
|
|
Can be completely cured with just clear washing |
328 (52.8%) |
|
Causes only cosmetic problem, not a health problem |
240 (38.6%) |
|
Takes over a year to completely cure |
353 (56.8%) |
|
Oral antifungals are the most effective |
283 (45.6%) |
|
Everyone can be cured by oral antifungals |
278 (44.8%) |
|
Is
onychomycosis contagious to other people? |
|
|
Yes |
465 (74.9%) |
|
20~29 y |
116 (76.7%) |
|
30~39 y |
122 (74.6%) |
|
40~49 y |
151 (73.5%) |
|
50~59 y |
144 (79.9%) |
|
Over 60 y |
88 (67.0%) |
|
No |
156 (25.1%) |
|
*Where can onychomycosis be transmitted? |
N=465 (100%) |
|
Finger nail & toenail |
186 (40.0%) |
|
Hand & foot |
111 (23.9%) |
|
Other site |
168 (36.1%) |
|
Do you think
hospitals are essential in treating onychomycosis? |
N=621 (100%) |
|
Yes |
418 (67.3%) |
|
No |
203 (32.7%) |
|
†Why do you think hospitals are essential in treatment? |
N=418 (100%) |
|
Exact diagnosis |
218 (52.2%) |
|
Shorter treatment period |
136 (32.5%) |
|
Safe treatment |
60 (14.4%) |
|
Others |
4 (1.0%) |
3. Experience of onychomycosis
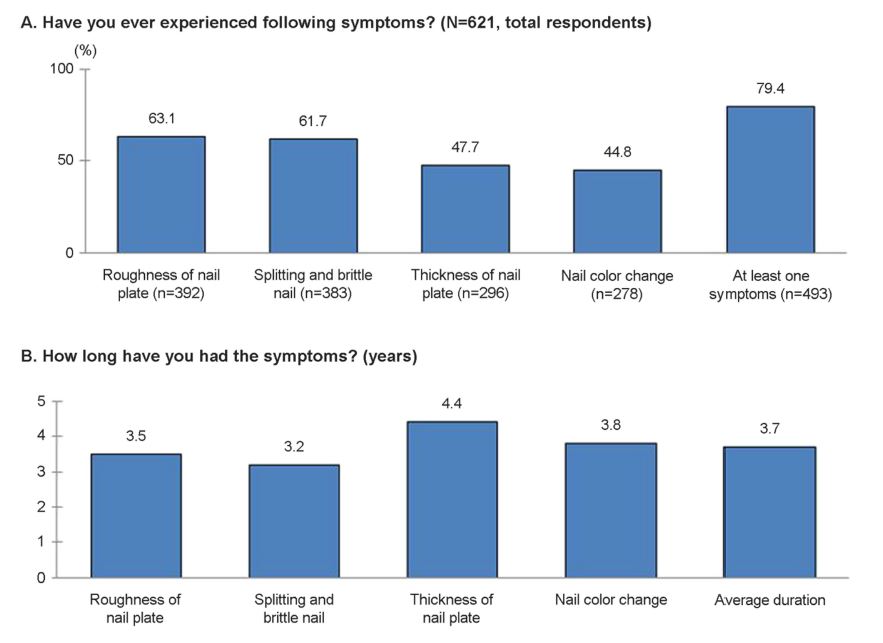
We surveyed the participant's experience of the symptoms, diagnosis, and treatment of onychomycosis. Questions and answers about the onychomycosis symptoms are presented in Figure 1. The experiences of the symptoms were investigated by respondent's subjective symptoms regardless of the expert's confirmation of the onychomycosis. Of the respondents, 79.4% had experienced at least one of the following symptoms in their lifetime: roughness of nail plate (63.1%), splitting and brittle nail (61.7), thickening of nail plate (47.7%), and nail color change (44.8%) (Figure 1A). Of the symptom experienced respondents, male accounted for 50.9%. The number of symptom experienced respondents in their 50s was the largest (25.2%). Also white-collar occupation was the most common occupation (53.5%). The 37.4% of participants were experiencing at least one symptom at the time of the survey. The average duration of the symptoms was 3.7 years (Figure 1B).
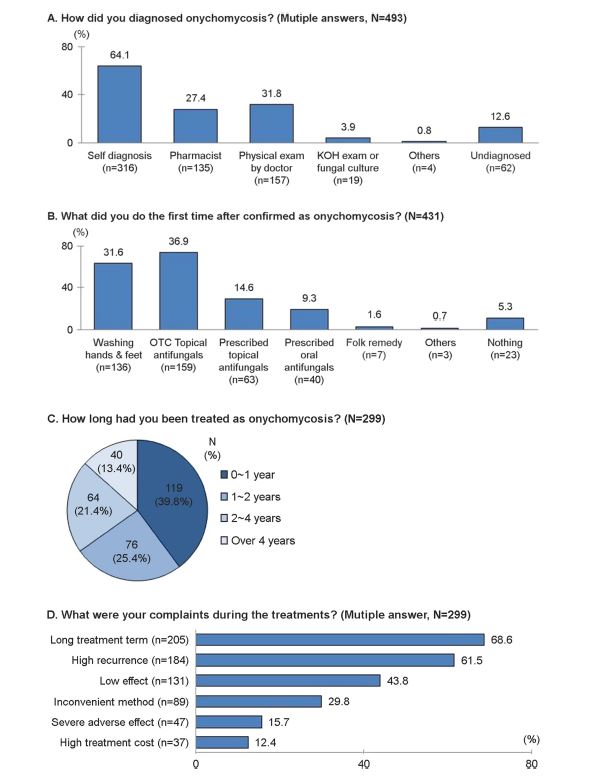
The surveys of the experiences in diagnosis and treatment of onychomycosis are summarized in Figure 2. A total of 493 respondents who experienced any symptoms of onychomycosis were asked about the diagnostic methods. They answered multiple options depending on their experiences (Figure 2A). As a result, self-diagnosis by asking other people around or searching online was the most commonly done diagnostic method (64.1%). Of the participants, 31.8% visited the hospital and were diagnosed by a doctor through physical examination, 27.4% visited the pharmacy and consulted the pharmacist, and only 3.9% were diagnosed through specific tests, such as KOH exam or fungal culture.
A total of 431 respondents diagnosed with onychomycosis were asked about their first action since the confirmation of onychomycosis (Figure 2B). The most common action was purchasing OTC (over the counter) topical antifungals from the pharmacy, which accounted for 36.9%, followed by washing the hands and feet (31.6%), applying topical antifungals prescribed at the hospital (14.6%), taking oral antifungals prescribed at the hospital (9.3%), and applying folk remedies such as vinegar, lemon concentrate, or alum (1.6%).
A total of 299 respondents (60.6% of the respondent who experienced symptoms) had treatment of onychomycosis including not only hospital treatments but also purchasing OTC antifungals at the pharmacy or having folk remedies. Washing the hands and feet was excluded in the treatment criteria. The 299 respondents were surveyed for the treatment duration and their discomforts with the treatments (Figure 2C, Figure 2D). The average treatment duration was 23.7 months. Regardless of the complete cure, treatment duration referred to the period from the start of the treatment to the discontinuation of the treatment or to the time of the survey if continuing treatment until then. A long treatment period was the most common complaint, accounting for 68.6% of the respondents, followed by high recurrence (61.5%), low effect (43.8%), inconvenient method (29.8%), severe adverse effect (15.7%), and high treatment cost (12.4%).
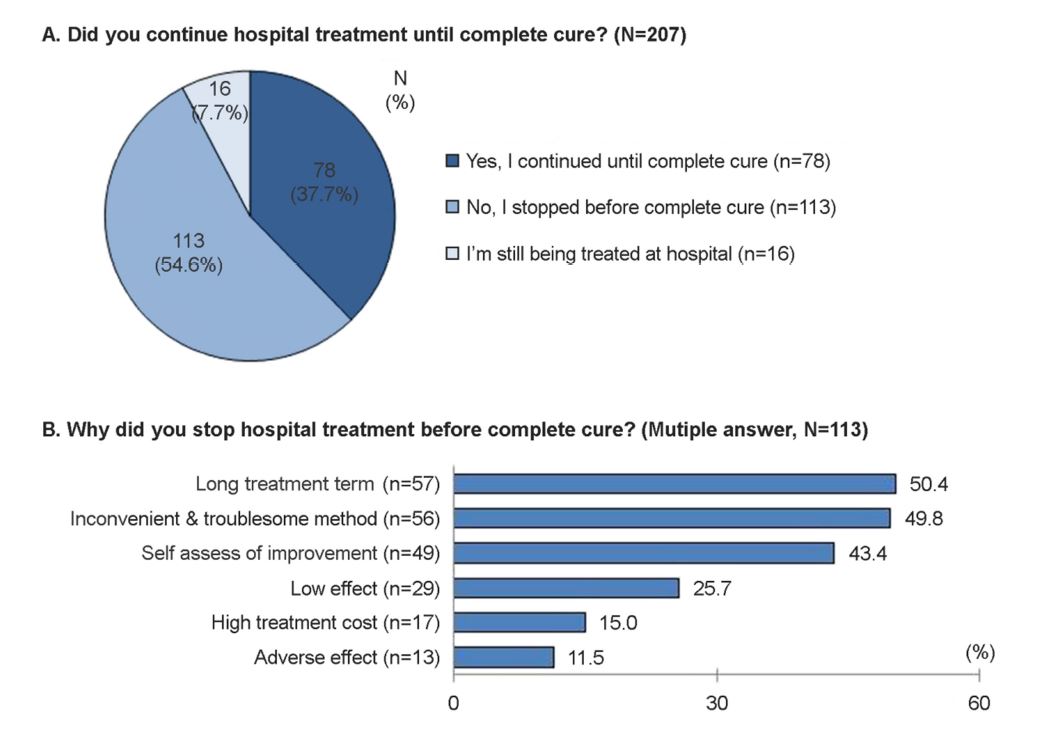
A total of 207 respondents (42.0% of the respondents who experienced symptoms) had hospital treatment of onychomycosis (Figure 3). Among the 207 respondents, 113 respondents (54.6%) had stopped their treatments before complete cure, 78 respondents (37.7%) had continued the treatments until complete cure, and 16 respondents (7.7%) were still being treated at the hospital at the time of the survey (Figure 3A). The 113 respondents who had stopped their hospital treatments before complete cure were asked about the reasons for discontinuation of the treatments (Figure 3B). The 50.4% of the respondent stopped their hospital treatment because of the long treatment period, followed by inconvenient and troublesome method (49.8%), self-assessment of improvement (43.4%), low effect (25.7%), high treatment cost (15.0%), and adverse effects (11.5%).
4. Comorbidity and medication history
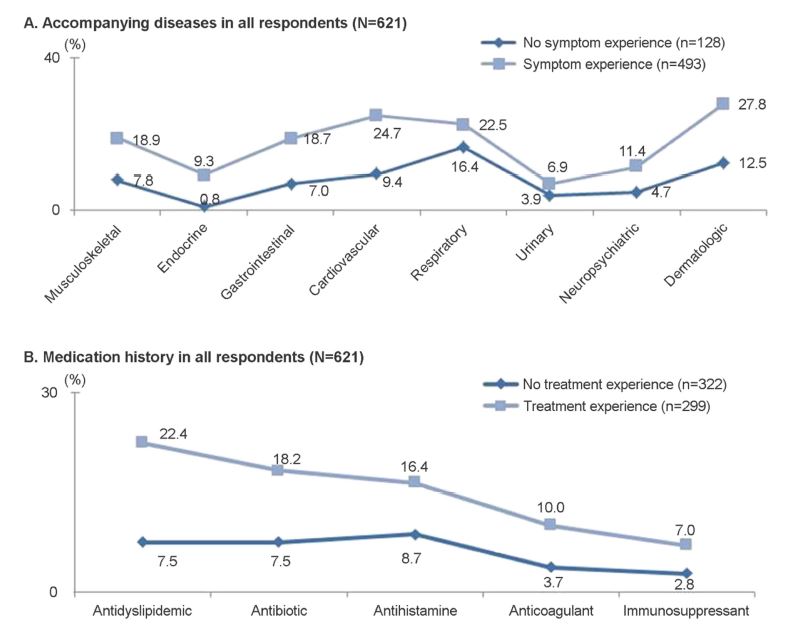
The data of comorbidity and medication history of the participants are presented in Figure 4. Regarding concomitant diseases, respondents were divided into two groups according to the experience of onychomycosis symptom (Figure 4A). Among the 493 respondents who experienced symptoms, dermatologic disease (27.8%) was the most common accompanying disease, followed by cardiovascular (24.7%), respiratory (22.5%), musculoskeletal (18.9%), gastrointestinal (18.7%), neuropsychiatric (11.4%), endocrine (9.3%), and urinary (6.9%) diseases. 34.3% of them replied that they had no accompanying disease. Among the 128 respondents who did not experience onychomycosis symptom, respiratory dis- ease was the most common accompanying disease (16.4%), followed by dermatologic (12.5%), cardiovascular (9.4%), musculoskeletal (7.8%), gastrointestinal (7.0%), neuropsychiatric (4.7%), urinary (3.9%), and endocrine (0.8%) disease. 54.7% of them replied that they had no accompanying disease. Overall, the respondents who experienced onychomycosis symptoms had much more comorbid diseases than the respondents who did not experience onychomycosis symptoms. Medication histories were surveyed in all 621 respondents. They were divided into two groups according to the experience of onychomycosis treatment (Figure 4B). The most commonly taken medicines in 299 respondents who had treatment were cholesterol-lowering drugs (22.4%), followed by antibiotics (18.2%), antihistamines (16.4%), anticoagulants (10.0%), and immunosuppressants (7.0%). 55.9% of them were not taking any medicine. In 322 respondents who did not have onychomycosis treatment, antihistamines were most commonly taken (8.7%), followed by antibiotics and cholesterol-lowering drugs (7.5%), anticoagulants (3.7%), and immunosuppressants (2.8%). 75.5% of them were not taking any medicine. Overall, the respondents with treatment for onychomycosis were taking more other medicines than the respondents with no treatment experiences.
Onychomycosis was a publicly known disease, so 99.5% of all respondents have heard of it and 88.1% of them know what it is. However, according to our survey, correct understanding of onychomycosis was lacking. For example, 52.8% of the respondents agreed that onychomycosis can be cured only by cleaning and managing their hands and feet, and 38.6% of them agreed that it is not related to general health but only to cosmetic problem.
A high rate of the respondents (79.4%) had experienced at least one symptom of onychomycosis, and 37.4% of respondents were suffering those symptoms at the time of the survey. The respondent's subjective symptoms were investigated regardless of the expert's confirmation of the onychomycosis, so that the unexpected high rate of symptom experienced respondents could be the limitation of this study. Despite the high rate of symptoms experienced, self-diagnosis was the most common diagnostic method (64.1%). Only 23.9% of the respondents who was diagnosed with onychomycosis visited the hospital (prescribed topical antifungals, 14.6%, and prescribed oral antifungals, 9.3%) for the first time after confirmation of onychomycosis. This rate was much lower than expected compared to the result that 67.3% of all respondents agreed with the necessity of hospital treatment. These public behaviors should be revised through proper education and guidance by dermatologists.
Among the respondents who had hospital treatment, 54.6% stopped their treatments before complete cure. The main reasons for the discontinuation were long treatment period (50.4%) and inconvenient and troublesome treatment methods (49.6%). Low treatment compliance should also be corrected. Close observation and detailed explanation by dermatologists emphasizing the necessities for the treatments can be helpful.
Onychomycosis is prevailing in elderly people or those who have poor hygiene and low immunity[20]. Thus, concomitant diseases and medication histories are frequent[21]-[22]. Likewise, in this survey, concomitant diseases were more frequent in the group experiencing symptoms, and more medication histories were present in the group having treatment. Antifungal agents frequently interact with other drugs[23]. Considering these results, diagnosis and prescription from experts are even more important.
We found two previous studies reporting on patient's self-recognition of onychomycosis in Mexico[24] and Thailand[25]. In a Mexican study, among 6069 affected patients, 35% had been previously diagnosed with onychomycosis and 27% had been treated by a physician[24]. Further, in a Thai study, the proportions of cases with self-recognition of onychomycosis, diagnosis by a dermatologist, and diagnosis by other physicians were 64.5%, 29.1%, and 6.4%, respectively[25]. The rate of self-diagnosis was high as our result. In Korea, several studies about epidemiologic, clinical, and mycological features of onychomycosis have been reported[9]-[20]. On the other hand, public awareness, experiences, and behaviors about onychomycosis have not been studied in Korea. Through this survey, we would like to emphasize that patient’s behaviors need to be changed and the roles of dermatologists are important in the diagnosis, treatment, and education of the patients. We would also like to inform Korean dermatologists about this public awareness, and we hope the results of this survey could be helpful when encountering patients with onychomycosis.
In relation to this article, I declare that there is no conflict of interest.
References
1. Elewski BE. Onychomycosis. Treatment, quality of life, and economic issues. Am J Clin Dermatol 2000;1:19-26
Crossref
Google Scholar
PubMed
2. Perea S, Ramos MJ, Garau M, Gonzalez A, Noriega AR, del Palacio A. Prevalence and risk factors of tinea unguium and tinea pedis in the general population in Spain. J Clin Microbiol 2000;38:3226-3230
Crossref
Google Scholar
3. Ghannoum MA, Hajjeh RA, Scher R, Konnikov N, Gupta AK, Summerbell R, et al. A large-scale North American study of fungal isolates from nails: The frequency of ony- chomycosis, fungal distribution, and antifungal suscepti- bility patterns. J Am Acad Dermatol 2000;43:641-648
Crossref
Google Scholar
4. Elewski BE, Charif MA. Prevalence of onychomycosis in patients attending a dermatology clinic in northeastern Ohio for other conditions. Arch Dermatol 1997;133:1172 -1173
Crossref
Google Scholar
5. de Berker D. Clinical practice. Fungal nail disease. N Engl J Med 2009;360:2108-2116
Crossref
Google Scholar
PubMed
6. Cheng S, Chong L. A prospective epidemiological study on tineapedis and onychomycosis in Hong Kong. Chin Med J (Engl) 2002;115:860-865
Crossref
Google Scholar
7. Ungpakorn R, Lohaprathan S, Reangchainam S. Preva- lence of foot diseases in outpatients attending the Insti- tute of Dermatology, Bangkok, Thailand. Clin Exp Dermatol 2004;29:87-90
Crossref
Google Scholar
8. Suh MK. Treatment and prophylaxis of onychomycosis. Korean J Med Mycol 2001;6:140-142
Crossref
Google Scholar
9. Hwang SM, Suh MK, Ha GY. Onychomycosis due to nondermatophytic molds. Ann Dermatol 2012;24:175 -180
Crossref
Google Scholar
PubMed
10. Hwang SM, Kim DM, Suh MK, Kwon KS, Kim H, Ro BI, et al. Epidemiologic survey of onychomycosis in Koreans: Multicenter study. Korean J Med Mycol 2011;16:35-43
Crossref
Google Scholar
11. Ahn HS, Park HJ, Lee JY, Cho BK. Classification of onycho- mycosis in Korea. Korean J Med Mycol 2008;13:129-137
Crossref
12. Song YC, Ahn KJ, Kim HO, Kye YC, Choi JH, Park CW, et al. The studies on the concomitant diseases and com- bined medication in patients with onychomycosis. Korean J Med Mycol 2007;12:163-172
Crossref
Google Scholar
13. Lee YW, Suh MK, Lee KH, Ho WY, Ahn KJ, Kim KH. A study of treatment and compliance on onychomycosis. Korean J Med Mycol 2005;10:83-90
Crossref
Google Scholar
14. Kim DH, Park HJ, Lee JY, Cho BK. Clinical study of ony- chomycosis: Factors contributing to the prognosis and response rate according to each factor and summation of factors. Korean J Med Mycol 2005;10:55-69
Crossref
Google Scholar
15. Lim SW, Suh MK, Ha GY. Clinical features and identifi- cation of etiologic agents in onychomycosis. Korean J Dermatol 2004;42:53-60
Crossref
Google Scholar
16. Kim JE, Park HJ, Lee JY, Cho BK. The compliance and long-term follow up of onychomycosis treatment. Korean J Med Mycol 2003;8:110-117
Crossref
Google Scholar
17. Han MH, Choi JH, Sung KJ, Moon KC, Koh JK, Kim BC. Onychomycosis and Trichosporon beigelii. Korean J Der- matol 1999;37:1709-1714
Crossref
Google Scholar
18. Kim JA, Eun HC, Moon SE, Cho KH, Lee HS, Kim BS. Clinical features and classification of nail diseases. Korean J Dermatol 1999;37:1733-1742
Crossref
Google Scholar
19. Lee JM, Shin DH, Choi JS, Kim KH. Analysis of treatment results of patients with tinea unguium and assessment of the real effectiveness of antifungal agents and patient compliance. Korean J Dermatol 1998;36:772-779
Crossref
Google Scholar
20. Yoo JY, Suh MK, Ha GY, Kim H. A clinical and mycological study of onychomycosis in the elderly over 10 years (2001-2010). Korean J Med Mycol 2014;19:83-92
Crossref
Google Scholar
21. Dogra S, Kumar B, Bhansali A, Chakrabarty A. Epidemi- ology of onychomycosis in patients with diabetes mellitus in India. Int J Dermatol 2002;41:647-651
Crossref
Google Scholar
PubMed
22. Cathcart S, Cantrell W, Elewski BE. Onychomycosis and diabetes. J Eur Acad Dermatol Venereol 2009;23:1119 -1122
Crossref
PubMed
23. Ko HC, Kim WI. Increasing therapeutic efficacy for ony- chomycosis. Korean J Med Mycol 2016;21:59-64
Crossref
24. Arenas R, Bonifaz A, Padilla MC, Arce M, Atoche C, Barba J, et al. Onychomycosis. A Mexican survey. Eur J Dermatol 2010;20:611-614
Crossref
Google Scholar
PubMed
25. Bunyaratavej S, Pattanaprichakul P, Leeyaphan C, Chayangsu O, Bunyaratavej S, Kulthanan K. Onychomy- cosis: A study of self-recognition by patients and quality of life. Indian J Dermatol Venereol Leprol 2015;81:270 -274
Crossref
Google Scholar
Congratulatory MessageClick here!
