pISSN : 3058-423X eISSN: 3058-4302
Open Access, Peer-reviewed
pISSN : 3058-423X eISSN: 3058-4302
Open Access, Peer-reviewed

Chihyeon Sohng,Jun Young Kim,Kyung Duck Park,Yong Hyun Jang,Seok-Jong Lee,Yong Jun Bang,Jae Bok Jun,Weon Ju Lee
10.17966/JMI.2019.24.3.79 Epub 2019 October 02
Abstract
Background: Tinea capitis is a contagious fungal infection that occurs predominantly in childhood. Although its incidence has declined, its epidemiological and mycological characteristics are continue to evolve.
Objective: To assess changes in the epidemiological and mycological characteristics of tinea capitis in teenage patients in Southeastern Korea.
Methods: We retrospectively investigated epidemiological and mycological characteristics of 202 teenage patients with tinea capitis who visited Kyungpook National University Hospital and the Catholic Skin Disease Clinic from 1989-2018.
Results: Of 202 patients, 177 patients showed KOH-positivity. Dermatophytes were cultured from 157 patients. The annual incidence of tinea capitis ranged from 0 to 30 between 1989 and 2018. Of 202 patients, 153 patients (75.74%) were male and 49 patients (24.26%) were female. The ratio of male to female was 1:0.32. For seasonal distribution, 78 patients (38.61%) visited our hospital in winter, 59 patients (29.21%) visited in spring, 35 patients (17.33%) visited in fall, and 30 patients (14.85%) visited in summer. Microsporum canis was the most common dermatophyte (44.06%) isolated from tinea capitis. Trichophyton tonsurans was the second most common dermatophyte (26.73%). For inhabitancy distribution, 151 patients (74.75%) lived in urban areas and 51 (25.25%) lived in rural areas.
Conclusion: The epidemiological characteristics of teenage patients with tinea capitis were distinct from those of adults in annual incidence, sexual distribution and isolated dermatophytes. Trichophyton tonsurans was the main causative organism of tinea capitis in recent 10 years. These results are useful for the targeted treatment and prevention of tinea capitis.
Keywords
Korea Teenage Tinea capitis Trichophyton tonsurans
Tinea capitis is one of several dermatophytoses caused by dermatophyte fungi and is highly contagious in children1. Trichophyton (T.) ferrugineum was the most common dermatophyte in Korean tinea capitis in the 1960s2. However, Microsporum (M.) canis has been prevalent since the 1970s3. In recent periods, T. tonsurans was reported as a causative fungus of tinea capitis4,5. Indeed, T. tonsurans has been found to be the main causative fungus of tinea capitis in teenagers6. T. tonsurans was thought to be originally imported from athletes during the international game7. Tinea capitis caused by T. tonsurans clinically manifests as scaly patches with black dots on the scalp. Here, we retrospectively investigated and analyzed changes in the epidemiological and mycological characteristics of tinea capitis in teenage patients in Southeastern Korea.
1. Patients
To analyze the epidemiological and mycological characteristics of patients with tinea capitis, we retrospectively reviewed medical records and identified a total 1,254 patients with tinea capitis who visited Kyungpook National University Hospital and Catholic Skin Disease Clinic from 1989-2018. Only teenage (ages 10-19) patients were included: a total of 202 teenage patients were identified. We investigated annual incidence, sexual distribution, seasonal distribution, isolated dermatophytes, and residence of each patient. To analyze changes over time, patients were divided into three groups according to visit date: Group A: 1989-1998, Group B: 1999- 2008, Group C: 2009-2018.
2. Diagnosis of Trichophyton infection
Scales and hairs were obtained from patients' scalps for fungal examination, and 15% potassium hydroxide (KOH) examination was performed. Of 202 patients, 177 (87.62%) showed KOH-positivity. Causative dermatophytes were isolated from fungal culture using potato dextrose agar corn meal Tween 80 media. The culture media were stored at 24~26℃ and examined after 2~4 weeks. Dermatophytes were successfully cultured from 157 of 202 patients. In addition, microscopic examination was performed with lactophenol cotton blue stain to identify filamentous fungi with conidia. A Wood lamp was also used to detect fluorescent fungal elements.
3. Ethics statements
This study was conducted after approval by the Institutional Review Board of Kyungpook National University Hospital (IRB No. 2019-03-014). Informed patient consent was waived by the board.
1. Incidence
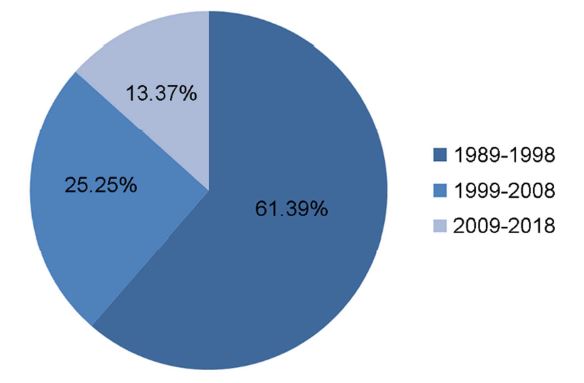
Of 1254 patients diagnosed with tinea capitis between 1989 and 2018, 202 teenage patients (16.11%) were identified. Of 780 patients with tinea capitis from 1989-1998, 124 (15.90%) were teenagers (Group A). Of 271 patients diagnosed with tinea capitis from 1999-2008, 51 (18.82%) were teenagers (Group B). Of 203 patients diagnosed with tinea capitis from 2009-2018, 27 (13.30%) were teenagers (Group C). Of 202 teenage tinea capitis patients between 1989 and 2018, 124 (61.39%) were in Group A, 51 (25.25%) were in Group B, and 27 (13.37%) were in Group C (Figure 1).
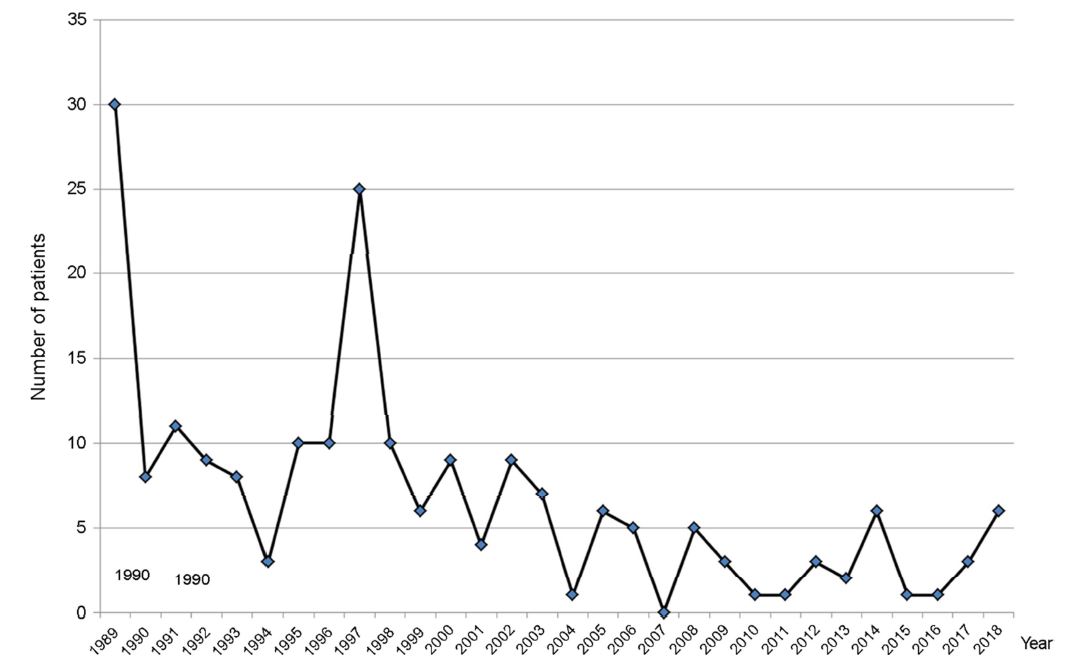
The annual incidence of teenage tinea capitis ranged from 0 to 30 between 1989 and 2018 (Figure 2). The mean annual incidence of teenage tinea capitis was 12.4 in Group A, 5.1 in Group B and 2.7 in Group C. The mean annual incidence of teenage tinea capitis was 6.7 from 1989-2018. The incidence was lowest in 2007 and highest in 1989.
2. Sexual distribution
Of 124 patients of Group A, 96 patients (77.42%) were male and 28 patients (22.58%) were female. The ratio of male to female was 1:0.29. Of 51 patients of Group B, 38 patients (74.51%) were male and 13 patients (25.49%) were female. The ratio of male to female was 1:0.34. Of 27 patients of Group C, 19 patients (70.37%) were male and eight patients (29.63%) were female. The ratio of male to female was 1:0.42. Of 202 patients, 153 patients (75.74%) were male and 49 patients (24.26%) were female. The ratio of male to female was 1:0.32.
3. Seasonal distribution
Of 124 patients of Group A, 48 patients (38.71%) visited our hospital in winter, 41 patients (33.06%) visited in spring, 24 patients (19.35%) visited in fall, and 11 patients (8.87%) visited in summer. Of 51 patients of Group B, 18 patients (35.29%) visited our hospital in winter, 16 patients (31.37%) visited in summer, nine patients (17.65%) visited in spring, and eight patients (15.69%) visited in fall. Of 27 patients of Group C, 12 patients (44.44%) visited our hospital in winter, 9 patients (33.33%) visited in spring, three patients (11.11%) visited in summer, and three patients (11.11%) visited in fall. Of 202 patients, 78 patients (38.61%) visited our hospital in winter, 59 patients (29.21%) visited in spring, 35 patients (17.33%) visited in fall, and 30 patients (14.85%) visited in summer (Table 1).
|
Period |
Season |
Total |
|||
|
Spring |
Summer |
Fall |
Winter |
||
|
1989-1998 |
41 |
11 |
24 |
48 |
124 |
|
1999-2008 |
9 |
16 |
8 |
18 |
51 |
|
2009-2018 |
9 |
3 |
3 |
12 |
27 |
|
Total |
59 |
30 |
35 |
78 |
202 |
4. Isolation of dermatophytes
In Group A, M. canis was the most common dermatophyte (50.81%) isolated from tinea capitis. T. tonsurans was the second most common dermatophyte (21.77%). T. rubrum was isolated from three patients. T. mentagrophytes, T. verrucosum and M. ferrugineum were isolated from two patients, respectively. In Group B, M. canis was the most common dermatophyte (37.25%) isolated from tinea capitis. T. tonsurans was the second most common dermatophyte (23.53%). T. rubrum was isolated from three patients. T. mentagrophytes and T. verrucosum were isolated from only one patient, respectively. In Group C, T. tonsurans was the most common dermatophyte (55.56%) isolated from tinea capitis. M. canis was the second most dermatophyte (25.93%) isolated from tinea capitis. In 202 teenage patients, M. canis was the most common dermatophyte (44.06%) isolated from tinea capitis. T. tonsurans was the second most common dermatophyte (26.73%) (Table 2).
|
Period |
Causative fungus |
|||||||||
|
M. |
T. |
T. |
T. |
T. |
M. |
M. |
Contaminant |
Negative |
Total |
|
|
1989-1998 |
63 |
3 |
2 |
2 |
27 |
0 |
2 |
5 |
20 |
124 |
|
1999-2008 |
19 |
3 |
1 |
1 |
12 |
0 |
0 |
9 |
6 |
51 |
|
2009-2018 |
7 |
0 |
0 |
0 |
15 |
0 |
0 |
1 |
4 |
27 |
|
Total |
89 |
6 |
3 |
3 |
54 |
0 |
2 |
15 |
30 |
202 |
5. Inhabitancy distribution
Of 124 patients of Group A, 88 patients (70.97%) lived in urban areas and 36 (29.03%) patients lived in rural areas. Of 51 patients of Group B, 39 patients (76.47%) lived in urban areas and 12 patients (23.53%) lived in rural areas. Of 27 patients of Group C, 24 patients (88.89%) lived in urban areas and three patients (11.11%) lived in rural areas. Of 202 teenage patients with tinea capitis, 151 patients (74.75%) lived in urban areas and 51 patients (25.25%) lived in rural areas.
6. Coexisting dermatophytosis
Tinea faciei coexisted with tinea capitis in seven patients in Group C. Tinea corporis coexisted in nine patients in Group C.
7. Clinical features
Almost all of patients in Group C presented with scaly hairless patches and/or folliculitis on the scalp. Only three patients had kerion celsi.
8. Causative factors and underlying diseases
Of 27 patients in Group C, one had a past history of contact with a cat and two had atopic dermatitis as an underlying disease. Two patients were judoists and 13 patients were wrestlers.
9. Treatment of tinea capitis
All patients had been treated with antifungals, such as oral itraconazole and terbinafine.
T. ferrugineum was identified as a major causative fungus of Korean tinea capitis in the 1960s2. M. canis has been the most prevalent cause of tinea capitis in Korea since the 1970s3. Starting in 1995, a nation-wide outbreak of trichophytosis gladiatorum caused by T. tonsurans was noted among wrestlers and judoists in Korea. Jun and Choi4 and Jun and Kim5 reported the epidemiological, clinical and mycological characteristics of trichophytosis gladiatorum caused by T. tonsurans in Korean wrestlers and judoists. They found that patients with trichophytosis gladiatorum were predominantly teenagers. Tinea capitis was the most common type of dermatophytosis in these patients. It was followed by tinea corporis and tinea faciei in incidence.
Trichophytosis gladiatorum is usually found on the head, neck, and extremities. This distribution supports the notion that skin-to-skin transmission is the most common cause of dermatophytosis8. Wrestlers and judoists occasionally travel and board in a group setting, increasing the likelihood of trichophytosis gladiatorum outbreaks. In addition, infected players often participate in competitions without any prevention or treatment, therefore serving as a reservoir for transmission of fungal organisms to other players. Indeed, in 1995, Hradil et al.9 reported an outbreak of dermatophytosis caused by T. tonsurans in 19 Swedish wrestlers who competed against American athletes, demonstrating the possibility of international disease spread. In this study, of 27 teenage patients diagnosed with tinea capitis from 2009-2018, 15 (55.56%) were wrestlers or judoists, and T. tonsurans was the most frequent dermatophyte (55.56%) isolated.
Iikit et al.10 studied Turkish wrestling patients with trichophytosis gladiatorum. They found that the scalp was the most common site of infection and that T. tonsurans was the most common causative fungus. Hedayati et al.11 also reported patients with trichophytosis gladiatorum in Iran. They demonstrated that the patients were teenagers with most lesions located on the trunk and head. In addition, T. tonsurans was isolated from all patients. Other outbreaks of tinea gladiatorum due to T. tonsurans have also been reported12-18.
Griseofulvin has been the treatment of choice for tinea capitis over 30 years before the advent of new antifungal agents such as terbinafine and itraconazole. Terbinafine may be a more desirable agent for tinea capitis caused by T. tonsurans because of shorter treatment schedule and lower recurrence rate19. Itraconazole is as effective as griseofulvin and terbinafine, and the pulsed regimen was also reported to be effective on tinea capitis20-22. Ketoconazole is avoided in children because of hepatotoxicity and its effectiveness over griseofulvin is controversial23. Proper treatment of dermatophytoses in athletes, especially judoists and wrestlers, is necessary to prevent future outbreaks during regular competitions and practices. The patients in our study were treated with either oral terbinafine or itraconazole.
Data from this study were extracted from the medical records of teenage patients with tinea capitis who were wrestlers, yudoists or neither. We found that M. canis was the most common dermatophyte isolated from teenage patients with tinea capitis and that T. tonsurans was the second most common dermatophyte isolated from teenage patients with tinea capitis. Interestingly, T. tonsuran was the most common cause of tinea capitis in teenage patients in recent 10 years. Common coexisting dermatophytoses were tinea faciei and tinea corporis. Generally, we found that the incidence of tinea capitis in teenage patients decreased from 124 in the 1990s to 27 in the 2010s. In contrast to adult patients, there was male predominance in sexual distribution of teenage patients.
In summary, the epidemiological characteristics of teenage patients with tinea capitis were different from those of children and adults with tinea capitis in annual incidence, sexual distribution and isolated dermatophytes. The incidence of tinea capitis is decreasing. In addition, T. tonsurans has recently emerged as a new common causative fungus in teenage patients with tinea capitis, especially in wrestlers and judoists. These findings may be useful for the treatment and prevention of tinea capitis in teenagers.
References
1. Gits-Muselli M, Benderdouche M, Hamane S, Mingui A, Feuilhade de Chauvin M, Guigue N, et al. Continuous increase of Trichophyton tonsurans as a cause of tinea capitis in the urban area of Paris, France: a 5-year-long study. Med Mycol 2017;55:476-484
Google Scholar
2. Hong JK. A supplementary study on tinea capitis in Taegu city. Korean J Dermatol 1962;2:7-14
Google Scholar
3. Oh SH, Kim SH, Suh SB. Tinea capitis of adults in Taegu City for 11 years (1978-1988). Korean J Dermatol 1989; 27:666-671
Google Scholar
4. Jun JB, Choi SK. The epidemiological, clinical and mycological studies of trichophytosis gladiatorum prevailing among Korean judoists. Korean J Med Mycol 2004;9:100-111
Google Scholar
5. Jun JB, Kim YD. The epidemiological, clinical and mycological studies of trichophytosis gladiatorum prevailing among Korean wrestlers. Korean J Med Mycol 2004;9:28-44
6. Park JS, Kim SW, Jun JB, Suh SB, Bang YJ. Clinical and epidemiological study of Trichophyton tonsurans infections (1995-2003). Korean J Med Mycol 2004;9:197-205
Google Scholar
7. Kim KH. Changing patterns of dermatophytosis and its causative agents according to social and economic developments in Korea. Korean J Med Mycol 2006;11:1-12
Google Scholar
8. Adams BB. Tinea corporis gladiatorum: a cross sectional study. J Am Acad Dermatol 2000;43:1039-1041
Google Scholar
9. Hradil E, Hersle K, Nordin P, Faergemann J. An epidemic of tinea corporis caused by Trichophyton tonsurans among wrestlers in Sweden. Acta Derm Venereol 1995;75:
Google Scholar
10. Ilkit M, Gümral R, Saraçli MA, Burqut R. Trichophyton tonsurans scalp carriage among wrestlers in a national competition in Turkey. Mycopathologia 2011;172:215-222
Google Scholar
11. Hedayati MT, Afshar P, Shokohi T, Aghili R. A study on tinea gladiatorum in young wrestlers and dermatophyte contamination of wrestling mats from Sari, Iran. Br J Sports Med 2007;41:332-334
Google Scholar
12. Pique E, Copado R, Cabrera A, Olivares M, Fariña MC, Escalonilla P, et al. An outbreak of tinea gladiatorum in Lanzarote. Clin Exp Dermatol 1999;24:7-9
Google Scholar
13. Beller M, Gessner BD. An outbreak of tinea corporis gladiatorum on a high school wrestling team. J Am Acad Dermatol 1994;31:197-201
Google Scholar
14. Stiller MJ, Klein WP, Dorman RI. Tinea corporis gladiatorum: an epidemic of Trichophyton tonsurans in student wrestlers. J Am Acad Dermatol 1992;27:632-633
Google Scholar
15. el Fari M, Gräser Y, Presber W, Tietz HJ. An epidemic of tinea corporis caused by Trichophyton tonsurans among children (wrestlers) in Germany. Mycoses 2000;43:191-196
Google Scholar
16. Poisson D M, Rousseau D, Defo D, Estève E. Outbreak of tinea corporis gladiatorum, a fungal skin infection due to Trichophyton tonsurans, in a French high level judo team. Euro Surveill 2005;10:187-190
Google Scholar
17. Ergin S, Ergin C, Erdoğan BS, Kaleli I, Evliyaoğlu D. An experience from an outbreak of tinea capitis gladiatorum due to Trichophyton tonsurans. Clin Exp Dermatol 2006; 31:212-214
Google Scholar
18. Kim SL, Lee KC, Jang YH, Lee SJ, Kim DW, Lee WJ, et al. The epidemiology of dermatophyte infection in Southeastern Korea (1979-2013). Ann Dermatol 2016;28:524-527
Google Scholar
19. Cáceres-Ríos H, Rueda M, Ballona R, Bustamante B. Comparison of terbinafine and griseofulvin in the treatment of tinea capitis. J Am Acad Dermatol 2000;42:80-84
Google Scholar
20. López-Gómez S, Del Palacio A, Van Cutsem J, Soledad Cuétara M, Iglesias L, Rodriguez-Noriega A. Itraconazole verses Griseofulvin in the treatment of tinea capitis: a double blind randomized study in children. Int J Dermatol 1994;33:743-747
Google Scholar
21. Jahangir M, Hussain I, Ul Hasan M, Haroon TS. A double-blind randomized comparative trial of itraconazole versus terbinafine for 2 weeks in tinea capitis. Br J Dermatol 1998;139:672-674
Google Scholar
22. Gupta AK, Alexis ME, Raboobee N, Hofstader SL, Lynde CW, Adam P, et al. Itraconazole pulse therapy is effective in the treatment of tinea capitis in children: an open multicentre study. Br J Dermatol 1997;137:251-254
Google Scholar
23. Gan VN, Petruska M, Ginsburg CM. Epidemiology and treatment of tinea capitis. ketoconazole vs. griseofulvin. Paediatr Infect Dis J 1987;6:46-49
Google Scholar
Congratulatory MessageClick here!
