pISSN : 3058-423X eISSN: 3058-4302
Open Access, Peer-reviewed
pISSN : 3058-423X eISSN: 3058-4302
Open Access, Peer-reviewed
Soo Yuhl Chae,Kyou Chae Lee,Hae Sook Lee,Yong Hyun Jang,Seok-Jong Lee,Do Won Kim,Weon Ju Lee
http://dx.doi.org/10.17966/KJMM.2015.20.1.13 Epub 2015 September 17
Abstract
Protothecosis is a rare skin infection caused by pathogenic algae of the genus Prototheca, especially Prototheca
wickerhamii. It is widely distributed throughout the natural world in tree, river, lake, sewage,soil, marsh, household
waste, etc. A 79-year-old woman presented with ill-defined edematous and erythematous patches with various sized and shaped deep ulcers on both dorsal hands and left distal forearm for 1 month. The left forearm was initially injured by scratching due to pruritus and insidiously aggravated. Biopsy specimen revealed the characteristic morula-like sporangias containing multiple endospores in the dermis. The GMS and D-PAS stains highlighted the characteristic spores showing multiple internal septations and some unicellular endospore. P. wickerhamii was isolated in culture and
identified by biochemical studies. Oral itraconazole 200 mg/day administration for 7 weeks resulted in marked
improvement of the skin lesion.
Keywords
Cutaneous protothecosis Prototheca wickerhamii
서 론
프로토테카증은 녹색조류인 Chlorella와 유사한 호기성, 비엽록소성의 조류인 Prototheca 균종에 의해 유발되는 드문 감염증이다[1],[2]. 현재까지 Prototheca(P.) wickerhamii, P. zopffi, P. stagnora, P. ulmea, P. blaschkeae sp. Nov., 그리고 P. cutis sp. Nov.의 균주가 알려져 있으며[3], 이들은 나무, 강, 호수, 하수, 토양, 습지 및 가정 폐기물 등에 서식 한다[4]. 인간과 동물에 감염을 일으킬 수 있으나, 인체에 감염될 경우에는 P. zopffi, P. wickerhamii가 관련되며, 대부분에서 P. wickerhamii가 원인이 되고, 면역이 저하된 환자에게 발생한다[5],[6]. 임상적으로 피부 감염 (66%), 주두활액낭염 (olecranonbursitis) (15%), 전신 감염 (19%) 등 다양한 양상으로 나타난다[7].
저자들은 정상 면역을 가진 79세 여자 환자에서 외상을 받은 후 발생한 양측 손등과 좌측 전 완부에 다양한 크기와 모양의 깊은 궤양을 가진 경계가 불명확한 홍반성 판의 임상 양상을 보인 피부 프로토테카증 1예를 경험하고 문헌고찰과 함께 보고한다.
증 례
환 자: 김OO, 79세, 여자
주 소: 양측 손등과 좌측 전완부에 다양한 크기와 모양의 깊은 궤양을 가진 경계가 불명확한 홍반성 판
현병력: 1개월 전 좌측 전완부에 소양감이 있어 긁은 후 상처가 발생하여 개인의원에서 항생제 복용 및 항생제와 스테로이드가 혼합된 연고를 도포하였으나 악화되어, 양측 손등과 좌측 전완부에 다양한 크기와 모양의 깊은 궤양을 가진 경계가 불명확한 홍반성 판으로 진행되어 내원함.
과거력 및 가족력: 수년 전부터 고혈압으로 치료 중이며, 무릎의 관절통으로 40년 정도 성분 미상의 약을 복용하다
10년 전에 중단하였음.
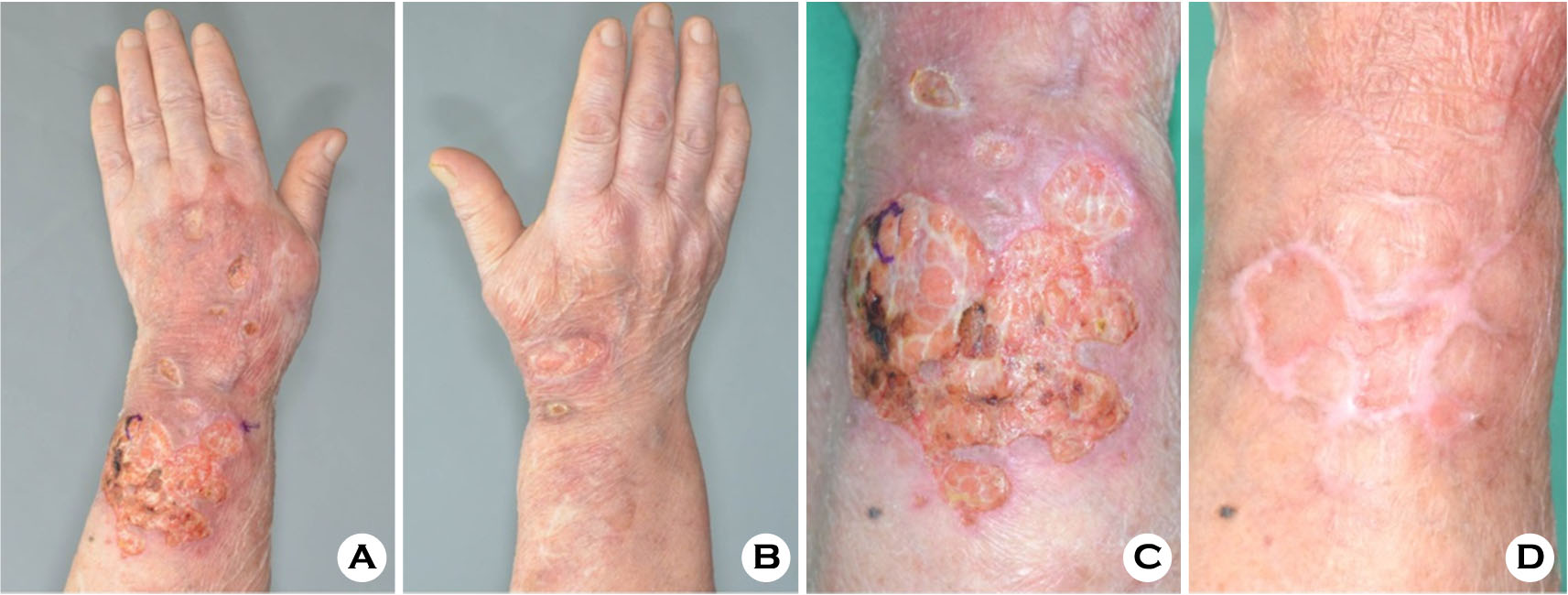
피부 소견: 양측 손등과 좌측 전완부에 압통을 동반한 다양한 크기와 모양의 깊은 궤양을 가진경계가 불명확한 홍반성 판 (Fig. 1A, 1B).
이학적 소견: 피부 소견 외에 다른 특이사항 없음.
검사 소견: 일반혈액검사상 ESR이 34 mm/hr, WBC 17,680/μl으로 증가되었으며 이외 다른 일반 혈액 검사, 흉부 X선상 특이 소견 없었다. Mantaux test에서 특이 반응이 없었으나, 조직에서 시행한 Tbc PCR에서 양성 확인되어, 호흡기 내과에서 QuantiFERON®-TB Gold test (Cellestis Limited, Australia) 시행하였으나 음성 확인되었다.
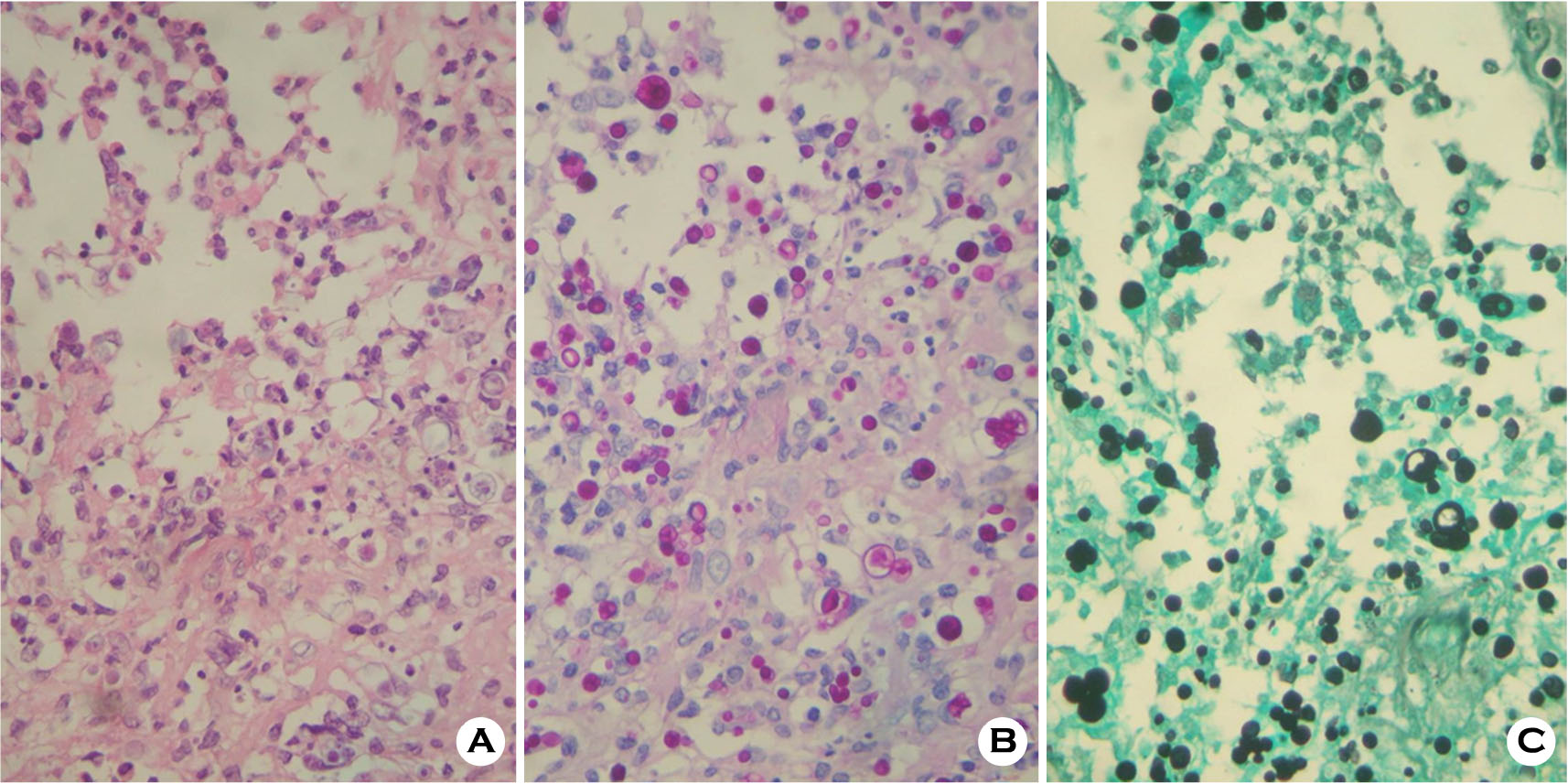
병리 조직학적 소견: 궤양의 변연부에서 조직검사를 시행하였으며, H&E 염색상 표피에 국소적인 과각화증, 이상각화증, 가시세포증이 관찰되었으며, 진피 전반에 걸쳐서 조직구와 림프구의 침윤과 둥근 포자들이 관찰되었고, 고배율에서는 내부 중격과 내생포자 (endospore)가 모인 특징적인 상실배 모양의 포자낭 (sporangia)을 확인할 수 있었다 (Fig. 2A). 이러한 소견은 periodicacid-Schiff with diastase (D-PAS) 염색과 Gomorimethenamine-silver (GMS) 염색에서 더 뚜렷하게 관찰할 수 있었다 (Fig. 2B, 2C).
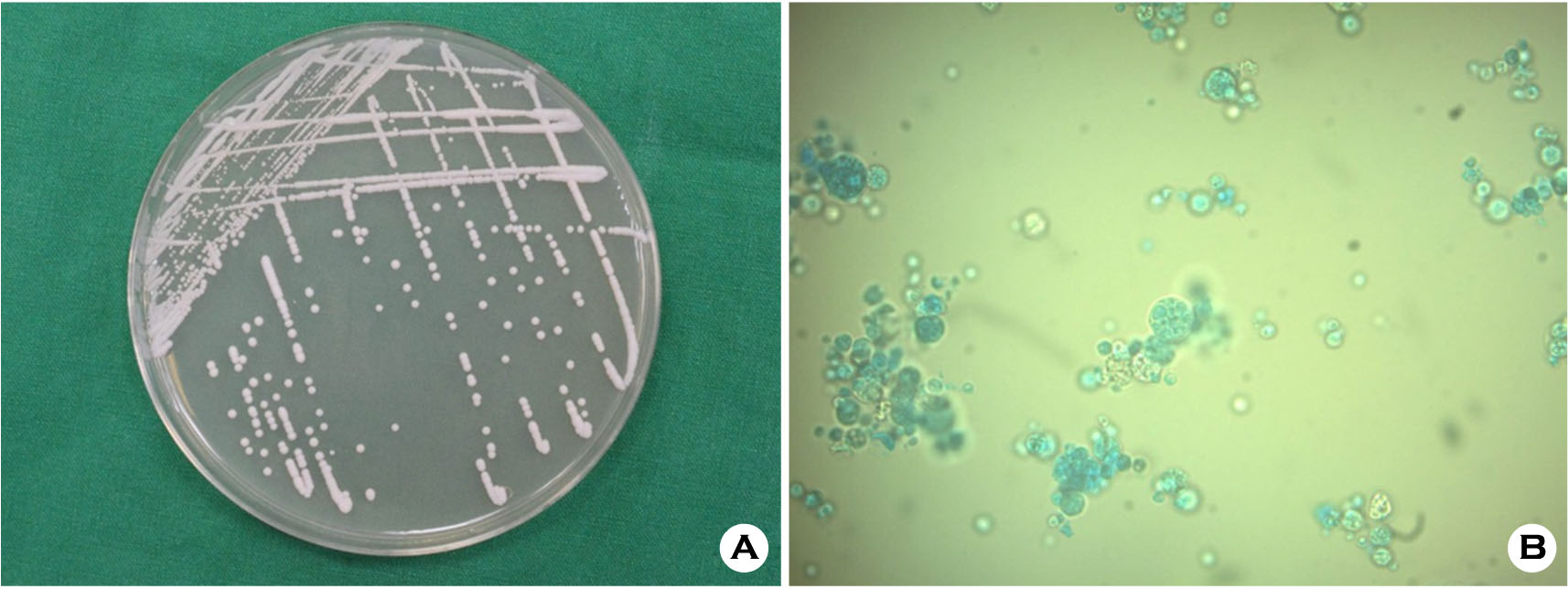
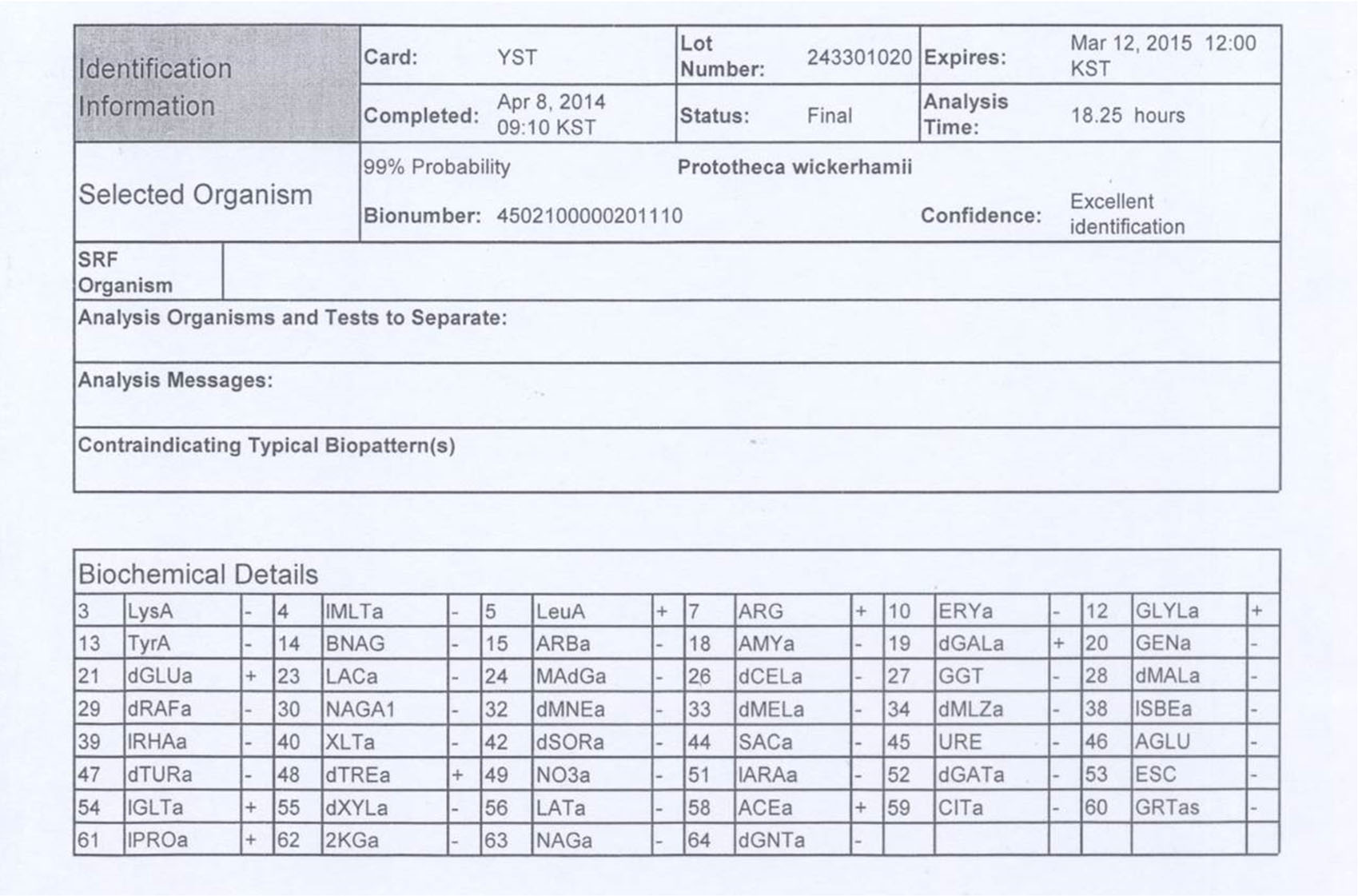
진균학적 소견: Potato dextrose agar에 corn meal agar, peptone, tween 80을 첨가한 것을 기본으로 한 PDAC 배지에 30℃에서 4일 배양 후 백색 크림 형태의 집락이 형성되었으며 (Fig. 3A), 배양된 집락을 lactophenol cotton blue 염색을 시행하여 다수의 내생포자를 함유한 포자낭들이 확인되었다(Fig. 3B). VITEK 2® (bioMérieux, Marcy l'Etoile,France) 자동화 시스템의 YST card를 사용한 검사에서 Prototheca wickerhamii로 동정되었다 (Fig. 4).
치료 및 경과: 환자는 매일 itraconazole 200 mg씩 7주간 경구 투여로 치료하여 병변은 치유되었고 (Fig. 1C), 치료 종료 6개월이 지났으나 재발의 소견은 보이지 않고 있다.
고 찰
프로토테카증은 Prototheca 종에 의해 인간과동물에서 드물게 발생하는 감염으로, 인체에 감염된 경우는 1964년에 아프리카 농부에게 발생한 피부 프로토테카증이 처음 알려졌으며, 이후로 증가하는 추세를 보이고 있다[8],[9]. Prototheca 종은 ribosomal RNA 연구에서 계통발생학적으로 청녹색 조류에 가까우며[10], 호기성, 비엽록소 단일 세포 (aerobic, achlorophillic, unicellular algae)로 구성된 조류로 알려져 있다[1],[2]. 그러나 토양이나 물에서 생활하며 세포벽이 ergosterol로 구성이 되어 있고, 진균 배양배지에서 잘 자라고, 항진균제의 치료에 잘 반응하여 생물학적으로 진균과 유사한 특성을 지닌다[11].
인체의 감염경로는 면역력이 약해져 있거나 미세한 외상을 받은 피부, 호흡기 또는 소화기를 통해 감염되며 잠복기는 확실하게 알려져 있지 않으나 수 주에서 수 개월 정도로 생각된다[3],[12]. 프로토테카증의 임상 양상은 전형적으로 피부 및 피하 감염, 주두부 활액낭염, 전신 감염 세 가지 형태로 나타날 수 있는데, 피부 감염은 대부분 피부 결손이나 외상이 있는 부위에 일어나며, 면역력이 저하된 경우에 전신으로 쉽게 퍼질 수 있다. 피부 및 피하 감염은 일반적으로 홍반, 구진, 결절, 궤양, 소수포, 사마귀양 또는 포진상 병변, 조갑박리증 등으로 다양하게 나타나며, 노출 부위 특히 사지에서 잘 발생한다[3]. 건강한 사람에서도 감염될 수 있으나, 대부분 악성종양, 당뇨, 장기이식, 스테로이드제의 장기투여 등에 의해 면역력이 저하된 환자에 발생하는 것으로 보고되었다[1],[9].
프로토테카증은 다양한 피부 증상을 보일 수 있으므로 본증이 의심될 경우에는 조직 검사와 배양 검사가 반드시 시행되어야 한다[13]. 조직 생검상 고배율에서 H&E 염색상 다수의 내부 중 격과 6~11 μm 크기의 내생포자들을 함유한 특징적인 상실배 모양을 보이는 3~30 μm 크기의 포자낭을 관찰할 수 있다[11],[14]. 이러한 소견은 PAS염색, GMS 염색, Lieb's crystal violet 염색을 시행하면 더 뚜렷이 관찰할 수 있다[15]. 배양 검사 시 25℃에서 37℃ 사이에서 가장 잘 자라고, 백색크림의 효모 모양 집락을 보이며, 이를 도말하여 lactophenol cotton blue로 염색하면 내생포자를 가진 특징적인 포자낭을 관찰할 수 있다[14],[16]. Blastomyces dermatitidis, Cryptococcus neoformans, Paracoccidioides brasiliensis, Rhinosporidium seeberi, Coccidiodes immitis 등의 균주와 감별이 필요하다[17]. 또한 Prototheca의 다른 종과도 감별이 필요하며, 효모동정용 카드를 사용하여 당대사에 대한 생화학적 성상을 비교하여 균주를 확진할 수있다.
프로토테카증의 정해진 표준 치료는 현재까지 없다. 면역이 정상인 환자에서 국소적 표재성 감염은 수술적 절제를 시행할 수 있으나, 항진균제에 반응이 좋아 일반적으로 amphotericin B 정맥내 주사가 가장 널리 사용된다[16]. 그리고 ketoconazole, itraconazole, fluconazole, tetracycline은 대부분 국한된 병변에 사용되나, 적정용량과 기간에 대해서는 아직 명확하게 확립되지 않았다[7].
피부 프로토테카증은 드문 질환으로 국내에서는 문헌상 모두 11 증례가 보고되어 있는데, 1예에서 P. zopfii가 배양되었고, 이외 모두 P.wickerhamii가 배양되었다. 대부분의 환자는 여성이었으며, 스테로이드제의 장기 투여, 당뇨 등의 면역저하요인이 있는 사람들이 많았다. 환자의 대부분이 itraconazole로 치료를 시작하였으며, 이에 저항을 보인 경우, fluconazole 치료 또는 국소 병변부 수술적 절제로 치료를 하였다[18],[19]. 본 증례는 정상 면역을 가진 고령의 여성 환자에서 외상을 받은 후 P. wickerhamii에 의해 발생한 프로토테카증으로 itraconazole에 성공적인 치료효과를 보인 비교적 드문 증례로 생각되어 보고하는 바이다.
References
1. Boyd AS, Langley M, King LE. Cutaneous manifestations of prototheca infections. J Am Acad Dermatol 1995;32:758-764
Google Scholar
2. Tejada E, Parker CM. Cutaneous erythematous nodular lesion in a crab fisherman. Protothecosis. Arch Dermatol 1994;130:244-245, 247-248
Google Scholar
3. Zhang Q, Li L, Yuli K, Zhao Y, Zhu J, Zhu M. A case of cutaneous protothecosis mimics eczema. Mycopathologia 2014
4. Pore RS, Barnett EA, Barnes WC, Jr., Walker JD. Prototheca ecology. Mycopathologia 1983;81:49-62
Google Scholar
5. Sheikh-Ahmad M, Goldstein S, Potasman I. Prototheca wickerhamii hand infection successfully treated by itraconazole and voriconazole. J Travel Med 2006; 13:321-323
Google Scholar
6. Torres HA, Bodey GP, Tarrand JJ, Kontoyiannis DP. Protothecosis in patients with cancer: case series and literature review. Clin Microbiol Infect 2003;9:786 -792
Google Scholar
7. Lass-Florl C, Mayr A. Human protothecosis. Clin Microbiol Rev 2007;20:230-242
Google Scholar
8. Davies RR, Spencer H, Wakelin PO. A case of human protothecosis. Trans R Soc Trop Med Hyg 1964;58: 448-451
Google Scholar
9. Todd JR, King JW, Oberle A, Matsumoto T, Odaka Y, Fowler M, et al. Protothecosis: report of a case with 20-year follow-up, and review of previously published cases. Med Mycol 2012;50:673-689
Google Scholar
10. Kwon-Chung KJ. Phylogenetic spectrum of fungi that are pathogenic to humans. Clin Infect Dis 1994;19 Suppl 1:S1-7
Google Scholar
11. Chao SC, Hsu MM, Lee JY. Cutaneous protothecosis: report of five cases. Br J Dermatol 2002;146:688-693
Google Scholar
12. Woolrich A, Koestenblatt E, Don P, Szaniawski W. Cutaneous protothecosis and AIDS. J Am Acad Dermatol 1994;31:920-924
Google Scholar
13. Kim ST, Suh KS, Chae YS, Kim YJ. Successful treatment with fluconazole of protothecosis developing at the site of an intralesional corticosteroid injection. Br J Dermatol 1996;135:803-806
Google Scholar
14. Pfaller AA, Diekema DJ. Unusual fungal and pseudofungal infections of humans. J Clin Microbiol 2005; 43:1495-1504
Google Scholar
15. Kim JA, Moon SE, Song KY. Two cases of cutaneous protothecosis: unique histopathological findings with crystal violet staining and the therapeutic effect of itraconazole. Ann Dermatol 1997;9:201-207
16. Kantrow SM, Boyd AS. Protothecosis. Dermatol Clin 2003;21:249-255
17. Zhang QQ, Li L, Zhu LP, Zhao Y, Wang YR, Zhu JH, et al. Cutaneous protothecosis in patient with diabetes mellitus and review of published case reports. Mycopathologia 2012;173:163-171
Google Scholar
18. Seok JY, Lee Y, Lee H, Yi SY, Oh HE, Song JS. Human cutaneous protothecosis: report of a case and literature review. Korean J Pathol 2013;47:575-578
Google Scholar
19. Moon HS, Lee HK, Park K, Chae JD, Son SJ. A case of cutaneous protothecosis. Kor J Med Mycol 2007; 12:70-74
Google Scholar
